Lymphoedema: breaking the swollen cycle

Lymphoedema
Lymphatic diseases
Lymphoedema can have a significant impact on a patient’s physical, psychological, social and financial wellbeing. Its early detection and appropriate management are pivotal in reducing the unnecessary suffering of affected patients.
- GPs will see both patients at risk of lymphoedema (for whom prevention is crucial) and those who already have lymphoedema.
- Early detection of lymphoedema and intervention significantly improve patient outcomes, and early referral of patients to a qualified lymphoedema practitioner for treatment will achieve the best outcomes.
- Compression is the mainstay of lymphoedema management but must be carefully prescribed to prevent adverse effects.
- Lymphatic insufficiency may be an underlying cause for patients presenting with limb cellulitis; control of the swelling can reduce the frequency of cellulitis episodes.
- GPs can facilitate prompt antibiotic therapy for lymphoedema-related cellulitis, which can present differently from classic cellulitis and usually requires a longer course of antibiotics.
- Simple strategies can become part of an everyday routine for patients with support from their GP and lymphoedema practitioner.
Picture credit: © Pixologic Studio/SPL
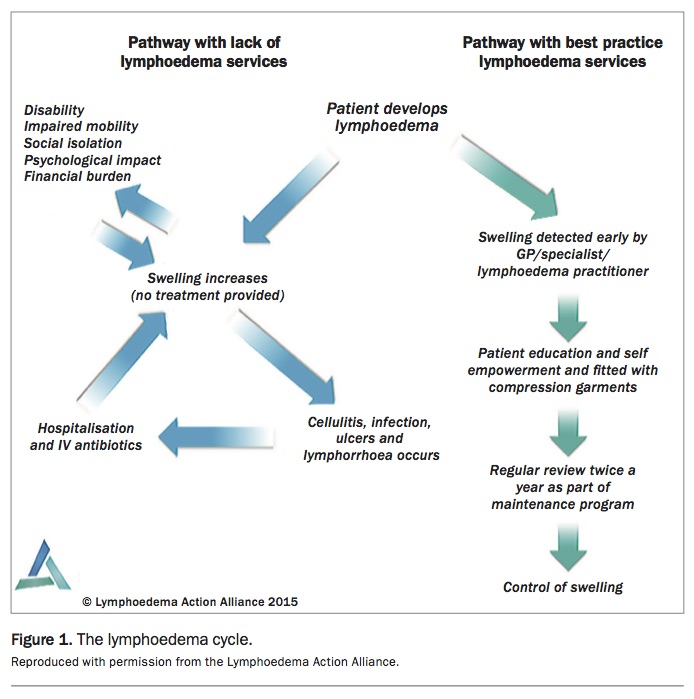
Established lymphoedema is associated with significant morbidity. Suboptimal management of people with lymphoedema can result in avoidable health complications, such as cellulitis with prolonged hospitalisation and poorer patient outcomes, as shown in Figure 1.
{kind=link}
What is lymphoedema?
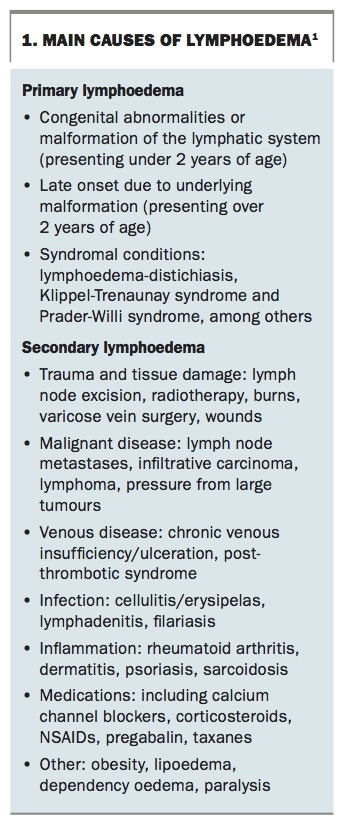
Lymphoedema is a chronic swelling of a limb or body region. It occurs when there is an imbalance in the transportation and/or production of fluid in the interstitial tissues resulting in the accumulation of extracellular fluid.1 It may arise as a result of a congenital malformation of the lymphatic system (primary lymphoedema) or due to damage and trauma to, or interference with, the lymphatic vessels or nodes (secondary lymphoedema). The main causes of both types of lymphoedema are listed in Box 1.1
{kind=link}
Although lymphoedema starts as a fluid-focused condition, in some patients it can progress to the accumulation of adipose and fibrotic tissue in the affected region. This excess fluid and/or tissue reaction is associated with inflammatory mediators, resulting in altered local immunity.
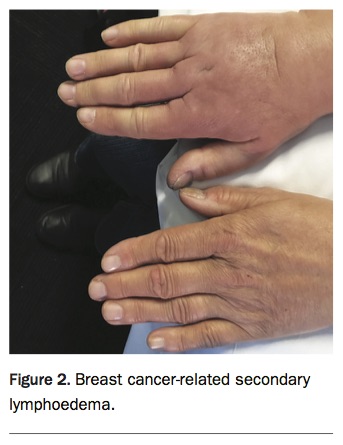
In developed countries, the most common cause of lymphoedema is cancer related (Figure 2). Approximately 15.5% of cancer survivors develop lymphoedema.2 This varies depending on the type of cancer, surgical intervention and adjuvant therapies. Other causes of secondary lymphoedema include trauma, infection, surgery and vascular conditions. A newly emerging and increasingly frequent cause of lymphoedema is obesity. The prevalence of this is less clear and largely undocumented. Primary lymphoedema makes up the remainder of the cases. There may be several contributing causes present in the one patient, called mixed lymphoedema.
{kind=link}
Prevalence studies in the UK have reported 0.13 to 2.0 per 1000 people living with lymphoedema.3 There are no equivalent Australian data, but conservative estimates suggest that there might be at least 35,000 people living with lymphoedema in the country.
Presentation
Lymphoedema should be considered in patients who have swelling of a body part that has persisted for more than three months (or earlier if it is associated with surgical removal of lymph nodes). It may be associated with heaviness and aching, and in the initial stages, diurnal fluctuation.
Diagnosis
The diagnosis of lymphoedema is a clinical one based on history and examination. It should be holistic in its approach and encompass any physical, functional or psychosocial issues a person may be facing.
Steps in the diagnosis of lymphoedema, including the differential diagnoses to consider, are summarised in the Flowchart.4 Further medical review and investigations are needed to exclude other causes of swelling when the following red flags are present:
- sudden acute onset of swelling
- pain as a main presenting complaint
- skin colour changes
- prominent collateral veins in the region of swelling
- lumps, sores, ulcers
- paraesthesia, other neurological signs
- history of unmonitored cancer.
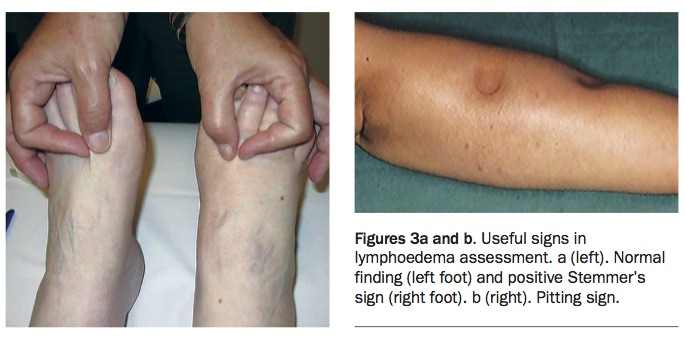
Important signs to look for in the clinical examination are the Stemmer’s sign and the pitting sign (Figures 3a and b). The Stemmer’s sign is the inability to pinch the skin at the base of the second toe or middle finger, which is considered pathognomonic of lymphoedema.5 The pitting sign is persistent indentation of the skin following firm thumb pressure for up to 30 seconds over the oedematous area, and is indicative of subcutaneous oedema.
{kind=link}
Lymphoedema can present many years after the triggering event, as shown in the following case.
A case of secondary lymphoedema
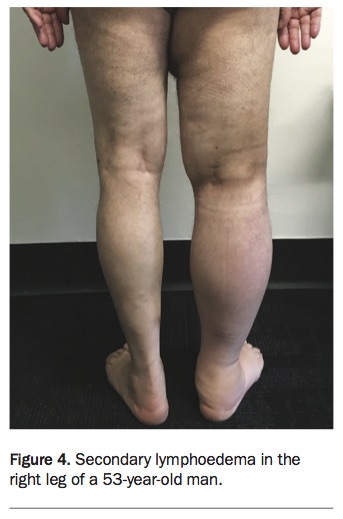
A 53-year-old farmer presents with swelling in his right leg (Figure 4). His leg has been progressively becoming more swollen and heavy, and now he can no longer fit into his right work boot. On history, he reveals that he had a melanoma removed from his right thigh 10 years ago. He remembers having had surgery to his groin for lymph node removal. He has a large fibrotic scar on his right thigh and groin.
{kind=link}
Key messages
- Lymphoedema can present many years after the triggering event.
- This patient has been at a high risk for lymphoedema ever since he had groin lymph node surgery. He would have benefited from regular surveillance and education on risk factors to raise awareness of the early signs and symptoms.
- It is important to exclude DVT and any recurrence of melanoma.
Investigations
Several investigations can be useful tools in the process of lymphoedema diagnosis, but not all are necessary.
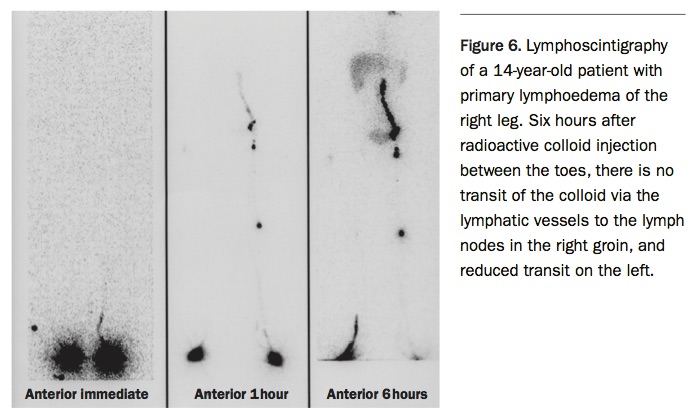
- Lymphoscintigraphy is a nuclear medicine procedure used to demonstrate lymphatic morphology and function. It is particularly useful where the cause of swelling is unclear (see the case below).
- New imaging techniques are rapidly evolving, such as indocyanine green fluoroscopy (ICG), which can be used to map the superficial lymphatics. This can be useful in difficult clinical cases.
- Ultrasound, Doppler ultrasound, MRI and CT can be useful to exclude differential diagnoses and also to assess for local area tissue changes.
- Bioimpedance spectroscopy (BIS) using low frequencies can measure extracellular fluid and can indicate differences between normal and lymphoedematous limbs. It is useful in monitoring patients at high risk of lymphoedema to detect early subclinical changes.
A case of primary lymphoedema in an adolescent
A 14-year-old girl presents with a swollen right foot and ankle (Figure 5). The swelling has been present for six months, and persisted after a minor sprain. Her GP has already excluded a DVT and other differential diagnoses, but is not sure what else can be causing this problem.
{kind=link}
Key messages
- Persistent swelling of more than three months needs a diagnosis, and primary lymphoedema should be considered.
- In this instance, lymphoscintigraphy is indicated to help with the diagnosis of primary lymphoedema (Figure 6).
- Early referral is recommended in such cases for treatment in a multidisciplinary paediatric lymphoedema clinic (if available) or alternatively to a trained lymphoedema practitioner to optimise swelling and prevent infections.
{kind=link}
Treatment
Once the diagnosis of lymphoedema is confirmed, the patient should be referred to a lymphoedema practitioner who can provide a range of treatments, help in developing skills for lifelong self-management and prescribe suitable compression garments.
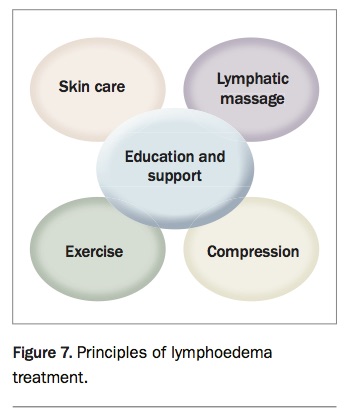
Best practice lymphoedema treatment is a multimodal regimen (Figure 7), including the components listed below.
{kind=link}
- Skin care involves cleansing and moisturising the skin to provide a barrier and encourage lymphatic flow. It includes regular checks for fungal infections and cellulitis.
- Exercise encourages lymph flow and is important for weight management. Hydrotherapy is a recommended form of exercise due to the incorporation of hydrostatic pressure.
- Compression is used initially in the form of bandaging to reduce swelling. Compression garments can then be used to maintain this reduction (see below).
- Manual lymphatic drainage is a specific decongestive massage technique to help move fluid away from congested areas.
- Education and support is central to these principles and to GP management. Engagement of patients in their self-management regimen is crucial.
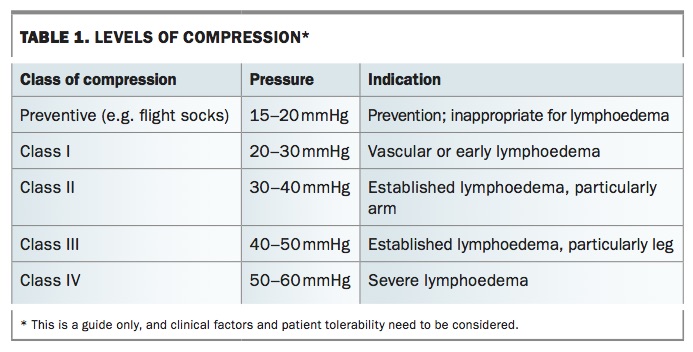
The ability of compression garments (e.g. sleeves, stockings, gloves) to maintain the gains made by intensive treatment depends on the appropriate choice of garment and the adherence of the person to the wearing regimen.6 For this reason, the garment should be fitted by a qualified professional, such as a trained lymphoedema practitioner or garment provider, to ensure the correct pressure and gradient distal to proximal. Numerous types of compression are available in a range of sizes, fabrics and methods of application with varying levels of compression (Table 1 and Figure 8).
{kind=link}
{kind=link}
Contraindications for compression include severe arterial insufficiency, uncontrolled heart failure or severe peripheral neuropathy (e.g. diabetes). Before commencing lower leg compression, vascular assessment is recommended to exclude any underlying arterial insufficiency.7 The ankle-brachial pressure index (ABPI) can be used if there are concerns about arterial insufficiency.
Newer compression treatments are constantly emerging. These include sequential intermittent pneumatic compression, low level laser, negative pressure and lymph taping.
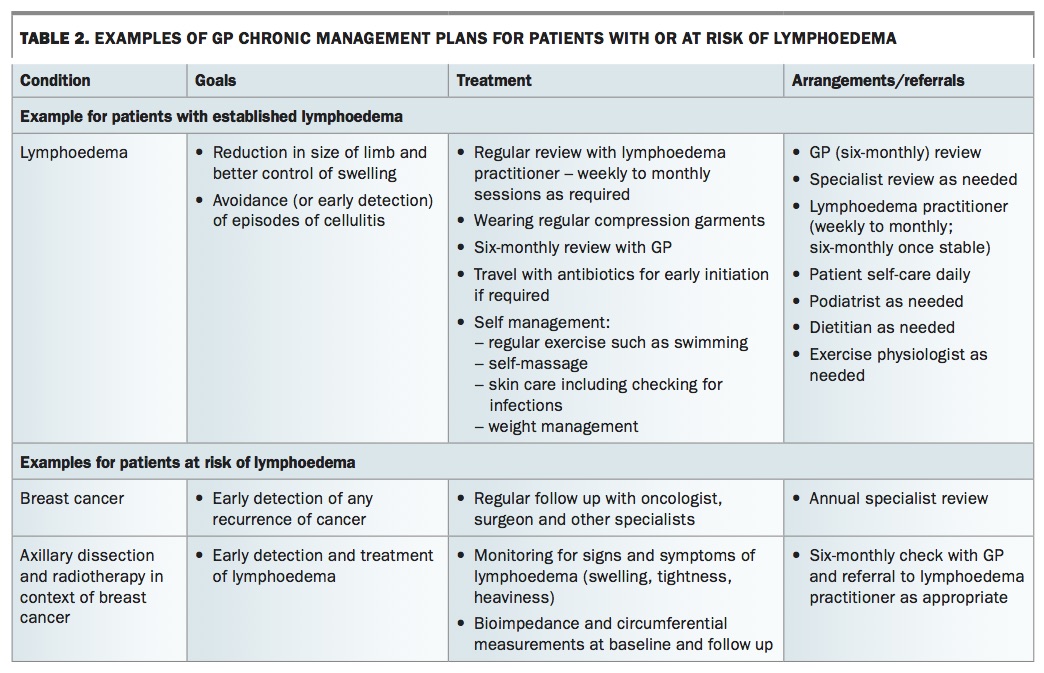
The GP has a role in the long-term chronic care management plan of patients with lymphoedema (Table 2). Simple treatments and discussions with patients can make a significant difference to their outcomes. Reinforcing good skin care, travel precautions, antibiotic use, exercise and massage are all part of the GP’s role. GPs can facilitate the creation of a good multidisciplinary team that could consist of a lymphoedema practitioner, podiatrist, dietitian and psychologist.
{kind=link}
Where to find a lymphoedema practitioner?
Lymphoedema practitioners are allied health professionals (e.g. physiotherapists, occupational therapists, nurses) and remedial massage therapists who have completed Australasian Lymphology Association (ALA) accredited lymphoedema management training. They can be found in some larger public hospitals that have a lymphoedema service available, and there are also several private practitioners. The ALA website has an online register of qualified lymphoedema practitioners (http://www.lymphoedema.org.au/the-register/find-a-practitioner).8
Lymphoedema-related cellulitis
Cellulitis presents with an acute spreading inflammation of the skin and subcutaneous tissues characterised by pain, swelling, warmth and erythema. Its onset can be highly variable in lymphoedema. Systemic symptoms often precede these signs. The decision to start antibiotics should not depend on blood test results, but rather on the patient’s clinical presentation. Prompt treatment is essential to avoid further damage to the lymphatics, which, in turn, may predispose to recurrent cellulitis.
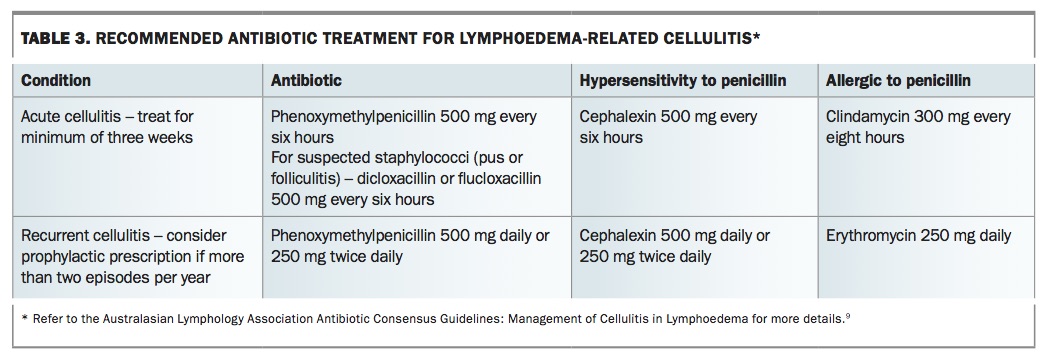
Nonpurulent cellulitis is most likely caused by group A streptococci, which remain 100% sensitive to penicillin. Purulent cellulitis is more likely to be caused by Staphylococcus aureus, which has a significant resistance profile.9 If present any pus should be swabbed; however, empirical antibiotics should be commenced in the interim (Table 3).
{kind=link}
Antibiotics should be continued for 14 days after a definite clinical response is noted. Drawing a line around cellulitic areas and reviewing 48 hours after starting antibiotics are important to establish efficacy of treatment and appropriateness of referral to hospital. Patients should be encouraged to return to wearing compression garments as soon as there is reduction in the acute symptoms of cellulitis.
The case of an elderly patient with mixed lymphoedema, a combination of secondary and dependent lymphoedema with cellulitis, is described below.
A case of dependency oedema, ulcers and recurrent cellulitis
An 82-year-old woman presents with her niece. She has swelling in her legs bilaterally. Her right leg is significantly more swollen (Figure 9). It is red, hot and tender across her right shin. She has had a fever for 48 hours. She has a history of varicose vein surgery and hysterectomy when in her 40s. She prefers to sleep in a recliner chair.
{kind=link}
Key messages
- This patient has a combination of secondary oedema and dependent oedema, which has placed her at increased risk of cellulitis.
- Her cellulitis needs to be treated urgently.
- The diagnoses of congestive cardiac failure and DVT need to be excluded.
- Concurrent treatment of her comorbidities and lymphoedema can help to improve her quality of life. Treating the swelling and addressing the skin integrity will reduce her risk of recurrent cellulitis, and assist in mobilisation.
Dispelling the myths
There are many myths in the lymphoedema literature regarding safety for patients. Some of these include: avoiding repetitive exercise; avoiding blood pressure measurements, venepuncture or injections in the affected limb; flying being a precipitating factor to lymphoedema; and avoiding all use of diuretics. Below the authors attempt to set the record straight.
- Exercise and usual activities should be encouraged in patients with lymphoedema. Recent Australian research has shown that exercise may be preventive for those at risk of breast cancer-related lymphoedema.10
- Blood pressure should ideally be measured in an unaffected arm. However, there is no evidence of exacerbation from taking single blood pressure readings in a lymphoedema-affected arm. Taking repetitive blood pressure readings (e.g. during surgery or 24-hour blood pressure monitoring) should be discouraged in the affected limb.
- There is no evidence that venepuncture triggers lymphoedema when performed using aseptic techniques by experienced health professionals; however, when possible it should be performed on the unaffected arm.
- Injections or vaccinations (e.g. tetanus vaccination) can induce an inflammatory reaction and, therefore, should be avoided in the affected limb.
- Flying can be a trigger for exacerbations in those with established lymphoedema. There is little evidence of this in at-risk populations. Prophylactic garments are often worn to prevent lymphoedema, but it is vital that they are appropriately fitted and trialled before travel. An ill-fitting garment can do more harm than good due to a possible tourniquet effect or poor pressure gradient.
- Diuretics do not remove lymphatic fluid in subcutaneous tissue. However, their use may be indicated where there is coexistent congestive cardiac failure. Diuretics can be used concurrently with compression in this instance.
- Bilateral cellulitis is extremely rare. Symmetrical erythema in the legs is most likely due to stasis dermatitis, particularly in the absence of systemic features.
Prevention
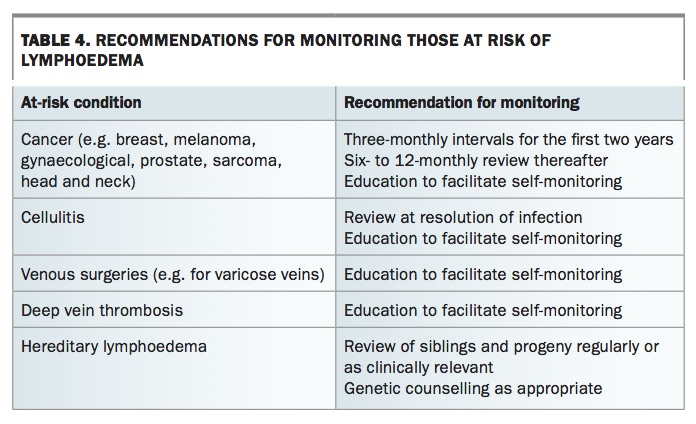
Effective identification of patients at risk of lymphoedema relies on an awareness of the causes of lymphoedema (see Box 1).1 The GP has an important role in monitoring for the early detection of lymphoedema in high-risk groups, especially after cancer therapy resulting in lymph node excision (Table 4). This monitoring should become part of a GP’s chronic care management plan.
{kind=link}
Surgical intervention
New treatments are available for the surgical management of lymphoedema. These are available to selected patients in specialist units. Liposuction is an option for severe lymphoedema that is no longer responsive to conservative treatment. However, patients who have liposuction are still required to wear compression garments. Super-microsurgical techniques based on new imaging are an emerging area of plastic surgery. These include lymphovenous anastomosis and vascularised lymph node transfer. These specialised surgical techniques should be embedded in an integrated lymphoedema service model.11
Conclusion
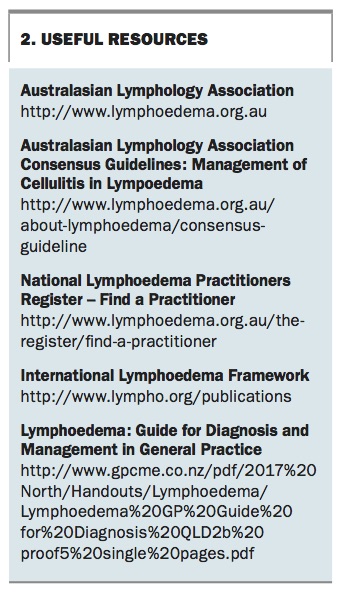
Lymphoedema detection and treatments are constantly evolving with new techniques in compression and surgery. Early and accurate diagnosis of lymphoedema by the GP remains the key to accessing appropriate treatment. GP co-ordination of a multidisciplinary team will ensure the best outcomes for the patient with, or at risk of, lymphoedema. A list of useful online resources for GPs is given in Box 2. MT
{kind=link}
References