Switching or stopping antidepressants: a clinical viewpoint
Depression
Antidepressants
As no antidepressant is ideal for all patients, GPs often face the challenge of withdrawing or switching patients’ antidepressants. Considerations before withdrawing or switching an antidepressant, choice of new antidepressant, impact of discontinuation syndrome and switching strategies are outlined in this article.
- As no antidepressant is tolerable or effective for all patients, doctors commonly have to stop or switch their patients’ antidepressants.
- A recommended approach to antidepressant prescribing is to ‘start low and go slow’ and ensure an adequate dosage is reached.
- If the treatment response is inadequate after a reasonable period (four weeks at a therapeutic dose) then the diagnosis should be reviewed and a switch to another antidepressant considered.
- Discontinuation syndrome is common with many antidepressants and can impact on patient adherence to a new medication.
- Switching strategies include conservative or moderate switching, in which the first antidepressant is slowly tapered and ceased before the next one is started, direct switching and cross-tapering.
Picture credit: © Jonathan Dimes
Antidepressants, preferably in conjunction with support, psychotherapy and social rehabilitation, can be helpful for patients who present with disabling unipolar major depression. They are also used to treat patients with obsessive–compulsive disorder, panic disorder, social anxiety disorder (social phobia) and post-traumatic stress disorder. However, some patients do not tolerate specific antidepressants (studies suggest about 10% of patients for any particular medication), although they may tolerate others. In addition, about one-third of patients with depression do not respond to the initial antidepressant prescribed but may respond to another.1 As a result, there is often a need to stop one antidepressant and switch to another. Further, antidepressants might be withdrawn when the passage of time reveals that the initial diagnosis is incorrect (e.g. the patient has bipolar rather than unipolar depression), the patient’s mood is destabilised by the antidepressant or they have responded to treatment and remained well for an extended period.
Switching or stopping antidepressants can pose specific challenges, as almost all antidepressants have the potential to cause discontinuation syndrome if they are ceased or the dose is reduced suddenly. This article discusses some of the issues to consider in making the decision to switch or stop antidepressants and the strategies that may be helpful in meeting the challenge.
Considerations before switching or stopping antidepressants
Before switching or stopping antidepressants because of adverse effects it is important to consider how serious the effects are and whether they might be an initial transient response or a result of an excessive dose or a drug interaction. If the treatment response is inadequate then consider whether the antidepressant has been taken at a high enough dosage for a sufficient period of time and whether the patient is adherent with therapy.
Could adverse effects be transient?
When initiating antidepressants, particularly the commonly used selective serotonin reuptake inhibitors (SSRIs) or serotonin and noradrenaline (norepinephrine) reuptake inhibitors (SNRIs), there may be a transient initial worsening of anxiety and depressive symptoms. These mainly serotonin-linked symptoms can include anxiety, agitation, panic, insomnia, increased dreaming, restlessness, mood elevation, irritability and an increase in suicidal ideation or intent. The last is usually transient, mild and followed by a decrease in suicidal ideation as the antidepressant starts to ‘work’. For some patients, however, the increase in suicidal thinking can be more marked and distressing, with a short-term need for closer care at home or, if indicated, in hospital, for their safety. Nausea is also a common adverse effect of antidepressants in the first few days but usually settles quickly. It is less common if the medicine is started at a low dose.
The emergence of these symptoms in the first few days of therapy can dissuade some patients from continuing treatment. Patients with an obsessional nature or somatic focus may be particularly sensitive to adverse events. However, a careful explanation of adverse effects is usually sufficient for patients to continue treatment.
Most antidepressants can be increased to a therapeutic level within about one to two weeks. Antidepressant doses that are not tolerated when the medicine is initiated may well be tolerated after a week or two.
Clinicians should not fail to treat depressed patients because of a concern about the possibility of these symptoms, as untreated depression is much more likely to be serious and disabling. Patients should be warned about the chance of adverse events and the likelihood that if any occur they will be mild and transient.
Are adverse effects related to excessive dosing or drug interactions?
Clinicians should beware of the potential toxicity of higher doses of antidepressants. For example, tricyclic antidepressants and the tetracyclic antidepressants mirtazapine and mianserin can have excessive anticholinergic effects, causing dry mouth, blurred vision or problems with thinking (e.g. slowed cognition, impaired executive function, fogginess, confusion and indecision). Tricyclic antidepressants can also have quinidine-like effects on the heart, which can cause arrhythmias. Antidepressants can also interact with other medications that the patient is taking, warranting a change of antidepressant or a change in the other medications. For example, SSRIs can interact with tramadol, causing serotonin syndrome.
Serotonin syndrome is an uncommon but serious adverse event associated with antidepressants, especially serotonergic antidepressants such as the SSRIs and SNRIs. Serotonin syndrome can manifest with sweating, tremor, tachycardia, hyperthermia, hypertension, muscle rigidity and delirium. Hallucinations can also occur and persist until drug levels fall.
Serotonin syndrome can arise through overdose with serotonergic antidepressants or through interactions between these antidepressants and other drugs, such as tramadol. Serotonin syndrome is quite different from the more common, mild, self-limiting serotonin-linked symptoms noted above. It is important not to misinterpret serotonergic symptoms such as anxiety and agitation as indicating a need to increase the antidepressant dose, rather than potentially signifying toxicity that warrants a dose reduction.
Some practitioners believe that very high doses of antidepressants can be more effective than doses within the therapeutic range recommended in the manufacturer’s product information (PI). Although patients differ in the metabolism, excretion and transfer of antidepressants across the blood–brain barrier, rarely do they need doses substantially higher than those recommended in the PI. Nevertheless, some patients appear to do better with doses that are a little higher than the recommended range. If considering a dose above the recommended range then seeking the opinion of a psychiatrist is recommended.
Is the dosage adequate?
When commencing a patient on an antidepressant, it is recommended to start at a low dose to improve tolerability and then to increase the dose gradually to a target therapeutic level as the patient tolerates the medication. This ‘start low, go slow’ strategy is helpful to transition patients safely to an effective dosage.
However, some patients remain on an inadequate dose for weeks or months, with continued disability, rather than increasing the dose under medical guidance to a therapeutic dosage. They may then cease the medication as they consider it ineffective when it might have been effective at a higher dose. Treating a patient with subtherapeutic doses that lead to an inadequate response could result in changing from antidepressant to antidepressant, with no one agent being prescribed at a sufficient therapeutic dose to show a benefit.
Has duration of use been adequate?
If a patient has shown no response after taking an antidepressant at a therapeutic dose for two to three weeks then a dose increase should be considered. This can be up to the upper limit recommended in the PI. If the antidepressant has the potential to be effective in that patient then a response would be expected to begin to appear within a further two weeks, and certainly after a further four weeks.
If the patient shows no response after an adequate duration of treatment, such as four weeks on a sufficient therapeutic dose, then the medicine should be reduced and ceased. An alternative antidepressant can then be tried. Medicines should not be switched after just one week of therapy, unless there is an adverse event that is intolerable to the particular patient.
Is the diagnosis correct?
Bipolar rather than unipolar depression
Although some patients with bipolar disorder may present first with a manic episode, others may experience several depressive episodes over years before their first episode of mood elevation. These episodes can appear at first sight to be similar to a unipolar depressive episode and consequently the patient can be misdiagnosed with unipolar depression. However, there is usually a history of mood elevation of greater or lesser degree (hypomania or mania), and the diagnosis of bipolar disorder may become clear with the passage of time.
Antidepressants may be efficacious in the earlier phase of bipolar disorder but over time they tend to become less and less useful. Patients with established bipolar depression tend not to respond to antidepressants or to respond for only a few weeks or sometimes a few months before the response ceases. As a further complication, patients with bipolar disorder treated with antidepressants may find the antidepressant destabilising, predisposing to mania (switching), rapid cycling or a mixed state with simultaneous elements of both mood elevation and depression. A patient with a mixed bipolar disorder may, for example, present feeling sad, tired, lacking in energy, hopeless, helpless and possibly suicidal, while at the same time being restless, agitated, easily distracted, irritable, with rapid thinking which may go from topic to topic, or they may become loud and sometimes inappropriately angry.
Antidepressants in conjunction with mood stabilisers may help depression in some patients with bipolar disorder, but in most, mood-stabilising therapies should be considered alone. Mood stabilisers include lithium carbonate and sodium valproate. Many of the atypical antipsychotics have mood-stabilising qualities, and bipolar depression may also be helped by the anticonvulsant lamotrigine.
Grief or another response to adverse life events
At first sight, a person who is distressed by a recent event may appear depressed but not actually have a depressive illness. This typically occurs after a loss such as a bereavement or broken relationship but might equally follow failing an examination, not getting a work promotion or being ostracised or bullied. An important group of patients have had adverse childhood experiences, such as physical or sexual abuse or emotional neglect, which render them especially vulnerable to emotional instability, relationship difficulties, impulsivity and self-harm.
For these groups of patients, psychological and social therapeutic approaches are favoured rather than pharmacotherapy. They may well respond rapidly to appropriate intervention, support or achievement of an alternative goal. Patients with a dysfunctional childhood may respond better to dialectic behaviour therapy. Many of these patients do not need antidepressants, and if one has been started then it can often be ceased. Nevertheless, some patients benefit from a combination of psychological therapies and antidepressants, especially those with a more pervasive and remorseless ongoing disabling illness.
Medical problems
It is important to take a full history, thoroughly examine the patient and also conduct baseline investigations to ensure there is no underlying medical cause contributing to the symptoms. Hyponatraemia, hypercalcaemia, hypothyroidism, hyperthyroidism and drug and alcohol problems can all cause psychiatric symptoms. Patients who use illicit drugs such as amphetamines can become depressed as they cease those stimulating agents. Assessment and interventions should address the underlying medical problem.
Has the patient responded to treatment and remained well for sufficient time?
A trial of tapering and stopping antidepressant treatment can be considered for patients who have responded to treatment and remained well for an extended period (ideally at least a year after a first episode of depression and up to five years or longer if they have had recurrent episodes). Although some patients remain in good health off antidepressants for many years, others need ongoing long-term treatment to remain well. Discontinuation of antidepressants shortly after initial recovery is not recommended as it is associated with a high rate of relapse of depression.
For many patients, depression is a recurrent illness so the decision to stop treatment must be carefully considered. Patients should be monitored, and treatment with the same antidepressant recommenced if needed.
What antidepressant should the patient switch to?
Almost any antidepressant may prove a reasonable first choice for a patient with a major depressive episode. The desire to minimise side effects often tempers the first choice. Good tolerability and past response by the patient or a close family member can help suggest the best antidepressant, although a response is not assured. Meta-analyses suggest that some agents, such as mirtazapine, escitalopram, venlafaxine and sertraline, are more effective than others, but all available antidepressants might be effective for any specific individual.2
The suitability of an antidepressant may change over the course of a depressive illness. For example, a sedating agent such as mirtazapine may be beneficial when initiating treatment for a patient whose symptoms include prominent insomnia, yet be too sedating for long-term use. A non-sedating agent such as escitalopram may be difficult to tolerate when treatment begins yet become better tolerated as it continues. Serotonergic agents (particularly SSRIs and SNRIs) can have adverse effects on sexual functioning that many patients find intolerable on recovery, whereas for other antidepressants the anticholinergic effects can prove the most troublesome. A newer antidepressant, vortioxetine, has been shown to improve cognition with recovery, but there are no comparisons to show whether this is a unique property or can occur with other antidepressants.3,4
When changing from one antidepressant to another, there are no good data indicating which classes to switch between. Although a specific antidepressant may have a dominant initial mode of action, for example on the serotonin system, most agents have a cascade of effects across the brain affecting a range of neurochemical processes.
Genetic testing
In general, there is no investigation that can particularly help with optimising antidepressant treatment. Genetic studies of hepatic metabolism of antidepressants have been available for some years but have had limited clinical uptake. A genetic test that assesses both hepatic metabolism and the blood–brain barrier transport mechanism is being launched in the USA but is not yet available in Australia. It is hoped this test may help guide prescribing and double the chance of choosing the appropriate antidepressant at the correct dose, but supporting evidence is currently limited.5 With guided prescribing the need to switch antidepressants might be reduced.
Combining antidepressants
If an antidepressant is not effective then it should be ceased. However, antidepressants are sometimes combined when patients have not responded to several single antidepressants. There are limited data suggesting that combining antidepressants results in better outcomes. The combination of venlafaxine and mirtazapine showed a response rate of less than 14% in the Star*D study.6 Such combinations may predispose to adverse events such as serotonin syndrome or unacceptable hypertension or hypotension. If considering combining antidepressants then it is worth seeking an opinion from a psychiatrist.
Discontinuation syndrome
Discontinuation symptoms usually begin within two or three days of appreciably lowering the dose or discontinuing an antidepressant. Symptoms vary between drugs and between patients. Some antidepressants can usually be discontinued uneventfully, such as moclobemide and agomelatine (which have very short half-lives) and fluoxetine (an SSRI with a long half-life). Other antidepressants are particularly likely to result in discontinuation syndrome, notably venlafaxine, desvenlafaxine and paroxetine. However, some patients appear to experience discontinuation syndrome after stopping almost any antidepressant.
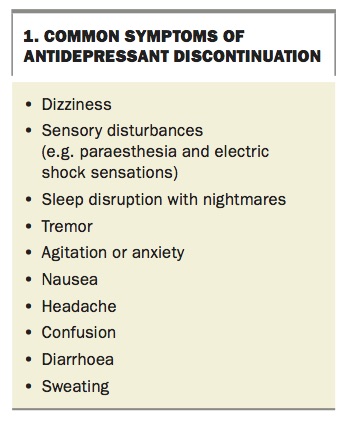
Common discontinuation symptoms are listed in Box 1. In most patients, symptoms are mild and settle within a few days, but for some they can be severe and distressing and last for one to two weeks before resolution.
{kind=link}
Managing discontinuation symptoms
Slowly tapering a drug can minimise discontinuation effects, although not in every case. The possibility of these effects should be explained to patients, emphasising that they are self-limiting and in most cases do not warrant any further medication to settle them. Pausing the tapering of an antidepressant until the discontinuation syndrome settles before the next dose reduction may reduce the severity of adverse events but prolongs the transition to another antidepressant. Short-term use of a benzodiazepine or atypical antipsychotic may reduce the subjective experience of discontinuation but adds complexity and other potential adverse events and is best avoided if possible. Patients should avoid reinstating an ineffective medication to minimise the discontinuation syndrome as this will prevent them transitioning to an alternative medicine which might be more effective treatment for their depression.
Impact of discontinuation symptoms on switching
Discontinuation syndrome can interfere with patient adherence when switching between antidepressants. Because discontinuation symptoms may not appear until a day or two after the antidepressant dose has been substantially reduced or ceased, the introduction of a new antidepressant in that time can lead patients to attribute the symptoms to the new medication and consequently to stop taking it.
To avoid this, it is worthwhile waiting if possible for around two to three days after withdrawing one antidepressant, to identify and manage any discontinuation symptoms, before starting the patient on the new antidepressant. Sometimes, clinical imperatives mean that one medication must be discontinued abruptly and the new one commenced, but in these circumstances clinicians should be aware of the potential complications and manage them effectively.
Which switching strategy should be used?
The main switching strategies include a conservative or moderate switch, direct switch and cross-tapering.7,8
Conservative or moderate switch
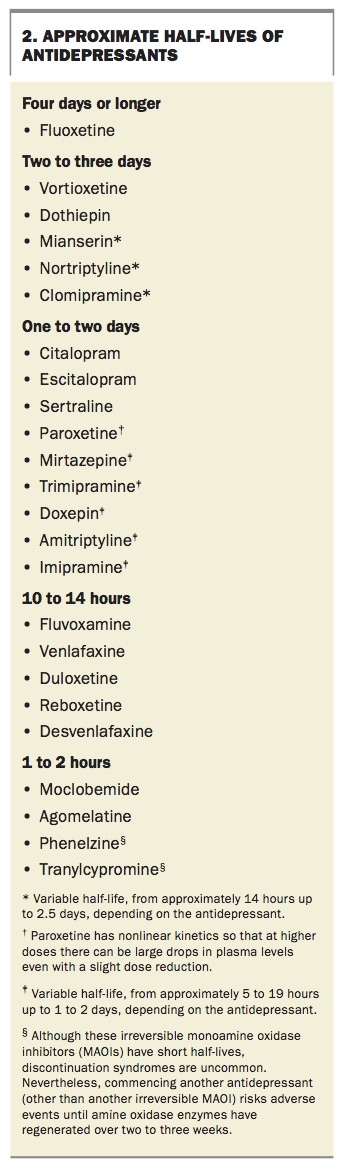
A conservative or moderate switch involves tapering the first medicine and stopping it for five half-lives (conservative switch), or at least a few days (moderate switch), before commencing the new antidepressant. Most antidepressants can be tapered and ceased within one to two weeks, but in rare cases a longer taper of up to a month may be needed. Approximate half-lives of antidepressants are shown in Box 2. Although the half-life can help in determining the risk of discontinuation syndrome, the link is not one to one and some antidepressants with very short half-lives have little risk of causing discontinuation syndrome.
{kind=link}
A conservative or moderate strategy can minimise the chance that patients attribute to the new antidepressant the adverse effects of stopping the first antidepressant, as described above. However, this advantage must be balanced against the risk that the patient will become more depressed because of the delay in starting the new antidepressant.
Direct switch and cross-tapering
The conservative and moderate strategies contrast with the option of abruptly stopping one medicine then immediately starting the next (direct switch). This carries the risk of severe discontinuation symptoms, drug interactions and patient misattribution of symptoms.
A cross-tapering strategy that involves gradually decreasing the dose of the first antidepressant while simultaneously increasing the dose of the new one can help in some circumstances. However, it creates the potential for drug interactions between the two antidepressants.
Factors to consider
Patient safety should always be paramount and sometimes an intermediate transitional strategy will be preferable based on clinical judgement. For example, a clinician might abruptly withdraw an ineffective antidepressant from a patient, find that emerging discontinuation effects are unacceptable and reintroduce the medication briefly to taper it more slowly.
When switching between medicines within a class, such as from one SSRI to another, or one SNRI to another, then it is often possible to transition rapidly without the patient experiencing discontinuation effects. Adverse outcomes seem more likely when patients abruptly discontinue antidepressants such as venlafaxine, desvenlafaxine and paroxetine. Further, patients ceasing therapy with an older irreversible monoamine oxidase inhibitor (MAOI) such as phenelzine or tranylcypromine should wait two to three weeks before starting another antidepressant, to allow time for amine oxidase enzymes to recover and reduce the risk of adverse outcomes such as hypertension.
When should patients be referred?
Most GPs have had excellent mental health training and are well equipped to initiate antidepressant treatment, evaluate patient response, increase dosage if necessary, and discontinue the antidepressant and transition to another if needed. Referral to a psychiatrist is appropriate if the patient:
- is actively suicidal
- is unable to tolerate medications
- is extremely depressed
- has bipolar disorder or psychosis
- has other factors that suggest an increased risk (e.g. marked agitation combined with significant depression)
- has personal factors that would benefit from more specialised intervention (e.g. childhood deprivation or abuse).
Referral to a psychologist for specialist psychological techniques such as cognitive behavioural therapy can be appropriate for patients whose illness includes more psychosocial elements and is less severe. Psychological techniques can be very effective for some patients, whereas others need a combination of psychological treatment and pharmacotherapy.
Shared care can be useful, with the GP dealing with the patient’s day-to-day treatment and the psychiatrist reviewing the patient occasionally to assess progress and the need for other more specialist interventions, a change of medication or a different therapeutic approach. This may be ongoing if long-term treatment is indicated. Usually the patient is referred back to the primary treating GP at the end of specialist care or concurrently, with ongoing specialist care if long-term treatment is indicated. Most patients are successfully treated in the community, although multiple trials of antidepressants may be necessary for some patients before finding the appropriate agent. A small proportion of patients will need a period of hospitalisation.
Conclusion
There is no one ideal antidepressant for all patients so doctors often have to stop or switch their patients’ antidepressants. Efficacy, potential adverse effects, patient factors and prior experience of antidepressants will help determine the choice of antidepressant. ‘Start low and go slow’ when prescribing an antidepressant and attain an adequate dosage. If the response is inadequate after a reasonable period of time then change to another antidepressant. Consider potential long-term as well as acute adverse events, and do not confuse brief discontinuation syndromes with a relapse. Review the diagnosis if there is no response, in case other physical, personal or social factors are influencing the clinical presentation. Consider a slow taper before stopping an antidepressant. When switching antidepressants consider the appropriate balance for each patient between an abrupt transition and a slow tapering and cessation of one medicine before commencing the next one. MT
References
1557-1567.