Detecting dystonia in general practice
Movement disorders
Neuromuscular disorders
Dystonia is an under-recognised movement disorder, characterised by involuntary twisting movements and postures. Diagnosis and treatment are often delayed. Early referral to a movement disorder neurologist is recommended to initiate treatment for this disabling condition.
Linked videos
There are four videos available for this article, which can be accessed here.
- Dystonia may affect a single body part and fluctuate in its manifestations, both between consultations and during the consultation – affected patients may easily be mistaken as having a psychogenic illness or being ‘worried well’.
- Dystonia may be functionally disabling, even when only a single body part is affected (e.g. involuntary eye closure or neck turning that prevents driving).
- Safe and effective treatment is available for focal dystonia in the form of botulinum toxin injections every two to three months – referral to a neurologist is recommended.
- Antidopaminergic antiemetic (e.g. metoclopramide, prochlorperazine) and antipsychotic (e.g. haloperidol, risperidone) medications are an important cause of tardive dystonia. These medications should be prescribed with care as long-term exposure can cause permanent and disabling tardive dystonia.
Picture credit: © Science Source/George Mattei/Diomedia.com Model used for illustrative purposes only
The diagnosis of dystonia has recently been revised to ‘a movement disorder characterised by sustained or intermittent muscle contractions causing abnormal, often repetitive, movements, postures, or both. Dystonic movements are typically patterned, twisting, and may be tremulous. It is often worsened by voluntary action and associated with overflow muscle activation.’1
Dystonia varies widely in distribution and severity, ranging from focal presentations affecting a single body part (e.g. torticollis) to severe generalised dystonia affecting the whole body, as encountered in patients with cerebral palsy. Although dystonia is uncommon, recognition in general practice is important as safe and effective treatments are available for this disabling problem. Moreover, patients may have symptoms that sound non-neurological (e.g. neck pain, dry eyes), leading to diagnostic delay while undergoing investigations and treatment from another clinical specialty. In a Canadian survey, patients on average waited five years and saw three physicians before receiving a diagnosis of dystonia, with about 40% given a diagnosis of ‘stress’ at some stage.2
The difficulty in recognising dystonia is unsurprising as the features on examination may be variable. Dystonia was previously thought to be psychogenic in origin, a view which changed in recent decades following the identification of genetic causes and consistent neurophysiological findings. Awareness of the classic symptoms and presentation of the common forms of dystonia and techniques for examination will allow GPs to recognise and diagnose dystonia.
In this review we focus on the common forms of dystonia that may be encountered in general practice, with special emphasis on the key features that enable GPs to diagnose these disorders, as well as principles of treatment. We highly recommend referring to the online supplementary videos which show examples of some common forms of dystonia described in the text (see http://medicinetoday.com.au/dystoniavideos).
What are the key features of dystonia?
Dystonia is a clinical syndrome consisting of the abnormal movements generated by inappropriate muscle contraction. These muscle contractions may be sustained or intermittent and may be confused with other abnormal movements such as tremor (seen in essential tremor and Parkinson’s disease), chorea (seen in Huntington’s disease) or tics (seen in Tourette’s syndrome). The intermittent nature of abnormal muscle contractions was a key part of Oppenheim’s original description of dystonia, when he was struck by the fact that patients have hypotonia at some times (especially at rest) and hypertonia at others.3
There are a few key features that can help in the identification of an abnormal movement as dystonia.
- Dystonia typically occurs on action or during movement.
- Dystonic movements cause twisting and sustained posturing of affected body parts.
- Dystonic muscle contraction may spread to adjacent muscles not normally involved in the task (‘overflow’). For example, when writing there may be abduction of the shoulder in focal arm dystonia (writer’s cramp).
- Dystonic movements often repeat in a particular (stereotyped) pattern. Common examples include head turning in a particular direction or inversion of the foot during walking.
- Dystonic movements may be accompanied by tremor.
- Dystonic movements may be suppressed by a change in sensory input such as a light touch or the action of an adjacent body segment, known as a geste antagoniste. Common examples include the patient lightly placing their hand on their chin to relieve head turning in torticollis, chewing gum to relieve blepharospasm and oromandibular dystonia, and altering pen shape and size in writer’s cramp. Historically, this phenomenon was used as evidence for the psychogenic nature of dystonia (which has since been disproven) but is now recognised as a useful clue to distinguish dystonia from other abnormal movements.4
- Dystonic movements may sometimes emerge only during certain skilled tasks or activities. The most common examples are writer’s cramp and musician’s dystonia, where the hand adopts an abnormal posture when writing or playing a musical instrument, respectively, impairing performance.5 This unusual and unique symptomatology was also used as evidence for a psychogenic aetiology (which has since been disproven).6 When a patient complains of difficulty with a skilled motor task such as writing, it is important to observe them perform the task and look for evidence of excessive muscle contraction and dystonic postures.
- It should be noted that the absence of task specificity or geste antagoniste does not exclude the diagnosis of dystonia.
How common is dystonia?
Determining the prevalence of dystonia is difficult because many cases are undiagnosed. A meta-analysis of service-based studies estimated that the prevalence of primary dystonia is 16 per 100,000 people, but this figure was substantially lower than that estimated by population-based studies, which ranged from 40 to 700 per 100,000 people.7
What causes dystonia?
Like other movement disorders (e.g. tremor), dystonia may occur as the result of a broad range of different aetiologies (e.g. genetic, metabolic, stroke, perinatal injury, traumatic, drug-induced, idiopathic). The common factor in these different aetiologies is the involvement of the basal ganglia, although more recent evidence also implicates the cerebellum and cerebral cortex as potentially being involved in dystonia.8
The evidence for neuroanatomical localisation of dystonia to the basal ganglia is strong, and is illustrated by the association between basal ganglia pathology and dystonia, imaging studies (positron-emission tomography, functional MRI, voxel-based morphometry, diffusion tensor imaging) and the therapeutic effects of deep brain stimulation to the basal ganglia in the treatment of dystonia.9
Dystonia classification and terminology
The classification of dystonia has evolved with time, with variable and often confusing terminology appearing in the literature. Some of the common terminology used in classifying dystonia is summarised in Table 1.
{kind=link}
Common and important types of dystonia
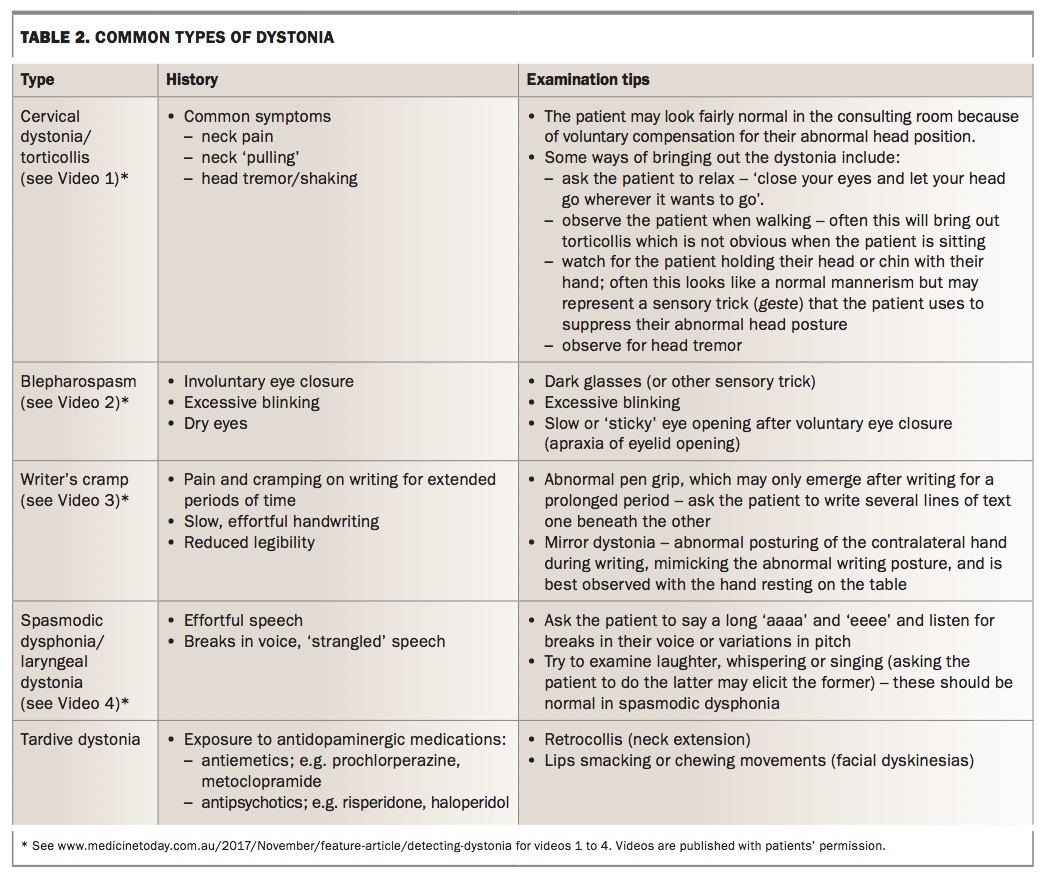
Table 2 provides a summary of the key clinical features and examination tips for common types of dystonia.
{kind=link}
Focal dystonia
Torticollis (cervical dystonia)
Idiopathic cervical dystonia, also known as (spasmodic) torticollis, is the most common type of focal dystonia, with an estimated prevalence of five per 100,000 people.7 It is more common in women (3:1 ratio) and has an average age of onset of 45 years.10 It often begins with subtle head turning or head tremor which worsens slowly with time. Patients may describe an abnormal head position or tremor, but also commonly complain of neck pain, stiffness or cramp, which often lead them to seek attention from physical or alternative therapies before seeing their GP.11
Patients may use a geste manoeuvre to suppress the movement (see Video 1). Cervical dystonia may cause significant disability through interference with driving (due to limitations in neck movement) and distress in social situations. In longstanding cases it may even cause damage to the cervical spine and myelopathy. Botulinum toxin injected into affected muscles at three-monthly intervals is the first-line treatment, but deep brain stimulation may be required in severe, refractory cases.
Blepharospasm
Blepharospasm is a focal dystonia characterised by spasm of the orbicularis oculi muscle and other muscles around the eyes manifesting as involuntary blinking and prolonged eye closure. Like cervical dystonia, it is more common in women. The peak age of onset is in the sixth decade of life.12 In addition to excessive blinking and involuntary eye closure, sensory symptoms such as dry eyes, a burning sensation or grittiness of the eye, and light sensitivity (photophobia) are common.12 During the examination, the following may be observed:
- excessive bilateral symmetrical blinking (in contrast to hemifacial spasm in which one eye is affected)
- prolonged spasm of eye closure
- a sensory trick
- dystonia elsewhere, in particular the lower face and neck (Meige syndrome; see Video 2).
First-line treatment is botulinum toxin injection. Deep brain stimulation has been used with success in patients with more widespread dystonia.12
Writer’s cramp
Writer’s cramp is a focal dystonia that affects the patient’s dominant arm and hand, and is caused by abnormal muscle contraction and postures when writing. First described in the 19th century and prominently affecting scribes in Victorian London (so called ‘Scriveners’ palsy’), this condition (like other dystonias) was for a time thought to be a psychogenic disease before being recognised as an organic condition.13 Patients may describe cramp or pain in the hand on writing, tremor or painless clumsiness or deterioration in their handwriting.13
Examination findings may be subtle and include abnormal pen grip and posturing of the hand on writing, as well as ‘mirror movements’ of the other hand
(see Video 3). About 30% of patients have tremor (dystonic tremor) on holding
the arm outstretched. Treatment with botulinum toxin has been proven in randomised controlled trials to be beneficial, but it is not currently subsidised on the PBS for this indication (off-label use); oral medications are sometimes used but may have side effects and the evidence is weaker.14
Spasmodic dysphonia (laryngeal dystonia)
Spasmodic dysphonia is a rare dystonia affecting the larynx. Patients find speech an effort and experience involuntary breaks in their voice and variation in pitch during speech due to vocal cord spasm. The voice may take on a different quality depending on whether the cord adductors (‘tight voice’) or abductors (‘breathy voice’) are primarily affected. Like other focal dystonias, spasmodic dysphonia may be task specific, occurring during spontaneous speech, whereas other vocal tasks (e.g. laughing, shouting, whispering or singing) are spared (see Video 4). This is in contrast to other more common causes of voice dysfunction which affect all vocal tasks.
Diagnosis is commonly delayed with patients being treated for anxiety or reflux.15 The diagnosis can be confirmed with nasolaryngoscopy and treated with botulinum toxin (which is not PBS subsidised for this indication).16 Spasmodic dysphonia may coexist with dystonia affecting the neck and face (Meige syndrome).
Generalised dystonia
Generalised dystonia, involving multiple body regions, has a broad range of potential aetiologies, including genetic (inherited) dystonia, metabolic and structural brain insults and perinatal brain injury (cerebral palsy). Further discussion of these dystonias is beyond the scope of this review.
The discovery of various genetic mutations causing dystonia was a key factor in the reclassification of dystonia, confirming an organic basis.17 Treatment involves several medications, often in combination, and sometimes deep brain stimulation. Botulinum toxin has a lesser role because it is impractical to inject all of the (many) affected muscles, but may be of use for particularly troublesome focal symptoms.
Drug-induced dystonia
Several medications may cause temporary or permanent dystonia. Tardive dystonia deserves special mention.
Tardive dystonia
Dopamine receptor-blocking medications may cause several movement disorders, commonly referred to as tardive dyskinesia, but which may have dystonia as the predominant feature. Classic causative medications include:
- antipsychotics (e.g. haloperidol, risperidone)
- antiemetics (e.g. prochlorperazine, metoclopramide)
- antihistamines (e.g. cinnarizine)
Young men are particularly vulnerable to tardive dystonia, and the classic clinical features include neck extension (retrocollis), trunk hyperextension (opisthotonus) and orofacial dystonia including blepharospasm and tongue protrusion.18 Treatment is challenging because withdrawal of the causative medication provides remission in only 11 to 14%,19,20 and sometimes deep brain stimulation is used for patients with severe generalised tardive dystonia – specialist input is important.
Although long-term antipsychotic treatment may be difficult to avoid in some patients (e.g. those with schizophrenia), GPs should exercise care and avoid long-term prescribing of dopamine receptor-blocking antiemetics to avoid this potentially severe and permanent side effect.
What tests should GPs consider arranging?
In the absence of other clinical features, brain MRI has a low yield in patients with classic focal dystonia (e.g. isolated cervical dystonia with onset in middle age) and is not routinely required. However, brain imaging is a useful starting point when other signs are present in focal, generalised or combined dystonia and especially in hemidystonia. In addition to routine tests such as full blood count and biochemistry, testing for Wilson’s disease with measurement of serum copper and caeruloplasmin levels and 24-hour urinary copper collection is useful because this is a treatable aetiology that may present at almost any age.21
When to consider referral
Referral to a movement disorder neurologist is recommended for all patients with a new presentation of dystonia.
Treatment of dystonia
In focal and generalised dystonia where a secondary cause has not been identified, treatment is focused on relieving symptoms rather than modifying the underlying disease process. There are a few important exceptions to this principle.
- Tardive or drug-induced dystonia. Avoidance of the offending agent may be an important part of management. It should be noted that withdrawal of antipsychotic medication from a patient with chronic schizophrenia may not be advisable because of the risk of worsening their psychiatric state.22
- Wilson’s disease. Copper-chelating drugs are an important part of therapy to prevent further copper accumulation and may lead to resolution of neurological symptoms.
In general, botulinum toxin is the therapy of choice for focal dystonia (or dystonia where only a few muscles are producing most of the disability). Oral medications and deep brain stimulation are preferred for patients with generalised dystonia.
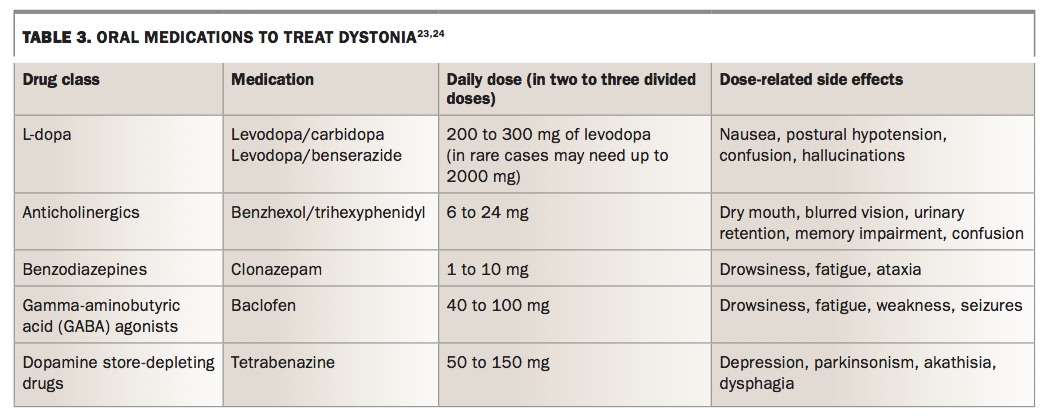
Oral medications
Several different medications are used to treat dystonia (Table 3).23,24 Benefits are modest and these medications may be poorly tolerated particularly in adult patients.
{kind=link}
Botulinum toxin
Botulinum toxin is a potent biological toxin produced by the Clostridium bacteria and is subsidised on the PBS for use in cervical dystonia hemifacial spasm and blepharospasm. It acts primarily by inhibiting the release of acetylcholine at the presynaptic terminal, thus preventing neuromuscular transmission and causing muscle weakness. Small doses of botulinum toxin are injected into affected muscles (often using electromyography or ultrasound guidance) to reduce dystonic muscle activity and alleviate symptoms. The therapeutic effects of botulinum toxin take five to seven days to start and usually last for two to three months. Most patients have repeat injections at three-monthly intervals.
This treatment is safe, effective and has been used for more than 20 years. Side effects of weakness of the injected muscle are transient because the toxin effect wears off after two to three months. Uncommon side effects from weakness due to excessive dose or spread of toxin beyond its injection site may include:
- dysphagia, head drop (after injecting neck muscles for cervical dystonia)
- ptosis (after injecting the orbicularis oculi muscle for blepharospasm)
- hand weakness (if distal muscles are injected for writer’s cramp)
- flu-like symptoms have been reported in 14% of patients within 24 hours of a botulinum toxin injection.25
Deep brain stimulation
Ablative surgical treatments of dystonia targeting the internal segment of the globus pallidus of the basal ganglia have been used for decades. More recently, deep brain stimulation, involving the delivery of pulsatile electric stimuli to the basal ganglia via implanted electrodes, has supplanted lesioning surgery. There is strong randomised evidence for this treatment, which is usually reserved for generalised or medically-refractory dystonia.26 The benefit of deep brain stimulation targeting the globus pallidus may take six to 12 months after the surgery to take full effect.
Conclusion
Dystonia is a treatable movement disorder that is under-recognised and undertreated. Early recognition of dystonia in primary care and early referral to a movement disorder neurologist can prevent unnecessary specialist reviews and reduce disability by offering early treatment options. MT