Refractory shallow ulcers on the lower leg

Leg injuries and disorders
Test your diagnostic skills in our regular dermatology quiz. What is the cause of this patient’s persistent leg ulceration and can it be adequately treated?
Case presentation
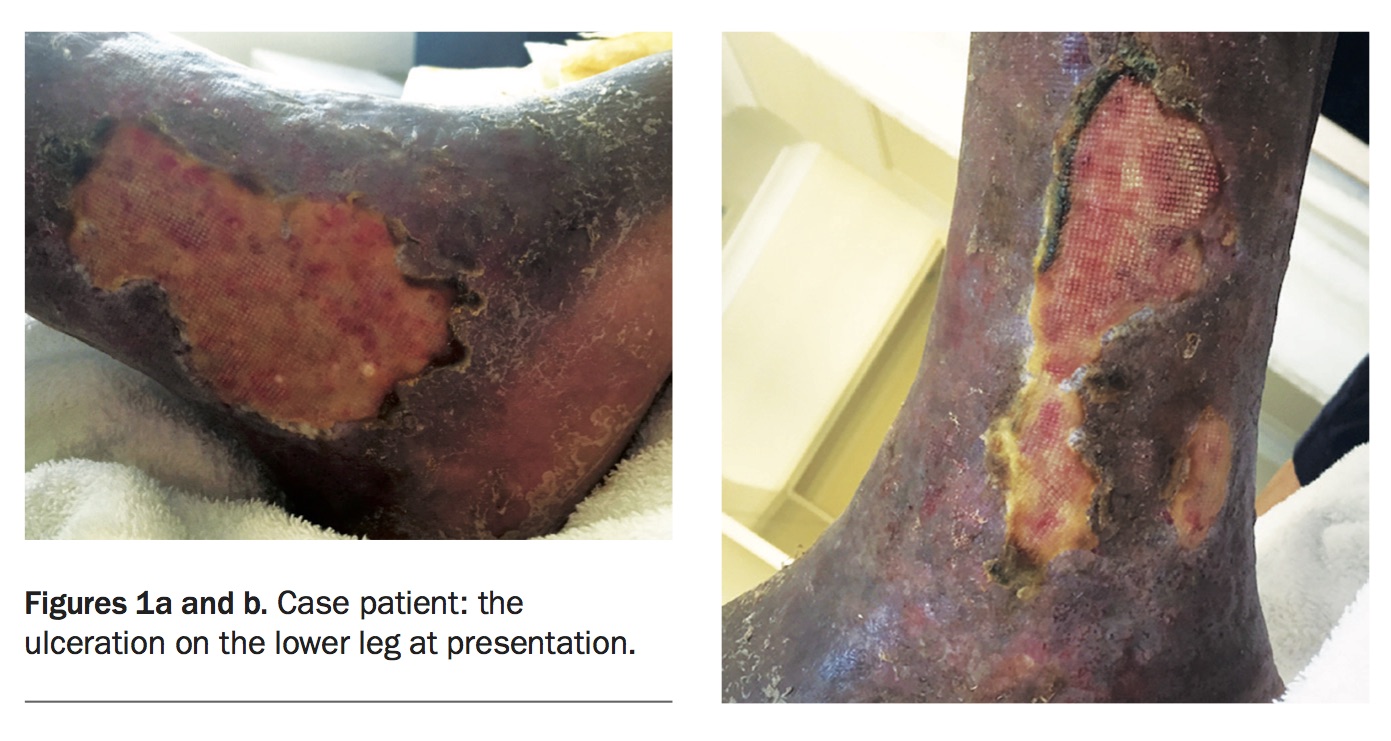
An 82-year-old man presents with persistent shallow ulceration of his lower right leg that has been present for three years (Figures 1a and b). It is moderately painful and has been recurrently infected. The patient has been treated with ulcer dressings and antibiotics with bed rest without improvement; skin grafting carried out a year ago also failed. The surrounding skin is dry, scaly and pigmented.
{kind=link}
The patient is otherwise in good health. His pedal pulses are palpable. Diabetes has been ruled out and his skin sensation is normal.
Differential diagnoses
Conditions to consider among the differential diagnoses include the following.
- Arterial ulcers. Ulcers caused by advanced peripheral arterial disease are the result of inadequate perfusion of the skin. Pain is an important feature and may occur when walking and on leg elevation. Ischaemic ulcers are typically located on the feet or toes and have punched out borders with a white or black wound base and an absence of granulation tissue. The surrounding skin shows signs of poor perfusion, such as feeling cold or having a white or cyanosed appearance, and pulses are absent or difficult to palpate. There is often other evidence of atherosclerotic disease, such as coronary artery disease or stroke.
- Pyoderma gangrenosum. This uncommon neutrophilic dermatosis rapidly breaks down skin, causing severely painful ulceration (Figure 2). It is not infectious and often occurs in association with a systemic condition such as inflammatory bowel disease, rheumatological disease or haematological malignancy; paraproteinaemia may be present.1 Pyoderma gangrenosum can be difficult to diagnose clinically, and does not have a characteristic appearance on biopsy. A history of pathergy (minor trauma to the skin such as a needlestick injury resulting in progressive ulceration) is characteristic but not always present or pathognomonic. The ulcer base is sloughy with a violaceous, undermined and irregular border.
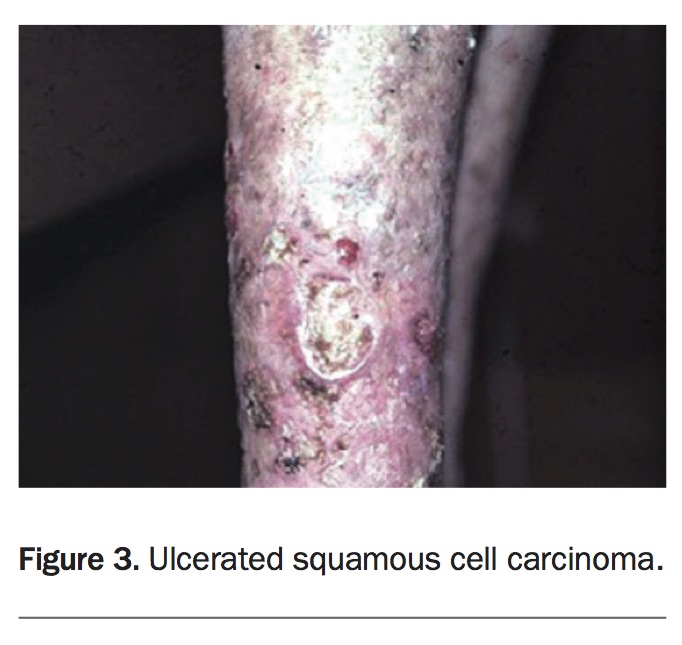
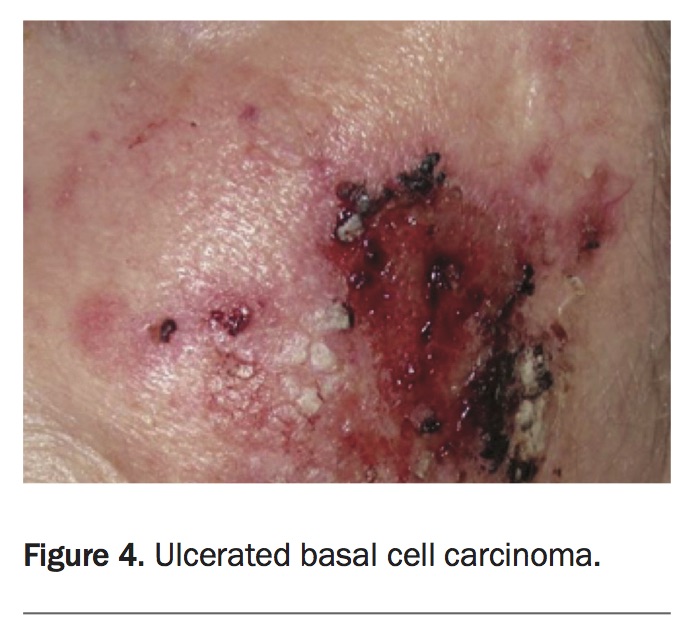
- Malignancy. Many advanced cutaneous malignancies can ulcerate, including squamous cell carcinoma (Figure 3), basal cell carcinoma (Figure 4), lymphoma, sarcoma and melanoma. Ulceration due to malignancy is not necessarily painful. To rule out a malignant process, a biopsy from the edge of the lesion should be performed for any ulcer of unknown aetiology.
- Polyarteritis nodosa and Wegener’s granulomatosis. These very rare diseases are characterised by necrotising vasculitis. Other clinical features of polyarteritis nodosa include livedo reticularis or tender cutaneous nodules on lower extremities.2 In Wegener’s granulomatosis, patients are usually very unwell and have other signs of cutaneous vasculitis, upper respiratory tract symptoms, fever and renal disease. Serious vasculitis is unlikely in the case patient described above, who has no features of systemic disease or associated cutaneous manifestations.
- Infection. In an immunocompetent host who is well and afebrile, a cutaneous infection causing a chronic nontender ulcer is unlikely. Nonetheless, the possibility of a deep fungal or mycobacterial infection should be considered and can be ruled out by biopsy and tissue culture. In tropical areas, diseases such as melioidosis (Burkholderia pseudomallei infection) and leishmaniasis can cause cutaneous ulceration.
- Dermatitis artefacta. Cutaneous lesions caused by self-harming actions are often apparently painless and bizarre in appearance (Figure 5). Patients hide these actions from their doctors and often give an illogical or incongruent history of the lesion. The most common sites of involvement are easily reached, such as the face (particularly the cheeks), backs of the hands, forearms (most commonly on the nondominant limb) and legs. The surrounding skin is normal, and a biopsy performed from the edge of the ulcer shows a sharp transition between normal and necrotic skin.
- Neuropathic ulcer. Ulceration may occur in patients with a peripheral neuropathy and is similar in appearance to dermatitis artefacta. The ulceration is due to unintentional pressure and trauma to skin where there has been sensory loss, and such ulcers are therefore usually located on pressure points (e.g. the heel).
- Venous ulcer. This is the correct diagnosis. Venous insufficiency is the most common cause of ulceration of the lower leg. A venous ulcer is typically painless and the surrounding skin shows trophic changes, such as dryness, scale and hyperpigmentation. A reddish or brown skin colour due to haemosiderin deposition supports the diagnosis. The surrounding tissue may become indurated (lipodermatosclerosis). Peripheral oedema may occur, resulting in an ‘inverted champagne bottle’ appearance of the legs.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Management
The first step in management of a painful venous ulcer is culture to rule out secondary infection. For the patient described above, whose ulcer was painful, swabs revealed Staphylococcus aureus and he was admitted to hospital for bed rest with leg elevation, analgesia, antibiotics, dressings and compression stockings. Skin care with moisturisers, a moderate potency topical corticosteroid and emollient was commenced.
Venous ulcers are often very persistent and many treatments may be attempted, such as compression therapy, hydrocolloid dressings and skin grafting. Care of surrounding skin is important to prevent dermatitis and reduce the risk of superinfection. In this patient’s case, all of these treatments had failed.
Recently, anecdotal success for treating venous ulcer has been reported using topical timolol in the ophthalmic 0.5% gel that is commercially available.3,4 As this patient’s ulcer had been resistant to all previous treatments, a trial of timolol 0.5% gel was commenced while he was in hospital, with gel administered at 1 cm intervals around the edge of the ulcers. This is off-label use of timolol but was considered to be low risk. The ulceration responded rapidly to the treatment, with healing within six weeks (Figures 6a and b).
{kind=link}
The patient was discharged with continuation of skin care, compression stockings and timolol gel, which he was advised to apply immediately to any new areas of ulceration. He was admitted for a short period a year later, with new venous ulceration after ceasing timolol treatment. This responded rapidly to re-treatment. The patient remains well and has begun planning an overseas trip.
Final comments
The use of topical timolol for venous leg ulcers is currently being investigated in a clinical trial (https://clinicaltrials.gov/ct2/show/NCT02422017). At the time of writing, it is not standard of care. A trial of topical timolol was commenced for the patient described above because standard treatment had failed; however, it may not be effective in every case. The risk of treatment with topical timolol is low and limited to local irritation. It does not have to be administered in a hospital environment. MT
References