Investigating thyrotoxicosis
Thyroid diseases
Endocrine diseases
Case scenarios are used in this section to educate doctors on the best approach to the diagnosis and management of patients with different endocrine problems. The appropriate selection of tests and correct interpretation of test results are discussed.
Thyrotoxicosis is characterised by the clinical syndrome of abnormally high levels of circulating thyroid hormones, whereas hyperthyroidism refers to the endogenous overproduction of thyroid hormones.1 Thyrotoxicosis is a common occurrence in general practice, with varying prevalences in different countries according to iodine status. In iodine-rich countries such as Australia, the prevalence is 0.5%,2,3 whereas in iodine-deficient countries the prevalence is higher, reaching 2% of population.4 Women are ten times more likely to be affected than men.5
There are many causes of thyrotoxicosis, with Graves’ disease being the most common and accounting for 80% of cases (Box).6 Graves’ disease is an autoimmune condition characterised by stimulatory antibodies binding to thyroid-stimulating hormone (TSH) receptors in the thyroid, resulting in thyroid over-stimulation. Occasionally, these antibodies may also bind to retro-orbital tissue, resulting in inflammation with fibrosis (ophthalmopathy). Such antibodies may also be responsible for patches of red, swollen skin over the shins (dermopathy). Autonomous (hyperfunctioning) thyroid nodules are common causes of thyrotoxicosis.
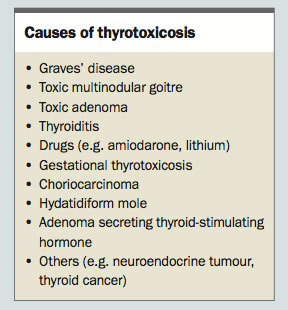{kind=link}
Toxic multinodular goitre is more common in iodine-deficient areas and is the most common cause of subclinical hyperthyroidism.6 A single autonomous thyroid nodule causing thyrotoxicosis is referred to as toxic adenoma. Thyroiditis or inflammation of the thyroid gland is responsible for 10% of cases of thyrotoxicosis. In such situations, follicular destruction caused by the inflammatory process results in high serum levels of thyroid hormones from release of preformed thyroid hormones (predominately free thyroxine [T4], but also includes free triiodothyronine [T3]). Thyroiditis can be caused by viral infection, autoimmunity, medications, iodine administration and, rarely, trauma.7,8
Clinical features
Signs and symptoms of thyrotoxicosis are determined by a patient’s age, severity of thyrotoxicosis and aetiology. The clinical spectrum ranges from asymptomatic cases to thyroid crisis and heart failure.9 Classic symptoms of thyrotoxicosis include easy fatigability, heat intolerance, profuse sweating, irritability, sleep disturbance and palpitations. Weight loss despite increased appetite is characteristic. Rarely, patients may present with weight gain due to hyperphagia. Goitre is a common finding in patients with thyrotoxicosis, but may not always be evident on physical examination.
Symptoms of thyrotoxicosis in the elderly may be atypical and can include lethargy, reduced appetite, palpitations and weight loss. Apathetic thyrotoxicosis is the appropriate term for this form of thyrotoxicosis. It may be due to age-related decline in sympathetic response to the action of thyroid hormones.10,11 Symptoms may be subtle and therefore overlooked. Consequently, diagnosis can be delayed and complications may occur.10
Thyrotoxicosis-related morbidity and mortality arise from cardiovascular complications. Atrial fibrillation complicates 15% of cases and its incidence increases with age.12,13 Atrial fibrillation can lead to thromboembolism, myocardial ischaemia and heart failure.14,15 It is therefore important to control thyrotoxicosis before major surgery. Other complications include osteoporosis, menstrual irregularities and infertility in women, gynaecomastia in men and thyrotoxic periodic paralysis.16-19
Thyroid storm is a rare medical emergency due to under-treated severe thyrotoxicosis, often precipitated by sepsis. It may occur following radioactive iodine treatment in patients with poorly-controlled thyrotoxicosis. Patients present with high fevers, excessive sweating, vomiting, diarrhoea, tachyarrhythmias and reduced consciousness.20 Prompt recognition with treatment is vital, as this condition carries a high mortality
Thyroid function testing
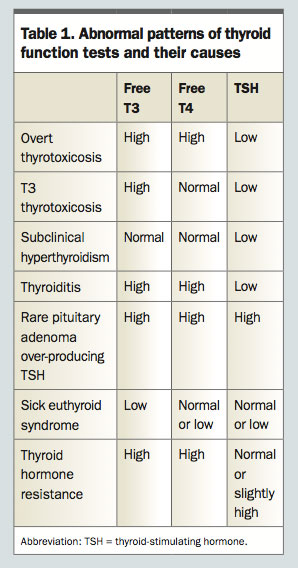
Thyroid function testing (TFT) is the mainstay in the diagnosis of thyrotoxicosis (Table 1). A TSH level below 0.01 mIU/L is highly sensitive and specific for thyrotoxicosis.21 Mild increases in thyroid hormone result in lowering or suppression of TSH production. Occasionally, free T3 level is mildly elevated with normal free T4 and suppressed TSH levels. This is referred to as T3 thyrotoxicosis and represents early hyperthyroidism, commonly due to Graves’ disease or toxic adenoma.
{kind=link}
In overt thyrotoxicosis, TSH is undetected with elevated free T4 and/or free T3 levels. In subclinical hyperthyroidism, TSH level is low but may be undetectable, whereas free T3 and free T4 levels are within the normal range, by definition.1,21
In seriously ill patients, TFTs may exhibit a distinct pattern with low free T3, normal or low free T4 and normal or low TSH levels. This is called sick euthyroid syndrome (also referred to as nonthyroidal illness) and may be part of the adaptive response to acute illness and starvation. Treatment of the underlying illness often resolves this unusual pattern of TFTs. If an initial TSH level is low but not suppressed, it is prudent to repeat the TSH measurement at least a month later before assuming a diagnosis of subclinical hyperthyroidism, as nonthyroidal illness states may be present instead. In thyroid hormone resistance, there is a mutation of the beta gene encoding thyroid hormone receptors, rendering peripheral tissues resistant to thyroid hormones. Typical TFTs include normal or slightly elevated TSH with high free T3 and free T4 levels. Patients usually lack symptoms of thyrotoxicosis, but tend to exhibit a goitre.22
Liver function tests
Mild liver enzyme elevations are common in thyrotoxicosis. Elevated alkaline phosphatase levels may be due to increased skeletal turnover. Excessive thyroid hormones may have a direct toxic effect on hepatocytes, leading to elevation of alanine amino transferase. Autoimmune liver diseases may occasionally coexist with autoimmune thyroid diseases.23 Very rarely, severe thyrotoxicosis may lead to progressive liver damage with centrizonal necrosis and perivenular fibrosis.24 The association of acute liver injury with use of antithyroid drugs (ATDs) is well known.24 Proposed mechanisms include generation of reactive oxygen species, mitochondrial injury and DNA damage.25 Fortunately, reports of fulminant liver failure are rare with use of ATDs, although propylthiouracil is more implicated than carbimazole.24,26 In general, the lowest possible dose of ATD should be used in managing people with thyrotoxicosis.
Imaging
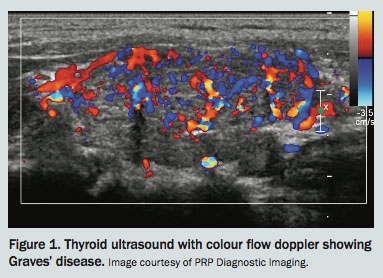
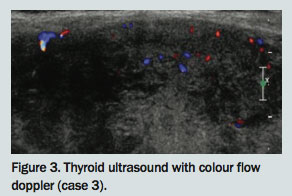
Two imaging modalities are commonly used to investigate people with thyrotoxicosis. These are ultrasonography with colour flow doppler and nuclear medicine imaging. Ultrasonography examines thyroid morphology, and is usually indicated if there is a nodular goitre to examine nodular characteristics. It can be useful if the diagnosis of thyrotoxicosis is unclear clinically, as it differentiates thyroiditis from nonthyroidal disease states. Parenchymal echoheterogeneity is usually detected in autoimmune thyroid diseases such as Graves’ disease and thyroiditis.27 Colour flow doppler allows estimation of thyroid blood flow. A highly vascular thyroid in a patient with thyrotoxicosis suggests active Graves’ disease rather than thyroiditis due to follicular destruction.21,28,29
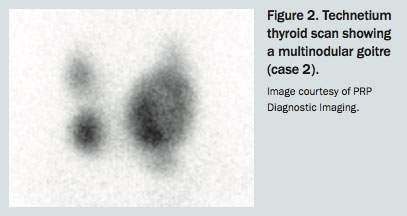
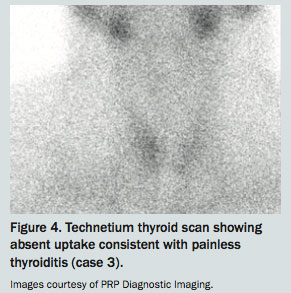
Nuclear medicine imaging with technetium thyroid scanning uses technetium pertechnetate (Tc-99m) to evaluate thyroid activity. Technetium pertechnetate is a molecule that mimics iodine and is readily taken up by the thyroid. The degree of uptake will differentiate between the hyperactive thyroid of Graves’ disease (diffuse and intense) and the hypoactive thyroid in destructive thyroiditis (low or absent uptake). Tc-99m thyroid scanning can also localise autonomous thyroid nodules(s) in toxic multinodular goitre (TMNG) and toxic adenoma (Table 2). Nuclear medicine imaging is contraindicated in pregnancy and breastfeeding.21
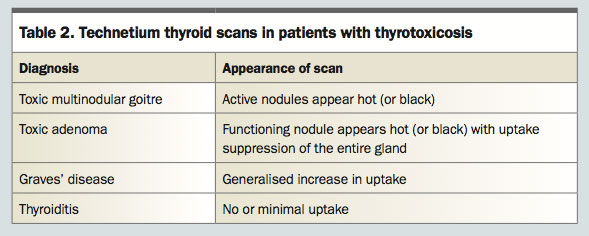{kind=link}
Case 1. Graves' disease
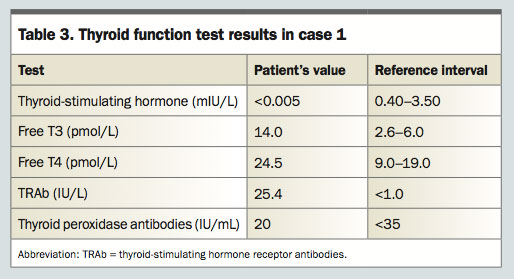
A 38-year-old woman who was previously well presents to her GP with unexplained tiredness, palpitations and a 6-kg weight loss over two months. Examination reveals ne peripheral tremor with sweaty palms, regular pulse of 126 beats per minute (bpm), blood pressure of 135/70 mmHg and respiratory rate of 17 bpm. Her thyroid gland is mildly enlarged, painless, soft on palpation and without lymphadenopathy. Generalised bruits are auscultated over the thyroid gland. Her eyes appear enlarged, with exposure of conjunctiva around the irises. Her right upper eye lid is swollen with mild lid lagging on downward gaze. Thyroid function test results are shown in Table 3.
{kind=link}
What do the test results show?
Graves’ disease can be diagnosed with confidence pending TSH receptor antibody (TRAb) levels and if clinical and biochemical features of thyrotoxicosis are present, along with diffuse goitre, bruits and orbitopathy. In this case, elevated TRAb levels are sensitive (96 to 97%) and specific (99%) for Graves’ disease.30 Although orbitopathy is useful in the diagnosis of Graves’ disease, it is present in less than a quarter of newly diagnosed patients.30 Thyroid imaging is generally not necessary if classic signs of Graves’ disease are present, along with biochemical documentation of thyrotoxicosis and raised TRAb levels.
The initial TRAb titre indicates immunological activity and serves as a baseline as it often normalises with use of ATDs. Graves’ disease is unlikely to remit if the TRAb titre is high at the end of the treatment.21 On the other hand, if the patient had a negative TRAb test, then technetium thyroid scanning with or without doppler flow ultrasound would be recommended to differentiate Graves’ disease from other causes of thyrotoxicosis (Figure 1).
{kind=link}
How should this patient be managed?
A beta blocker such as propranolol 10 mg twice daily should be commenced to alleviate symptoms of thyrotoxicosis. Nonselective beta blockers are preferred because they reduce peripheral conversion of free T4 to free T3 at high doses. If beta blockers are contraindicated, then calcium channel blockers may be used.31 Antithyroid treatment with carbimazole 10 mg twice daily should also be commenced, with TFT monitoring every six to eight weeks.
After three months and once euthyroid status is achieved, carbimazole can be gradually reduced to a maintenance dose of 5 mg daily. After 12 to 18 months of treatment, when both TFTs and TRAb titres have normalised, carbimazole may be discontinued. Thereafter, monitoring with TFTs initially every two to three months and then four to six monthly is recommended.21 If TFTs remain normal after 12 months of stopping ATDs, then yearly monitoring may suffice. Agranulocytosis and hepatotoxicity are serious but rare adverse effects of ATDs. Liver function tests and white cell counts are recommended during treatment.21
Relapse of Graves’ disease is common, and necessitates restabilisation on carbimazole and consideration for iodine-131 therapy or surgery as definitive treatment. Alternatively, patients may choose to keep taking ATDs indefinitely.21
Case 2. Toxic multinodular goitre
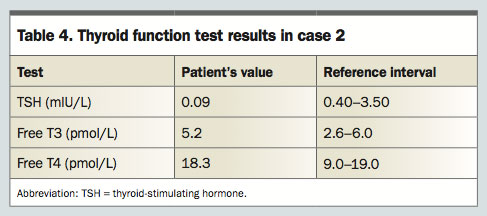
A 78-year-old woman presents to her GP with palpitations, tiredness and shortness of breath. Her past medical history includes euthyroid multinodular goitre. On examination, she appears apathetic and tired with generalised weakness. Her blood pressure is 147/87 mmHg and her pulse is 128 bpm and irregular. Neck palpation reveals an asymmetrical nodular goitre. ECG confirms atrial fibrillation.
What do the test results show?
TFTs show a nonsuppressed TSH level with normal free T4 and free T3 levels, suggesting subclinical hyperthyroidism (Table 4). Common causes of subclinical hyperthyroidism are TMNG and toxic adenoma. Classically, in this patient, there is a long-standing history of euthyroid multinodular goitre, which may harbour autonomous nodules. Less common causes of subclinical hyperthyroidism are Graves’ disease and thyroiditis.
{kind=link}
Subclinical hyperthyroidism is a biochemical entity and it does not mean the patient is truly asymptomatic as arrhythmias are common in these scenarios. The risk of atrial fibrillation increases with a TSH level below 0.1 mIU/L.
A thyroid ultrasound shows a multinodular goitre and a technetium thyroid scan shows patchy uptake suggesting TMNG (Figure 2). TRAbs are not detected. TRAb titre should be checked as Graves’ disease and multinodular goitre may coexist.
{kind=link}
How should this patient be treated?
Nonselective beta blockers and carbimazole should be started, pending definitive treatment with surgery or radioactive iodine (RAI) treatment. Thyroidectomy is indicated for large goitres causing compression of trachea or oesophagus resulting in obstructive symptoms. However, it is relatively contraindicated in elderly patients and those with reduced cardiovascular fitness. RAI is effective in treating TMNG but confers a significant risk of post-treatment hypothyroidism.
In this case, there was no evidence of obstruction and, after careful discussion about the pros and cons of both treatment modalities, the patient chose RAI therapy. After three months, once euthyroid status was achieved, RAI therapy was administered. However, the patient developed post-RAI hypothyroidism six months later, and required lifelong thyroxine replacement.
Case 3. Painless thyroiditis
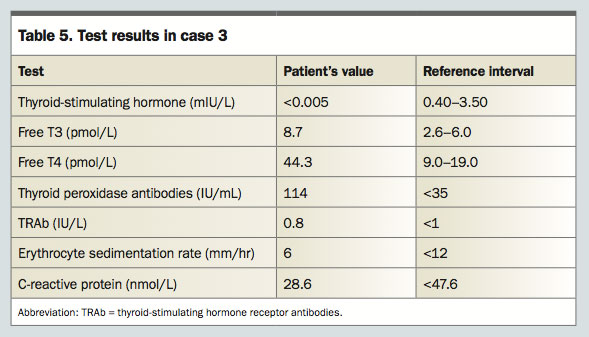
A previously healthy 36-year-old man presents with thyrotoxicosis of a two-week duration. He has a diffuse, nontender goitre. Mild lid-lagging is evident without orbitopathy. Thyroid function testing and measurement of thyroid antibodies and inflammatory markers are performed (Table 5).
{kind=link}
What is the diagnosis?
Lack of thyroid nodularity on examination does not exclude TMNG or toxic adenoma, as small nodules are not easily palpable. High free T4/T3 ratio suggests thyroiditis. Thyroid peroxidase antibody titres are present in people with painless thyroiditis.33 High titres generally indicate underlying autoimmune or Hashimoto’s thyroiditis. However, low titres may be detected in 10 to 30% of the normal population.3,34 Low-titre TRAb likely excludes Graves’ disease, although, rarely, people with Graves’ disease may present with low-level or absent antibodies.30
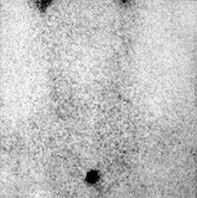
Thyroid ultrasound with colour flow doppler and technetium thyroid scanning often differentiate thyroiditis from antibodies-negative Graves’ disease and concealed toxic adenoma. In this case, thyroid ultrasound with colour flow doppler reveals a heterogeneous gland without thyroid nodules, and diminished blood flow (Figure 3). Technetium thyroid scan demonstrates generalised low uptake (Figure 4), confirming thyroiditis in the thyrotoxic phase.
{kind=link}
{kind=link}
What is painless thyroiditis and how is it treated?
Painless thyroiditis (also referred to as silent thyroiditis) is an uncommon cause of thyrotoxicosis, comprising only 5% of all cases.35 It is an important diagnosis to consider as it is a relatively self-limited condition. In contrast to subacute thyroiditis, patients do not experience neck pain or constitutional symptoms. Inflammatory markers such as C-reactive protein and erythrocyte sedimentation rate are typically normal.36 Patients may present with thyrotoxicosis lasting two weeks to three months, typically followed by hypothyroidism lasting up to six months.
Although most cases recover, 10 to 20% of patients develop permanent hypothyroidism.33 Propranolol 10 mg twice daily is the mainstay of treatment for thyroiditis in the thyrotoxic phase. ATDs are not used as they may lead to prolonged hypothyroidism.21
Conclusion
A thyroid function biochemistry panel is important in confirming the suspicion of thyrotoxicosis. Certain clinical features and TFT patterns may provide accurate clues on the causes of thyrotoxicosis. Subsequent investigations such as thyroid antibodies testing, thyroid ultrasound and technetium thyroid scanning may help to differentiate the aetiologies, particularly if classic signs and symptoms are absent.
COMPETING INTERESTS: None.
References
- De Leo S, Lee SY, Braverman LE. Hyperthyroidism. Lancet 2016; 388: 906-918.
- Dahl P, Danzi S, Klein I. Thyrotoxic cardiac disease. Curr Heart Fail Rep 2008; 5: 170-176.
- Hollowell JG, Staehling NW, et al. Serum TSH, T(4), and thyroid antibodies in the United States population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J Clin Endocrinol Metab 2002; 87: 489-499.
- Knudsen N, Jorgensen T, Rasmussen S, Christiansen E, Perrild H. The prevalence of thyroid dysfunction in a population with borderline iodine deficiency. Clin Endocrinol 1999; 51: 361-367.
- Vanderpump MPJ. The epidemiology of thyroid disease. Br Med Bull 2011; 99: 39-51.
- Laurberg P, Pedersen IB, Knudsen N, Ovesen L, Andersen S. Environmental iodine intake affects the type of nonmalignant thyroid disease. Thyroid 2001; 11: 457-469.
- Seigel SC, Hodak SP. Thyrotoxicosis. Med Clin North Am 2012; 96: 175-201.
- Bindra A, Braunstein GD. Thyroiditis. Am Fam Physician 2006; 73: 1769-1776.
- Goichot B, Caron P, Landron F, Bouee S. Clinical presentation of hyperthyroidism in a large representative sample of outpatients in France: relationships with age, aetiology and hormonal parameters. Clin Endocrinol 2016; 84: 445-451.
- Boelaert K, Torlinska B, Holder RL, Franklyn JA. Older subjects with hyperthyroidism present with a paucity of symptoms and signs: a large cross-sectional study. J Clin Endocrinol Metab 2010; 95: 2715-2726.
- Boelaert K. Thyroid dysfunction in the elderly. Nat Rev Endocrinol 2013; 9: 194-204.
- Parmar MS. Thyrotoxic atrial fibrillation. MedGenMed 2005; 7: 74.
- Frost L, Vestergaard P, Mosekilde L. Hyperthyroidism and risk of atrial fibrillation or flutter: a population-based study. Arch Intern Med 2004; 164: 1675-1678.
- Traube E, Coplan NL. Embolic risk in atrial fibrillation that arises from hyperthyroidism: review of the medical literature. Tex Heart Inst J 2011; 38: 225-228.
- Siu CW, Yeung CY, Lau CP, Kung AW, Tse HF. Incidence, clinical characteristics and outcome of congestive heart failure as the initial presentation in patients with primary hyperthyroidism. Heart 2007; 93: 483-487.
- Lam L, Nair RJ, Tingle L. Thyrotoxic periodic paralysis. Proc (Bayl Univ Med Cent) 2006; 19: 126-129.
- Nicholls JJ, Brassill MJ, Williams GR, Bassett JH. The skeletal consequences of thyrotoxicosis. J Endocrinol 2012; 213: 209-221.
- Meikle AW. The interrelationships between thyroid dysfunction and hypogonadism in men and boys. Thyroid 2004; 14 Suppl 1: S17-S25.
- Krassas GE, Poppe K, Glinoer D. Thyroid function and human reproductive health. Endocr Rev 2010; 31: 702-755.
- Chiha M, Samarasinghe S, Kabaker AS. Thyroid Storm. J Intensive Care Med 2015; 30: 131-140.
- Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association Guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid 2016; 26: 1343-1421.
- Ortiga-Carvalho TM, Sidhaye AR, Wondisford FE. Thyroid hormone receptors and resistance to thyroid hormone disorders. Nat Rev Endocrinol 2014; 10: 582-591.
- Huang MJ, Liaw YF. Clinical associations between thyroid and liver diseases. J Gastroenterol Hepatol 1995; 10: 344-350.
- Kyriacou A, McLaughlin J, Syed AA. Thyroid disorders and gastrointestinal and liver dysfunction: a state of the art review. Eur J Intern Med 2015; 26: 563-571.
- Heidari R, Niknahad H, Jamshidzadeh A, Eghbal MA, Abdoli N. An overview on the proposed mechanisms of antithyroid drugs-induced liver injury. Adv Pharm Bull 2015; 5: 1-11.
- Williams KV, Nayak S, Becker D, Reyes J, Burmeister LA. Fifty years of experience with propylthiouracil-associated hepatotoxicity: what have we learned? J Clin Endocrinol Metab 1997; 82: 1727-1733.
- Pedersen OM, Aardal NP, Larssen TB, Varhaug JE, Myking O, Vik-Mo H. The value of ultrasonography in predicting autoimmune thyroid disease. Thyroid 2000; 10: 251-259.
- Hari Kumar KV, Pasupuleti V, Jayaraman M, Abhyuday V, Rayudu BR, Modi KD. Role of thyroid doppler in differential diagnosis of thyrotoxicosis. Endocr Prac 2009; 15: 6-9.
- Alzahrani AS, Ceresini G, Aldasouqi SA. Role of ultrasonography in the differential diagnosis of thyrotoxicosis: a noninvasive, cost-effective, and widely available but underutilized diagnostic tool. Endocr Prac 2012; 18: 567-578.
- Tozzoli R, Bagnasco M, Giavarina D, Bizzaro N. TSH receptor autoantibody immunoassay in patients with Graves’ disease: improvement of diagnostic accuracy over different generations of methods. Systematic review and meta-analysis. Autoimmun Rev 2012; 12: 107-113.
- Tagami T, Yambe Y, Tanaka T, et al. Short-term effects of beta-adrenergic antagonists and methimazole in new-onset thyrotoxicosis caused by Graves’ disease. Intern Med 2012; 51: 2285-2290.
- Goichot B, Luca F. [Subclinical thyroid dysfunction]. Presse Med 2011; 40(12 Pt 1): 1132-1140.
- Mittra ES, McDougall IR. Recurrent silent thyroiditis: a report of four patients and review of the literature. Thyroid 2007; 17: 671-675.
- Legakis I, Manousaki M, Detsi S, Nikita D. Thyroid function and prevalence of anti-thyroperoxidase (TPO) and anti-thyroglobulin (Tg) antibodies in outpatients hospital setting in an area with sufficient iodine intake: influences of age and sex. Acta Med Iranica 2013; 51: 25-34.
- Ross DS. Syndromes of thyrotoxicosis with low radioactive iodine uptake. Endocrinol Metab Clin North Am 1998; 27: 169-185.
- Pearce EN, Farwell AP, Braverman LE. Thyroiditis. N Engl J Med 2003; 348: 2646-2655.