Urinary incontinence in men: an approach to diagnosis and management

Urinary incontinence
Men's health
Urinary incontinence is a common but underrecognised problem in men. A systematic approach can aid in the diagnosis and management of these patients, including when to refer them for specialist input.
Urinary incontinence is a common problem among Australian men, affecting about one million men, and increases in prevalence with age. Up to one in four men aged over 70 years experience this condition, which can significantly affect their quality of life.1 However, uncertainties regarding diagnosis often result in a delay in appropriate management.
Urinary incontinence in men can be classified as stress urinary incontinence (SUI), urge urinary incontinence (UUI), mixed incontinence (a combination of SUI and UUI symptoms), continuous incontinence, overflow incontinence, postmicturition dribble and functional incontinence.2 As the most common subtypes, SUI and UUI are the focus of this article. Postmicturition dribble and overflow incontinence have previously been covered in detail in our article on benign prostatic hyperplasia.3 Postmicturition dribble is usually relieved by antegrade milking of the urethra from perineum to glans to remove residual urine.4
Understanding the condition
Stress urinary incontinence
SUI in men is often iatrogenic after pelvic surgery, such as radical prostatectomy, which may result in sphincter weakness or dysfunction or a change in urethral axis or motility.5 The exact mechanisms of male continence are not yet fully understood but are generally thought to be a combination of anatomical and functional factors, making it difficult to predict the effect of surgery on any given patient’s continence.5 Rarely, other factors such as neurological disease or pelvic trauma can result in SUI.
Urge urinary incontinence
UUI is associated with overactive bladder (OAB). OAB arises from a combination of hyperexcitability of smooth muscle in the bladder, increased parasympathetic nerve activation and, in cases of neurogenic OAB, denervation at the spinal or cortical level, resulting in the bladder operating through spinal reflex alone.6
OAB may occur in conjunction with various neurological conditions, inflammatory conditions of the bladder, psychological stress and ageing.7 Bladder outlet obstruction, usually prostatic, can result in detrusor hypertrophy and overactivity. This may only become symptomatic after transurethral resection of the prostate (TURP). Primary OAB may be idiopathic.
Diagnosis
The aim of the diagnostic evaluation is to determine the underlying type of incontinence, exacerbating factors and any complicating features.
History
The diagnostic work-up of urinary incontinence should begin with taking the patient’s history. Urinary urgency, frequency of urination and nocturia are the classic features of OAB, with or without UUI. SUI typically manifests as urinary leakage while performing activities that increase intra-abdominal pressure, such as coughing, laughing, sneezing, straining, sexual activity or heavy lifting. Volume and frequency of leakage should be assessed.
For all types of incontinence, the onset, duration and severity of symptoms should be ascertained. Fluid intake, including diuretics, caffeine and alcohol, should be recorded in a bladder diary, along with frequency, times and volumes of voided urine, frequency of incontinence and precipitants. Other urinary symptoms that may suggest a bladder outlet obstruction or urethral stricture, such as weak stream and hesitancy, should be considered.6,8-10
Neurological conditions, such as multiple sclerosis, spinal injuries, stroke and Parkinson’s disease, should be a focus when obtaining the medical history. Diabetes, previous urological history, previous pelvic surgery or radiotherapy and history of urinary infections can all have an effect on the severity, cause or treatment of UUI and SUI. Obstructive sleep apnoea, which is itself underdiagnosed, and other conditions causing sleep disturbance can increase nocturia. Complicating features such as haematuria, urinary tract infection or flank pain should also be noted.
Examination
Physical examination may indicate an undiagnosed neurological condition or a palpable distended bladder. Examination of the genitalia and prostate can identify obstructive disorders such as benign prostatic hyperplasia or meatal strictures. The presence of faecal impaction should be noted.
Investigations
Investigations should include a urine dipstick test, urine microscopy and culture, and a renal tract ultrasound to assess for hydronephrosis, postvoid residual volume and prostate volume (Box 1). A blood sample should be tested for renal function, fasting blood glucose level and, if indicated, prostate-specific antigen (PSA) level. A contrast CT intravenous pyelogram may occasionally be useful to exclude the presence of bladder lesions, fistulae or abnormal anatomy, such as a duplex collecting system.6,9
{kind=link}
Red flags indicating referral to a specialist are shown in Box 2. Specialised investigations performed by a urologist include:
{kind=link}
- uroflowmetry
- cystoscopy
- urodynamic studies
- 24-hour pad weight tests.
Urinary flow rate can be assessed in the clinic. Cystoscopy (endoscopic visualisation of the bladder wall) can be performed either with local anaesthetic in an outpatient setting or in an operating theatre with sedation. Urodynamic studies are important for accurately diagnosing lower urinary tract symptoms, especially in patients with incontinence, as they can aid in determining the underlying aetiology. It is useful to perform urodynamic studies before considering surgical treatments.9,10
Urologists will often use 24-hour pad weights to classify incontinence as mild, moderate or severe. This classification can vary for different types of incontinence and is usually proportional to the patient’s activity level.11 The test is performed with the patient wearing waterproof underwear to reduce evaporation and begins with an empty bladder. The patient undertakes normal activity and changes pads every four to six hours, weighing each one. In patients with UUI, a total pad weight increase over 24 hours of 4 to 20 g is mild, 21 to 74 g moderate and more than 75 g severe.12 In patients with postprostatectomy SUI, the 24-hour weight increases for stratification are higher: less than 100 g is mild, 100 to 400 g is moderate and more than 400 g is severe.13
Treatment
Stress urinary incontinence
Conservative treatment
Conservative treatment of SUI involves pelvic floor muscle training and weight loss. Pelvic floor muscle training has been shown to hasten return to continence after radical prostatectomy,14 but there is no clear evidence that it improves overall long-term continence rates.15
Surgical treatment
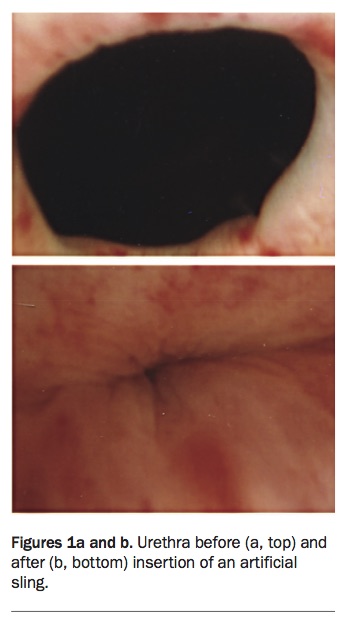
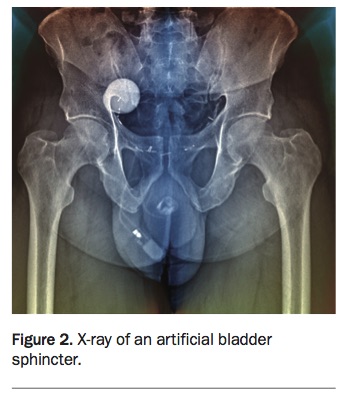
Surgical treatment options for SUI are urethral slings (Figures 1a and b) and the artificial urinary sphincter (AUS) (Figure 2). Various slings, including minimally invasive and adjustable types, are available. The advantage of a sling is that it requires no manipulation with voiding, unlike an AUS, which needs to be cycled manually before each void. Urodynamic studies are recommended before insertion of a sling.10
{kind=link}
{kind=link}
Traditional teaching is that slings are used for milder incontinence and in patients without a history of radiotherapy. For severe incontinence, an AUS is recommended.16 Moderate incontinence can be treated by either a sling or an AUS after an informed discussion with the patient. A new type of adjustable sling, the ATOMS device, has been released on the Australian market.17 This can be used for all types of incontinence and in patients with a history of radiotherapy. However, for patients with severe incontinence, the AUS is still the gold standard. The ATOMS sling does not need to be cycled before each void but has an adjustable cushion that can augment continence by a simple in-clinic injection into a scrotal port. The degree of continence can therefore be titrated to effect. Ultimately, the choice of anti-incontinence device involves a discussion between the patient and the urologist regarding the benefits and disadvantages of each.
Both the AUS and slings carry a risk of erosion, infection, device failure and the need for revision. However, for men with incontinence, regaining control makes a significant difference to their quality of life.18,19
Urge urinary incontinence
Conservative treatment
Conservative options for treating UUI are behavioural modification, bladder retraining and pelvic floor exercises.6 Behavioural modification involves reducing caffeine intake, timing of fluid intake (spread out fluid intake rather than consuming large amounts of fluid at a time and avoid fluids within a few hours of bedtime), losing weight and avoiding constipation, and is often very effective. Success of bladder retraining and pelvic floor exercises can be optimised by involving specialist pelvic floor physiotherapists.
Medical treatment
Medical treatment of UUI is divided into first-, second- and third-line pharmaceuticals. First-line therapy is an antimuscarinic anticholinergic medication, such as oxybutynin or solifenacin, which inhibits unwanted contraction of the bladder through antagonism of its muscarinic receptors. However, these medications have the potential side effects of dry eyes, dry mouth, constipation, urinary retention and cognitive decline. More than half of patients treated with anticholinergic agents will cease treatment within the first three months.20
Transdermal delivery of oxybutynin may be better tolerated than oral medication, particularly in those who are bothered by a dry mouth.20 Extended-release preparations are generally better tolerated and have fewer side effects than immediate-release preparations.18 In multiple studies, no antimuscarinic medication has proved more effective or better tolerated than others.21 The short- and long-acting forms of oxybutynin and short-acting proprantheline are the most commonly prescribed anticholinergics for OAB that are listed on the PBS.
Second-line therapy is the beta-3 agonist mirabegron, which relaxes the bladder by stimulating adrenergic receptors in bladder smooth muscle. As a relatively new agent, long-term data are not yet available; however, its side effect profile is generally better than that of antimuscarinics, with hypertension (which needs to be monitored) being the main reported adverse effect.22 As a result, some urologists are now using mirabegron as first-line therapy. However, it is not listed on the PBS and costs about $55 per month.
As tricyclic antidepressants have anticholinergic effects, they have historically been used for treating UUI (off-label use). However, there are no recent studies looking at their efficacy, and their use should generally be limited to patients who cannot tolerate first- or second-line medications.
Surgical treatment
Surgical treatment for OAB and UUI is reserved for patients in whom conservative approaches and medical therapy have not been effective. Urodynamic studies should be performed for patients with suspected OAB and UUI before surgical intervention, to confirm the aetiology and rule out other causes (e.g. bladder obstruction).
Intravesical botulinum toxin type A injections can be performed under local or general anaesthesia and offer effective and durable improvement in continence, although the patient will require retreatment usually every three to six months.23,24 Sacral nerve neuromodulation involves insertion of an electrode into the S3 foramen under general anaesthesia. The electrode is connected to an implanted device, which stimulates the nerves to the bladder. This has been shown to be effective in multiple studies.25,26 Patients will typically have a temporary lead inserted as a trial to ensure improvement before receiving a formal lead and implanted nerve stimulator.
Bladder augmentation and urinary diversion are reserved for only the most refractory cases and are rarely performed.
Mixed urinary incontinence
In patients with mixed urinary incontinence, the most bothersome symptoms should be treated first.9 Specialist intervention is often needed, as the patient may require a combination of surgical and medical therapies.
Conclusion
Male urinary incontinence is underrecognised and can be a challenging management problem. Treatment needs to be individualised, with attention paid to determining the underlying cause. General practitioners play a vital role in accurately assessing patients, initiating therapy, counselling patients about behavioural modification strategies and determining which patients require referral to a urologist. MT