Liam's allergy symptoms: better while away, recurring when back home

Allergy
Rhinitis
A 45-year-old man who suffers from the allergy trifecta experiences symptom improvement when he takes a trip to Thailand but is disappointed to find his symptoms quickly recur when he returns home. What treatment might be appropriate in his situation?
Case scenario
Liam is a 45-year-old man who has marked eczema, asthma, hayfever and allergic rhinoconjunctivitis. He has just returned from a six-week trip in Thailand, where he ceased his medications for these conditions because he found he had no symptoms of allergy or asthma while he was away. Once he returned to Australia the symptoms recurred.
Liam’s medications for rhinoconjunctivitis include a corticosteroid intranasal spray and antiallergy eyedrops (olopatadine hydrochloride, levocabastine and a combination preparation of pheniramine maleate and naphazoline hydrochloride), but he says these have never controlled his symptoms satisfactorily. He lives in a coastal area on the eastern seaboard of Australia.
- If Liam were to move to another part of Australia, such as to a mountain area, are his conditions likely to improve or to recur?
- What is the place of allergy testing in this setting? Should the GP arrange this testing (and if so, which tests) or refer the patient?
- How successful is desensitisation? Is sublingual immunotherapy less successful than subcutaneous immunotherapy?
- Liam noticed resolution of both rhinoconjunctivitis and asthma while he was away. What is the association between these two atopic conditions, and why is it that if one is poorly controlled then the other may flare too?
Commentary
Liam has the allergy trifecta of allergic rhinoconjunctivitis (ARC), asthma and eczema. It is not uncommon for allergy patients returning from overseas to notice symptom improvement while away and deterioration on return, usually within 24 hours. Although this phenomenon has not been specifically studied it could arise from two possibilities:
- a change in allergen exposure in a different environment
- relief of stress by temporarily leaving behind workplace and relationship issues and entering a ‘time out’ period.
A change in allergen exposure might include reduction in exposure to house dust mite (HDM), which is generally high in the domestic environment of coastal Australia where conditions for HDM growth (warm and humid) are optimal. In addition, measurable levels of HDM are known to be lower in other countries and also in ‘public places’, which would include aeroplanes, airports and hotels.
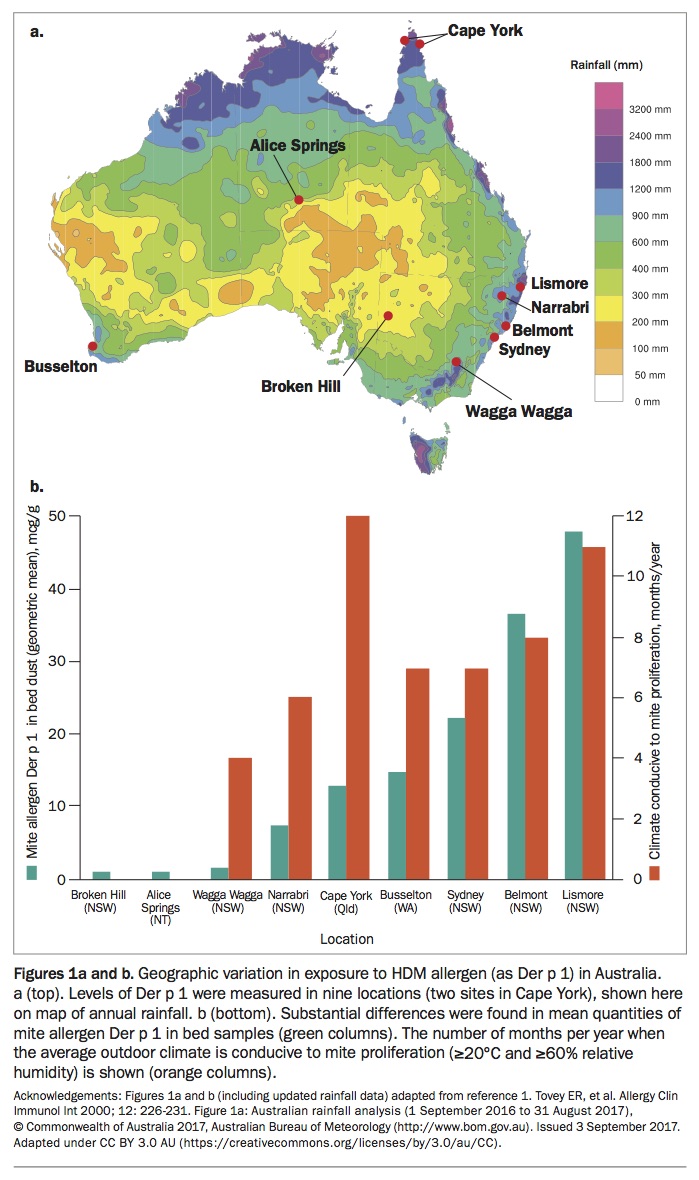
Levels of domestic mite species and the main HDM allergen (Der p 1) have been measured in nine locations around Australia, with Broken Hill and Alice Springs being the only places where HDM levels were found to be consistently low (Figures 1a and b).1 For Liam, moving to a different part of the coast or to the mountains is unlikely to significantly improve his symptoms. Humidity over 60% is largely responsible for HDM load, with low humidity being strongly suppressive of HDM proliferation. It is estimated that HDM or Der p 1 levels less than 10 mcg/g are required to prevent symptoms and less than 2mcg/g to prevent sensitisation. So far anti-dust measures in the Sydney area – although reducing HDM levels significantly – have not consistently achieved levels of Der p 1 below 10mcg/g, which is why anti-HDM measures are frequently ineffective.
{kind=link}
Pollen allergy is Australia is often due to a combination of temperate and subtropical grasses, whereas in large parts of Europe the main pollens are temperate and in Thailand they would be tropical or subtropical. In Sydney, 72% of allergy patients are sensitised to both temperate and subtropical grasses,2 so it is possible for them to visit another part of the world where the pollen is no longer a relevant allergen trigger.
Eczema can be aggravated by a number of factors including allergen exposure, weather patterns (usually worse in winter) and also routine skin care measures such as moisturisation (which patients might have more time to attend to when they are away from home).
Management
Liam is using a large number of medications for his upper airways disease or ARC and still has poorly controlled symptoms. Using the Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines, it is likely that his ARC would be categorised as moderate to severe and therefore considered suitable for immunotherapy.3 The ARIA guidelines are available online (http://dx.doi.org/10.1016/j.jaci.2012.07.053). Disease severity is often underestimated. Patients with severe ARC have poorly controlled local symptoms but also impaired quality of life, with poor sleep, increased absenteeism and presenteeism, poorer examination and physical performance and increased anxiety. It should be noted that immunotherapy is only appropriate when:
- a patient is shown to be atopic on skin testing or serum specific IgE testing (this testing can be performed by GPs),
- the positive result is clinically relevant, and
- asthma is adequately controlled to allow use of immunotherapy – that is, FEV1 more than 80% for subcutaneous immunotherapy (SCIT) and FEV1 more than 70% for sublingual immunotherapy (SLIT).4
If Liam is suitable for desensitisation then this treatment should be offered because he presents with treatment failure. The treatment is successful for HDM, grasses and cat allergens. It is a long and moderately expensive form of therapy, so patients need to be well motivated to commence treatment, which will last for a minimum of three years. For some allergens there is now a choice of SCIT or SLIT (liquid or tablets). Recent large studies with tablets (HDM and grass pollen) have demonstrated good efficacy in ARC and also asthma.5 The SLIT preparations are most expensive but have fewer systemic side effects and so have become increasingly popular. Studies have shown that regular follow up improves adherence to treatment while cost analyses confirm the positive cost benefits of treatment.6
This case demonstrates the concept of united airways disease, where inflammation of both upper and lower airway exists in the same patient. Between 80% and 100% of patients with asthma have acute or chronic rhinosinusitis; and 50% of patients with allergic rhinitis have asthma.7 It has been well demonstrated that if one part of the airway (either upper or lower) is exposed to allergen then this results in an inflammatory response in the other site.8 It should be noted that treatment of both upper and lower airways disease results in overall better control of symptoms, so this patient’s asthma needs to be carefully assessed with a history, asthma control questionnaire and spirometry. His treatment for asthma should be reviewed and an asthma action plan should be given. Guidelines for asthma treatment are provided in the current Australian Asthma Handbook.4
Final comments
It is not uncommon for allergy patients returning from overseas to notice symptom improvement while away and deterioration on return. For patients with moderate to severe disease for whom symptom-directed treatment does not control disease satisfactorily, specific immunotherapy should be considered. MT
COMPETING INTERESTS: Associate Professor Rimmer is an Advisory Board member for Sequirus and has received an honorarium for a presentation from Stallergenes.