Chronic hepatitis B: a continually evolving disease

Hepatitis
Chronic hepatitis B virus infection is the most common liver infection in the world, with high prevalence rates in at-risk communities in Australia. The main goal of treatment is to reduce the risk of developing liver cancer. Lifelong monitoring of disease progression and screening for early liver cancer are required whether or not the patient is receiving drug therapy.
Chronic hepatitis B virus infection is the most common liver infection in the world, with high prevalence rates in at-risk communities in Australia. The main goal of treatment is to reduce the risk of developing liver cancer. Lifelong monitoring of disease progression and screening for early liver cancer are required whether or not the patient is receiving drug therapy.
Remember
- Chronic hepatitis B virus (HBV) infection affects more than 400 million people globally, and its prevalence varies greatly in different regions.
- Although Australia and New Zealand have low prevalence rates of less than 1%, some communities recognised as being at risk, including Indigenous people and immigrants from South-East Asia, Pacific islands, Southern Europe, the Mediterranean region and Africa, have much higher prevalence rates (six- to 12-fold increased prevalence).1
- Countries with higher intermediate prevalence rates include China, with an estimated 5.49% of the population affected by chronic HBV infection. Particular efforts must be made to not overlook such population groups with regard to screening and surveillance.2
Natural history of hepatitis B virus infection
- Chronic HBV infection has a dynamic course ranging from an immune tolerance/control phase to one of active liver disease and inflammation with immune clearance/escape that may evolve to cirrhosis and hepatocellular carcinoma (HCC).3-5
- Progression through fibrosis to cirrhosis is variable and can occur rapidly.
- Fibrosis and even cirrhosis may be reversible with treatment.
Long-term outcome of chronic HBV infection
- The cumulative five-year incidence of cirrhosis is 8 to 20% in adults with untreated chronic HBV infection.6 Of the patients with compensated cirrhosis, the five-year cumulative risk of decompensation is 15 to 20% and the risk of HCC is 2 to 5%.6,7
- Viral determinants of disease progression include a high viral load, the hepatitis B genotype and coinfection with hepatitis C virus or HIV. Male sex, advancing age and a family history of HBV-related complications increase the risk of disease progression. Other contributors are environmental factors such as alcohol consumption, tobacco smoking and nonalcoholic fatty liver disease.8
Assessment
- Targeted screening for chronic HBV infection is recommended for high-risk groups to increase case finding and provide linkage of care. Where indicated, drug therapy and cancer surveillance improves outcomes.9
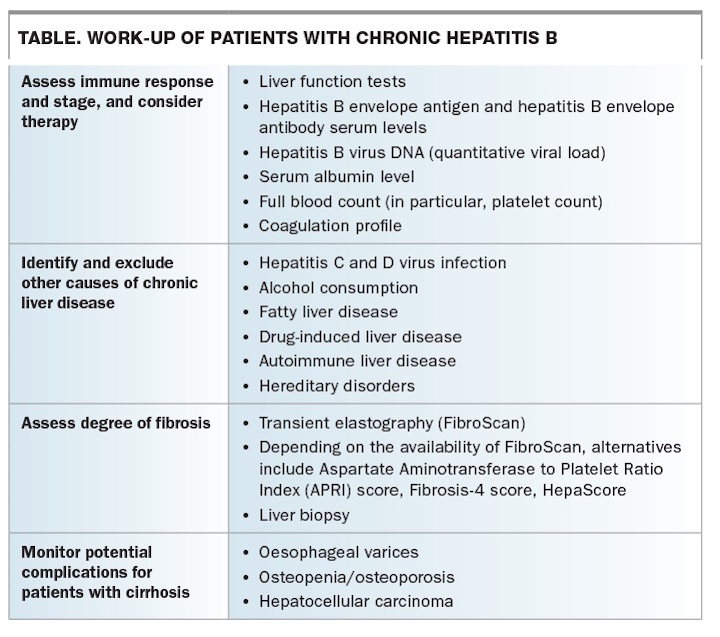
- Chronic HBV infection is confirmed by the presence of hepatitis B surface antigen (HBsAg) for at least six months. HBV DNA is tested to confirm replication status and to assist in considering treatment options. Staging of the disease is performed using blood tests and imaging. Where available, FibroScan provides a quick, noninvasive measure of the degree of cirrhosis (Table).
{kind=link}
Management
- The goal of management for patients with chronic HBV infection is to prevent or reverse cirrhosis and reduce the risk of HCC.10
- Treatment is initiated in the immune clearance and immune escape phases depending on evidence of inflammation and fibrosis.
- Chronic HBV cannot be ‘cured’ because HBV DNA is integrated into the human hepatocyte DNA.
- HBsAg loss and seroconversion is considered a complete response but is infrequently achievable with currently available treatment agents.11
- A more realistic endpoint of treatment is HBV DNA at undetectable levels (<15 IU/mL) to prevent progressive liver injury.12
Pharmacological agents
- Current first- and second-line therapies that are PBS listed include nucleoside/nucleotide analogues such as entecavir and tenofovir, and peginterferon alfa-2a.
- The advantages of peginterferon alfa-2a include defined treatment duration, no antiviral resistance and the durability of hepatitis B envelope antigen seroconversion. However, its side effects can be limiting and use of peginterferon alfa-2a in patients with advanced liver cirrhosis (a Child–Pugh score of B or C) is contraindicated.11
- Nucleoside/nucleotide analogues are safe in advanced cirrhosis and have minimal side effects, but long-term treatment is often required and patients may develop resistance.6
- Numerous new potential therapies are currently being trialled for use in patients with chronic HBV infection. These include therapeutic vaccines for chronic HBV and a newer version of tenofovir, tenofovir alafenamide, that has fewer renal and bone side effects. Tenofovir alafenamide is TGA approved but not PBS listed for treating patients with chronic HBV.
Monitoring and surveillance
- Monitoring of patients with chronic HBV infection should include liver function tests every six months and annual HBV DNA viral load testing. More frequent monitoring may be needed if clinically indicated, especially in patients on antiviral treatment.13
- Surveillance among patients who are at risk for HCC requires abdominal ultrasound every six months.14
Special populations
- Patients with special considerations, such as those who are pregnant or have coinfections with hepatitis C virus or HIV, should be managed together with a specialist with expertise in the relevant field.
Conclusion
- Chronic HBV infection has a complex, dynamic natural history that can progress to cirrhosis and HCC and requires lifelong monitoring.
- Where indicated, therapy can reverse advanced disease and reduce the risks of complications. Potent viral suppression is achieved with antiviral therapy, which is likely to be required long term. Antiviral therapy is safe and highly effective with low rates of significant side effects and resistance.
- Surveillance for HCC is recommended in patients whose risk is increased.
Competing interests: None.
References
- Tawk HM, Vickery K, Bisset L, Lo SK, Selby W, Cossart YE; Infection in Endoscopy Study Group. The current pattern of hepatitis B virus infection in Australia. J Viral Hepat 2006; 13: 206-215.
- Schwetzer A, Horn J, Mikolajczyk R, Krause G, Ott J. Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet 2015; 386: 1546-1555.
- Fattovich G. Natural history and prognosis of hepatitis B. Semin Liver Dis 2003; 23: 47-58.
- Gastroenterological Society of Australia - Digestive Health Foundation. Australian and New Zealand chronic hepatitis B (CHB) recommendations. 2nd ed. Melbourne: Digestive Health Foundation, Gastroenterological Society of Australia; 2009/10.
- Patullo V, Strasser SI. Managing the rising burden of chronic liver disease: chronic hepatitis B and C. Med Today 2017; 18(2): 34-42.
- Terrault NA, Bzowej NH, Chang KM, et al; American Association for the Study of Liver Diseases. AASLD guidelines for treatment of chronic hepatitis B. Hepatology 2016; 63: 261-283.
- Fattovich G, Bortolotti F, Donato F. Natural history of chronic hepatitis B: special emphasis on disease progression and prognostic factors. J Hepatol 2008; 48: 335-352.
- Ganem D, Prince AM. Hepatitis B virus infection: natural history and clinical consequences. N Engl J Med 2004; 350: 1118-1129.
- Hutton DW, Tan D, So SK, Brandeau ML. Cost-effectiveness of screening and vaccinating Asian and Pacific Islander adults for hepatitis B. Ann Intern Med 2007; 147: 460-469.
- Lok AS, Heathcote EJ, Hoofnagle JH. Management of hepatitis B: 2000 – summary of a workshop. Gastroenterology 2001; 120: 1828-1853.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: management of chronic hepatitis B. J Hepatol 2009; 50: 227-242.
- Lai CL. Therapeutic advances in chronic hepatitis B. J Gastroenterol Hepatol 2004; 19 Suppl: S5-S9.
- McMahon BJ. The natural history of chronic hepatitis B virus infection. Semin Liver Dis 2004; 24 Suppl 1: 17-21.
- Bruix J, Sherman M; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology 2011; 53: 1020-1022.