A child with swollen lips and angular cheilitis

Crohn's disease
Test your diagnostic skills in our regular dermatology quiz. What is the cause of this child’s progressive lip swelling?
Case presentation
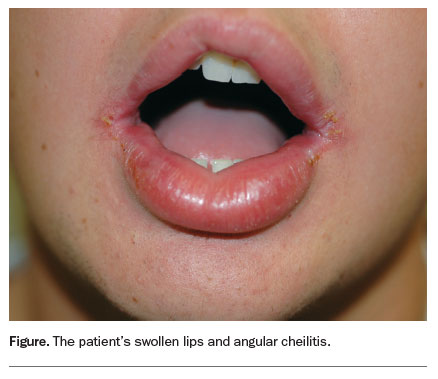
A 12-year-old boy presents with a three-month history of painless swelling of his upper and lower lips and angular cheilitis (Figure). He is otherwise well and is taking no regular medications.
{kind=link}
Differential diagnosis
For the patient described above, acute allergic angioedema, which occurs within one to two hours of contact with an allergen, is an important differential diagnosis to consider. Acute allergic angioedema can involve swelling of the lips and almost always occurs with urticaria. It may also result in airway compromise and is potentially a medical emergency. However, it is an intermittent condition, not a chronic one.
The correct diagnosis is orofacial granulomatosis, a rare chronic inflammatory disease characterised by relapsing/remitting lip swelling. It can also involve the buccal mucosa, gingivae and floor of the mouth. Orofacial granulomatosis is characterised by the histological finding of noncaseating granulomas that are indistinguishable from those of Crohn’s disease and similar to those of sarcoidosis.
Causes
Orofacial granulomatosis is a condition restricted to the orofacial region that may be caused by several granulomatous conditions. It encompasses more that one aetiology.1 The reported conditions are Crohn’s disease, sarcoidosis, Melkersson–Rosenthal syndrome and tuberculosis.
Crohn’s disease
Orofacial granulomatosis and oral Crohn’s disease share a number of clinical and histological features but the exact relationship between the two conditions is unknown. Although oral manifestations of Crohn’s disease can affect all age groups, they happen most frequently in children.2 The younger a child, the more likely it is that he or she will have intestinal inflammation, even when gut symptoms are not present.2 Mucosal signs such as linear ‘knife-cut’ ulcers and buccal swelling that gives a ‘cobblestone’ appearance may indicate Crohn’s disease as the underlying pathology in orofacial granulomatosis.3
Sarcoidosis
Sarcoidosis, which is characterised by noncaseating granulomas that can affect many different parts of the body, usually starts in the lungs or the lymph nodes of the chest. Patients can have associated generalised, nonspecific symptoms that should prompt further investigation (e.g. malaise, weight loss, loss of appetite and night sweats), but sarcoidosis can be isolated to the skin. Cutaneous sarcoidosis is known to be a great imitator, but skin biopsy will show noncaseating, epitheloid granulomas for diagnostic purposes.
Melkersson–Rosenthal syndrome
Melkersson–Rosenthal syndrome is an uncommon syndrome that results in chronic lip swelling due to granulomatous inflammation with recurrent facial palsy.4 It may have a genetic predisposition: patients may have an affected sibling or other relative who is unaffected except for a fissured tongue. Miescher’s cheilitis, another example of chronic swelling of the lip with confined granulomatous changes, is generally regarded as a monosymptomatic form of Melkersson–Rosenthal syndrome, but the possibility remains that these are two separate diseases.
Tuberculosis
Tuberculosis is a rarer cause of orofacial granulomatosis and should be considered in patients who have a family member with the infection and in immigrants from countries where it is endemic.5 Patients with orofacial granulomatosis due to tuberculosis present with associated cervical lymphadenopathy and systemic features such as fever and malaise.
Investigations
A diagnosis of orofacial granulomatosis is confirmed by a lip biopsy. Investigations should be aimed at identifying any underlying local or systemic disease. Recognised causes of granulomas such as sarcoidosis and Crohn’s disease should be excluded with requisite serology and chest x-ray. Intradermal tuberculin skin test and/or Quantiferon Gold blood test can be performed if there is suspicion of tuberculosis. Endoscopy or colonoscopy may be indicated if the history is suggestive of Crohn’s disease.5 A dental assessment to exclude active dental and periodontal disease is advisable.
Patch testing for unrecognised food allergies may also be undertaken. Atopy occurs more frequently in patients with orofacial granulomatosis than in the general population and allergies to a variety of agents (such as toothpaste, cinnamon foods, preservatives, dental materials and infections) have been suggested as possible aetiological factors. However, although patients are often atopic and exclusion diets may be helpful, a relevant allergen is rarely found on patch testing.6
Management
Spontaneous remission of orofacial granulomatosis can occur but is rare. Management is essentially symptomatic, and the degree of disfigurement needs to be considered when approaching treatment.
For patients with mild disease, dietary modification (exclusion of cinnamon and benzoate) can be trialled initially.7 For patients with recurring lip swelling episodes, oral medications such as tetracycline, metronidazole or dapsone are sometimes helpful in reducing inflammation. Corticosteroids are variably effective – these can be used as topical or systemic preparations or intralesional injections (triamcinolone acetonide 5 to 40 mg/mL).8 Intralesional corticosteroid is usually first-line treatment but needs to be repeated at regular intervals, between six and 12 weeks.
In patients with concurrent Crohn’s disease, early referral to a gastroenterologist is warranted. Systemic treatment for Crohn’s disease can improve orofacial granulomatosis. Topical tacrolimus ointment has been reported to be effective for oral and perineal Crohn’s disease but this is only likely to be effective in mild disease.
The response of orofacial granulomatosis to treatment is slow. Partial or complete improvement can be observed in most but not all patients, although this can take years. Treatment of disfiguring permanent orofacial swelling or severe orofacial granulomatosis can be exceedingly difficult. Surgery may be required for patients with severe permanent swelling that interferes with speaking or eating.
Outcome
For the case patient presented above, initial treatment with oral minocycline (100 mg daily) reduced his swelling initially, but the treatment became less effective with time. Over the next year he was treated with intralesional triamcinolone acetonide (10 mg every three months). He was referred for colonoscopy and found to have asymptomatic Crohn’s disease. Treatment with azathioprine was commenced, and the boy’s lip swelling resolved. MT
COMPETING INTERESTS: None.
References
- Weidenfeld D, Ferguson MM, Mitchell DN, et al. Oro-facial granulomatosis – a clinical and pathological analysis. Q J Med 1985; 54: 101-113.
- Sanderson J, Nunes C, Escudier M, et al. Oro-facial granulomatosis: Crohn’s disease or a new inflammatory bowel disease? Inflamm Bowel Dis 2005; 11: 840-846.
- Campbell H, Escudier M, Patel P, et al. Distinguishing orofacial granulomatosis from Crohn’s disease: two separate disease entities? Inflamm Bowel Dis 2011; 17: 2109- 2115.
- Scully C, Almedia ODP, Bagan J, Diz PD, Mosqueda A. Oral medicine and pathology at a glance. Oxford: Wiley Blackwell; 2010.
- Ramesh V. Orofacial granulomatosis due to tuberculosis. Pediatr Dermatol 2009; 26: 108-109.
- Smith VM, Murphy R. Orofacial granulomatosis and overlap with Crohn’s disease. Clin Exp Dermatol 2012; 38: 33-35.
- White A, Nunes C, Escudier M, et al. Improvement in orofacial granulomatosis on a cinnamon- and benzoate-free diet. Inflamm Bowel Dis 2006; 12: 508-514.
- Fedele S, Fung PP, Bamashmous N, Petrie A, Porter S. Long-term effectiveness of intralesional triamcinolone acetonide therapy in orofacial granulomatosis: an observational cohort study. Br J Dermatol 2014; 170: 794-801.