Management of red cell antibodies in pregnancy

Health problems in pregnancy
Infant and newborn care
An early blood group and antibody screen for maternal red cell antibodies is a standard component of pregnancy management. In proven alloimmunisation, a thorough obstetric and medical history is important. Women with fetuses at high risk of developing fetal anaemia require referral to a maternal–fetal medicine specialist for close antenatal ultrasound surveillance.
- About 1% of pregnant women carry a red cell antibody that has the potential to destroy fetal red blood cells and cause fetal anaemia (alloimmunisation).
- The three most clinically important antibodies in alloimmunisation are Rhesus D, Rhesus c and Kell antibodies.
- Alloimmunised pregnant women whose antibody levels exceed a certain critical threshold are at high risk of their baby developing fetal anaemia and warrant prompt referral to a maternal–fetal medicine specialist.
- Regular in utero ultrasound assessment of the fetal middle cerebral artery is a very sensitive method of detecting anaemia in the fetus of women with high-risk red cell antibodies.
- A fetus that becomes anaemic before 34 weeks’ gestation may require a life-saving in utero fetal transfusion.
- After birth, babies are at increased risk of anaemia and jaundice, which are the neonatal effects of haemolysis.
Picture credit: © Phaine/Burger/Diomedia.com Models used for illustrative purposes only
In Australia it is recommended that all pregnant women have a blood group and antibody screen performed early in pregnancy to look for red cell antibodies. When this test confirms a maternal antibody, it can be challenging to understand its significance and what additional measures are needed to safely care for the pregnancy. This review provides a broad overview of alloimmunisation in pregnancy so that GPs can offer safe antenatal care to women with this condition. It also discusses when it is appropriate to refer alloimmunised women to specialist care.
Alloimmunisation - what is it?
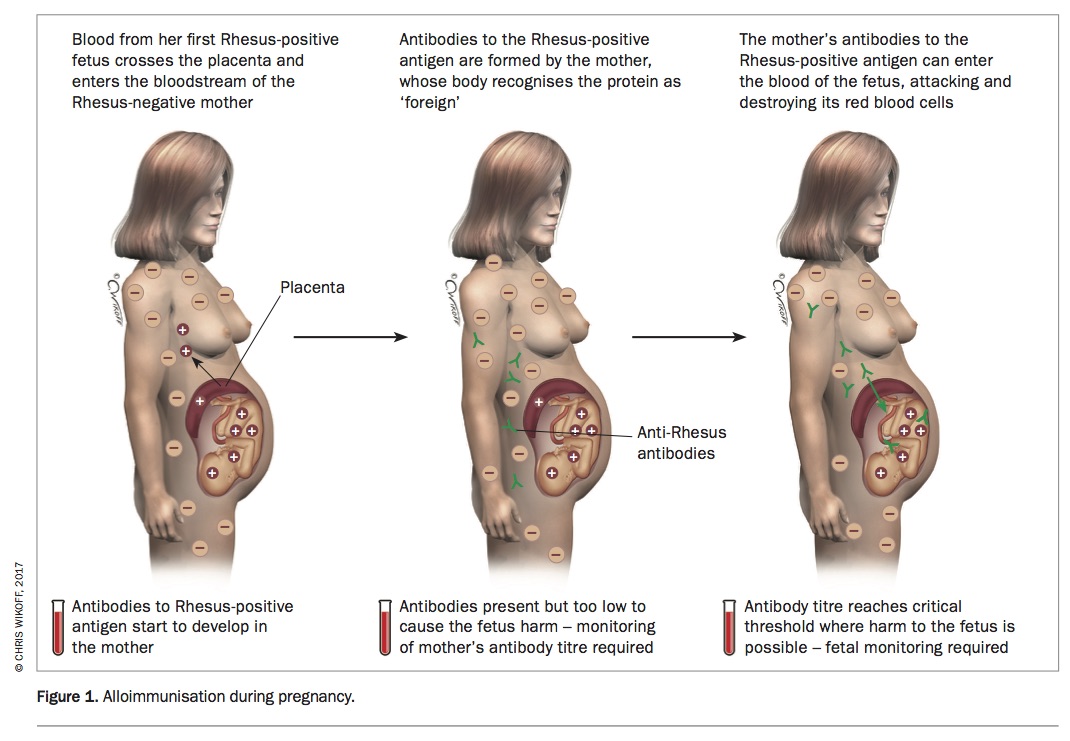
In addition to the four major blood groups (O, A, B and AB), each red blood cell is coated with several different sugars and proteins (antigens). A baby’s blood group is determined genetically by the blood groups of its parents, so the blood groups of the mother and baby are not identical. During pregnancy, some fetal red blood cells normally cross the placenta into the maternal circulation. If the fetal red cells possess ‘foreign’ antigens, the mother’s immune system forms antibodies, just as it would do against the antigens of bacteria or viruses. These red cell antibodies have the potential to cross back over the placenta and attack the fetal red cells, causing haemolysis (Figure 1). This process is called alloimmunisation (previously termed isoimmunisation) and affects 1% of pregnancies.1,2
{kind=link}
Common red cell antibodies seen in pregnancy
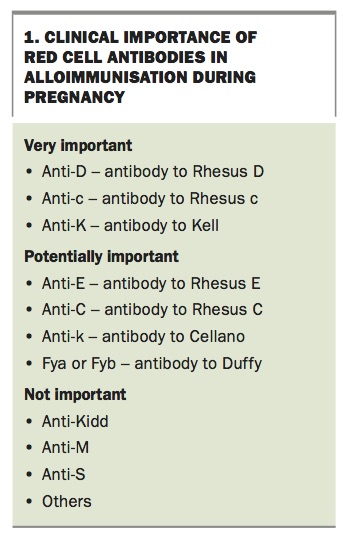
Although more than 50 different red cell antigens have been described, most are not clinically relevant in pregnancy. Antigens are clustered into families and the most important families in pregnancy are the Rhesus (Rh) and Kell (K) systems. Antibodies from other families – such as the MNS system, and Duffy and Kidd systems – rarely cause serious problems in pregnancy.3 Box 1 summarises the red cell antibodies that are important for managing alloimmunisation in pregnancy.
{kind=link}
Rhesus antibodies
The main Rhesus antigen on the red blood cell is the ‘D’ antigen, which is usually written as Rh(D). When we refer to a patient’s blood group as ‘A positive’ or ‘O negative’, this is really shorthand for ‘A Rh(D) positive’ or ‘O Rh(D) negative’. The other important Rhesus antigens are c, C, e and E (in alloimmunisation small and capital versions of a letter denote different antigens and this is an important distinction). The maternal antibodies formed against the fetal Rhesus antigens are referred to as anti-D, anti-c, anti-C, anti-e and anti-E antibodies.
‘Anti-D’ – an antibody and a treatment
The term ‘anti-D’ can be confusing as it refers to both the maternal antibody that is responsible for Rhesus D alloimmunisation and to the prophylactic treatment offered to women antenatally. In Australia, about 17% of women are Rhesus D negative but prevalence does vary with ethnicity.4 Pregnant women whose blood group is Rhesus D negative and who are not yet alloimmunised are offered an injection of Rhesus D immunoglobulin – known as the ‘anti-D injection’ – at 28 and 34 weeks’ gestation and also following any potentially sensitising event. This prevents maternal alloimmunisation and has been a remarkably successful public health initiative globally. In essence, a small dose of anti-D antibody is injected, to ‘mop up’ any fetal Rhesus D-positive cells and prevent the mother’s immune system forming her own antibodies.
Kell antibodies
The other family of red cell antigens that often causes serious alloimmunisation is the Kell (K) family (Box 1). Pregnant women with Kell antibodies need to be monitored particularly closely because the risk to the fetus is more unpredictable.
The most common antigen from this family is the K antigen (often simply referred to as ‘Kell’). Less frequently, a related antigen – termed k (little-k) or Cellano – may also be encountered. (The names of these Kell antibodies are derived from the surnames of the women in whom they were first detected.)
Antenatal testing for alloimmunisation
Each of us inherits two copies of every red cell antigen – one copy from each of our parents. For the Rhesus c antigen for example, we might inherit two copies of ‘little-c’ (cc), two copies of ‘big-c’ (CC) or one of each (Cc), depending on our own parents’ Rhesus c status. Rather confusingly, there is no ‘little-d’ – we either inherit the Rhesus D antigen or we do not.
The whole basis of alloimmunisation is an underlying incompatibility between the blood groups of the mother and the fetus. The fetus is only vulnerable to a maternal antibody if it carries the related antigen so knowing the mother’s and baby’s blood groups should make prediction of alloimmunisation fairly straightforward. However, the problem is that the baby’s blood group is usually not known until after birth. The best we can do antenatally is to test the blood groups of both parents to try and predict what red cell antigens the baby might possess.
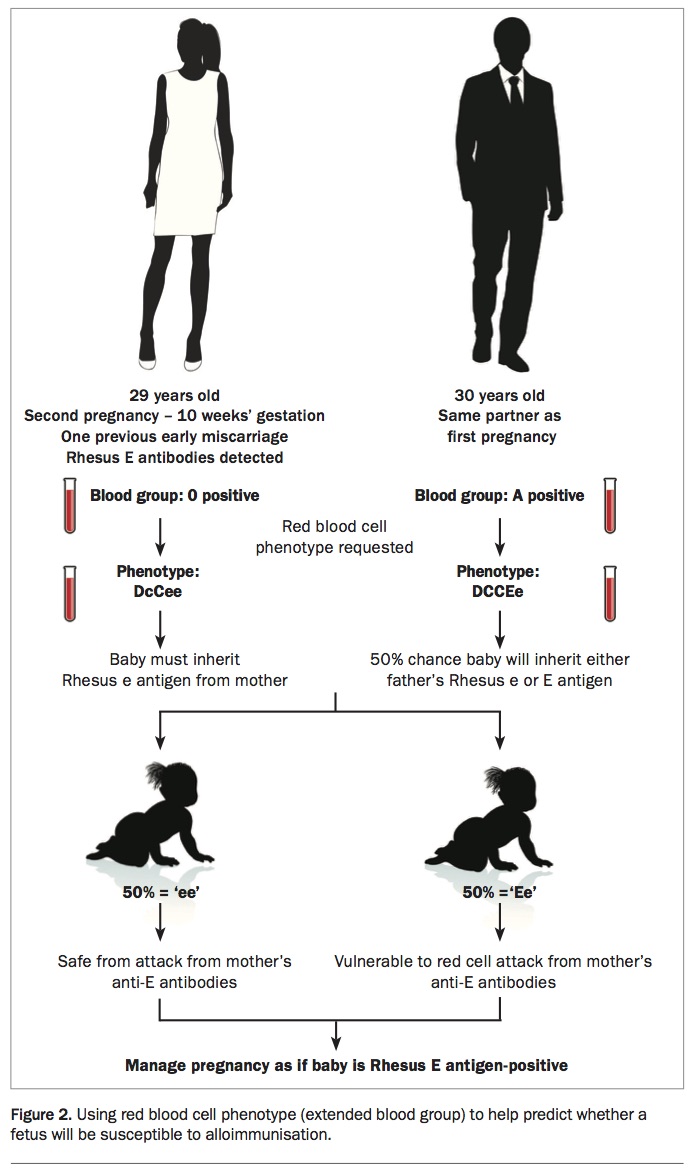
Any adult may be referred to a pathology centre for a simple blood test to check their ‘red blood cell phenotype’ (the extended blood group). This is often indicated for the partner of an alloimmunised pregnant woman because even if her partner knows his blood group is A positive for instance, it does not help us if the woman has red blood cell antibodies – anti-E for example. In this case, the partner’s extended blood group needs to be requested. By testing his extended blood group, we can see whether the woman’s partner carries the Rhesus E antigen and can predict whether the baby might be susceptible to alloimmunisation (Figure 2).
{kind=link}
Complications of alloimmunisation
Alloimmunisation is responsible for a disorder called haemolytic disease of the fetus and newborn (HDFN). Previously this was referred to as HDN, but the term has evolved to reflect the fact that babies can be affected in utero as well as in early neonatal life. The underlying mechanism is an immune-mediated attack of the fetal red blood cells by maternal antibodies.
- In a fetus this leads to fetal anaemia that, if left untreated, can progress to high-output heart strain, fetal hydrops (heart failure) and eventually, death.
- In a newborn infant this typically manifests as moderate to severe jaundice that can progress to neurological impairment and hearing loss if left untreated.
Risk of HDFN
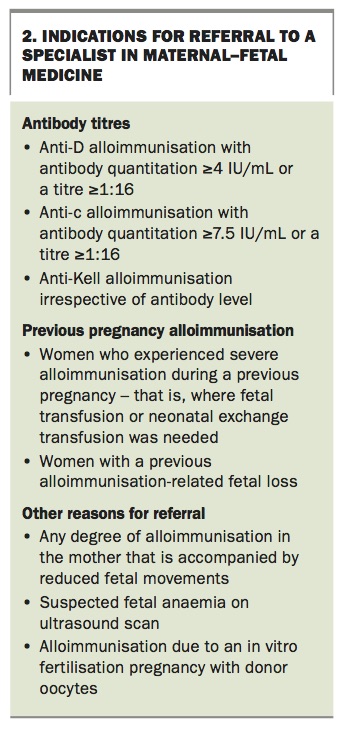
The risk of HDFN depends on three factors: which particular antibody is involved; how much antibody is in the maternal circulation; and whether a previous baby was affected. Box 2 highlights when referral to a maternal–fetal medicine specialist is warranted due to a high risk of HDFN.
{kind=link}
Which antibody
The vast majority of HDFN is due to one of three antibodies – anti-D, anti-c and anti-Kell (K) (Box 1). One large study found that 100% of women requiring an in utero fetal transfusion for severe alloimmunisation had one of these three antibodies.5
How much antibody
A fetus is only at risk of severe anaemia if the antibody levels in the mother’s blood reach a certain critical threshold, which is different for each antibody (Box 2).6 Traditionally, antibody levels are reported by the laboratory in titres (e.g. titre = 8). The titre is the number of times a blood sample must be diluted before the antibody is rendered undetectable; for example, a titre of 32 means there is a higher concentration of antibody present than a titre of 8. It has now become possible to quantify antibody levels directly using flow cytometry so the quantity is then reported in IU/mL. This newer technology means results are less variable between laboratories. However, it is often only available in national blood banks such as the Red Cross and the seven- to 10-day turnaround time for results can limit its clinical usefulness.
Previous baby affected by alloimmunisation
In certain circumstances alloimmunised women should always be referred to a maternal–fetal medicine specialist as the normal rules between antibody levels and risk of HDFN do not apply and expert input is required (Box 2). This includes women who:
- have high Rhesus D or Rhesus c antibody levels or Kell antibodies of any level
- required fetal transfusion in a previous pregnancy or experienced a previous fetal loss thought to be secondary to alloimmunisation
- had a previous baby who developed severe neonatal haemolytic disease requiring exchange transfusion.
Managing women who have red cell antibodies during pregnancy
Take a thorough obstetric and medical history
For a woman’s immune system to become alloimmunised, she must be exposed to a foreign red cell antigen. This is usually a paternally derived antigen carried by the fetus during a previous pregnancy. In cases of Kell alloimmunisation, it is frequently due to a previous blood transfusion. It is therefore vital to obtain a clear history of:
- previous pregnancies including miscarriages
- previous blood transfusions
- antibody screening results from prior pregnancies
- occurrence of jaundice in previous babies.
Check the partner’s red blood cell phenotype
For most women, the partner’s red cell phenotype should be obtained. This allows prediction of the possible antigen status of the baby and whether the current fetus is potentially at risk. If the partner does not carry the equivalent antigen it cannot be passed onto the baby and the risk of HDFN is zero. Of course, partner testing assumes paternity, which is a very sensitive topic. It also requires the partner to be available and agreeable to testing.
Consider non-invasive testing of fetal Rhesus D status if appropriate
Non-invasive prenatal testing for fetal chromosomal disorders is now widely available in Australia. What most clinicians are not aware of is that the same technology has been utilised to check the Rhesus status of a fetus for more than a decade. Currently in Australia testing is only available for the Rh(D) antigen although non-invasive testing of fetal Kell, Rh(E) and Rh(c) is available overseas. Testing for Rhesus D in Australia is undertaken in the Red Cross laboratory in Queensland. If a woman is found to carry anti-D antibodies and her partner is Rhesus D antigen positive, a maternal blood sample can be sent on ice to the Red Cross. Non-invasive testing can confirm whether the fetus is Rhesus D positive or negative. If the fetus is found to be Rhesus D negative, there is no risk of HDFN and no further monitoring is necessary.
Arrange serial monitoring of maternal antibody levels
Women with confirmed red cell antibodies and a fetus that is potentially antigen-positive should have their antibody levels checked every four weeks until 28 weeks and then every two weeks until delivery (maternal antibody levels are more likely to rise towards term). Women whose antibody levels reach the critical threshold for that antibody need prompt referral to a maternal–fetal medicine specialist for regular ultrasound surveillance.
With Rhesus D and Rhesus c alloimmunisation the antibody level correlates closely with the risk of HDFN because the disorder is due purely to red cell haemolysis. This means that women with very high antibody levels of these antigens can be monitored more intensively, while women with low antibody levels can be reassured. However, Kell antibodies cause fetal bone marrow suppression as well as direct haemolysis, which can cause a more severe type of fetal anaemia earlier in the pregnancy. The HDFN risk does not correlate well with Kell antibody levels and all women with Kell alloimmunisation require referral to a specialist in maternal–fetal medicine (Box 2).7
Planning the delivery and baby after-care
The baby is only at risk of ongoing allo- immunisation while it is exposed to the maternal antibodies, which is during pregnancy. Following delivery, the source of the problem is removed although the baby can still experience some after effects of haemolysis in early neonatal life. The neonate may be anaemic and jaundiced and may require prompt treatment (phototherapy, top-up transfusion or even exchange transfusion). In some centres, neonatal intravenous immunoglobulin therapy is utilised in cases of severe HDFN to try to avoid the morbidity of exchange transfusion. Intravenous immunoglobulin is thought to block the antibody receptors on the neonatal red cells and thus prevent haemolysis. However, data are conflicting on the efficacy of this intervention and ongoing research is needed.8
Delivery approach
In pregnancies complicated by alloimmunisation but with no fetal anaemia, delivery at term (37 to 38 weeks) is common practice. Caesarean section is not routinely indicated; induction of labour is usually appropriate, with continuous electronic fetal monitoring intrapartum.4 In women where there is evidence of fetal anaemia after 34 weeks, early delivery may be indicated and a caesarean delivery may be needed.
Alloimmunised pregnancies with evidence of fetal anaemia before 34 weeks are candidates for in utero fetal therapy, which is discussed in another section.
Multidisciplinary input
Delivery of a baby in an alloimmunised pregnancy requires multidisciplinary input. The neonatology team should be made aware of the delivery timing so that they can prepare appropriately. Timely communication with the blood bank is also essential. Usually it is useful to obtain a group and antibody screen from both partners in the lead up to delivery so that type-specific blood for the neonate can be available if needed emergently.
At the time of delivery, a cord blood sample must be sent for extended blood group analysis, a Coombs test (for haemolysis) and for measurement of haemoglobin and bilirubin levels. (A fetus with haemolysis excretes more bilirubin in their urine.) This provides the neonatal team with an early indication of the potentially serious nature of the condition.
Managing women at high risk for HDFN
Alloimmunised pregnant women whose antibody levels reach the critical threshold and any woman who has developed Kell antibodies or had a previous pregnancy where their baby developed severe HDFN should be managed by a maternal–fetal medicine specialist (Box 2). These high-risk women need increased antenatal surveillance for fetal anaemia.
Assessing fetal anaemia
Before the year 2000, the only way to assess fetal anaemia was to undertake invasive testing of at-risk women. These women would undergo regular amniocenteses so the amniotic fluid could be tested for bilirubin levels, with high levels being an indication for fetal transfusion. The problem with this approach – in addition to being invasive and uncomfortable for the woman – was the risk of stimulating preterm labour every time an amniocentesis was performed. However, a landmark publication in 2000 revolutionised the management of high-risk alloimmunised women.9 It made regular non-invasive ultrasound assessment of the fetal middle cerebral artery blood flow the cornerstone of surveillance in high-risk pregnancies. Now only women with confirmed fetal anaemia on middle cerebral artery Doppler ultrasound are subjected to the risks of an invasive procedure.
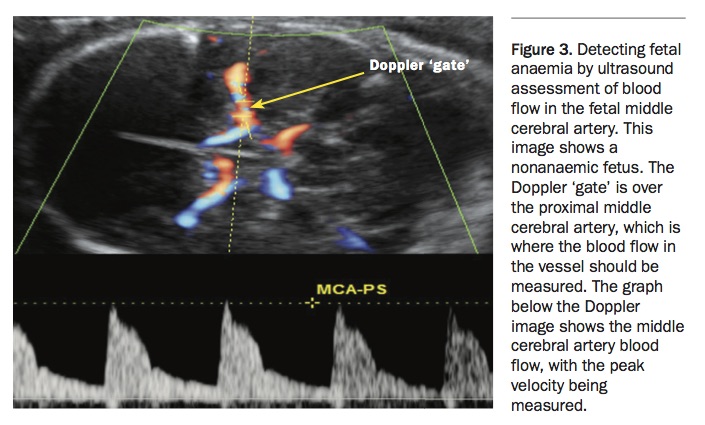
The middle cerebral artery Doppler assessment measures middle cerebral artery blood flow by measuring the artery’s peak systolic velocity (Figure 3). It works on the principle that the red cell mass of the fetus is reduced when the fetus is anaemic, which leads to a reduced viscosity and a faster blood flow that is measurable with ultrasound. The peak systolic velocity in the middle cerebral artery can be easily measured on an ultrasound scan by appropriately trained clinicians from 16 weeks, identifying anaemic fetuses with a high sensitivity and a low rate of false-positive results.
{kind=link}
When red cell transfusion is indicated
Evidence of fetal anaemia before 34 weeks using middle cerebral artery Doppler ultrasound is an indication for in utero fetal red cell transfusion. This should be performed by an experienced operator in a centre with expertise in fetal transfusion. A needle is inserted through the maternal abdomen, under ultrasound guidance, into the umbilical cord vein or fetal vasculature. Steroids for fetal lung maturation should be considered before commencing the procedure if appropriate.
Intrauterine fetal transfusion carries a significant risk and is only used as a life-saving intervention. Even the best centres in the world report fetal loss rates of 1.5 to 2% per procedure and the rate is even higher in centres performing fewer procedures.5 Also, intrauterine transfusion for alloimmunisation is not curative. In cases performed at very premature gestations, the alloimmunisation process continues and a follow-up transfusion after two to three weeks is usually needed. In many cases, multiple transfusions may be required.
Conclusion
Alloimmunisation is common, affecting 1% of pregnancies. This makes knowledge of red cell antibodies crucial for healthcare practitioners caring for pregnant women. All pregnant women should have a group and antibody screen early in pregnancy. Most women with red cell antibodies can be safely managed in pregnancy with serial monitoring of antibody levels and delivery at term. The partner’s extended blood group should also be tested to help guide management. Women at high risk for HDFN require referral to a maternal–fetal medicine specialist for close ongoing ultrasound surveillance. After birth, babies are at increased risk of anaemia and jaundice. In rare cases, severe alloimmunisation may lead to fetal anaemia that requires an intrauterine fetal transfusion. MT