An updated guide to contraception. Part 3: Permanent methods, traditional methods and emergency contraception

Women's health
Permanent methods of contraception have high efficacy but their usage is falling, which may relate to increased awareness and uptake of long-acting reversible contraception. Traditional methods – the barrier methods, fertility awareness methods, withdrawal and lactational amenorrhoea – remain valued options despite lower efficacy in typical use than modern methods. Emergency contraception has an important role in reducing the number of unintended pregnancies.
- The use of permanent contraceptive methods is decreasing with the increasing availability and acceptability of long-acting reversible contraception.
- Barrier methods, including male and female condoms and diaphragms, require sustained motivation and correct use to be effective contraceptives.
- Condoms (male and female) offer good protection against sexually transmitted infections but use of an additional contraceptive method is usually recommended to ensure good contraceptive efficacy.
- Fertility awareness methods require an understanding of the female reproductive cycle and a commitment to daily vigilance of physical changes, signs and symptoms.
- Women wishing to avoid an unintended pregnancy should be provided with information about emergency contraception, including its mode of action and where to access it.
This third and final article in an updated series on contraception provides practical information about permanent contraceptive methods, barrier methods, fertility awareness methods (FAMs), withdrawal and lactational amenorrhoea. Apart from sterilisation, each of these methods has relatively low efficacy in typical use compared with modern methods, particularly long-acting reversible contraception (LARC).1 However, it is important to acknowledge their role within the range of options available to women and their partners. Women may value the nonhormonal nature of these methods, but they should also be made aware that the nonhormonal copper intrauterine device (IUD) is a highly effective, reversible alternative.
Emergency contraception is also discussed in this article. It plays an important role after unprotected intercourse or contraceptive mishap. Informing women about its availability is an important part of all contraceptive consultations.
The first article in this series covered short-acting methods (the combined hormonal contraceptives and the progestogen-only pill) and the second article discussed the LARC methods and depot medroxyprogesterone acetate injection. These articles were published in the October and November 2018 issues of Medicine Today.2,3 The series is based on the fourth edition of Contraception: an Australian Clinical Practice Handbook.4
Permanent methods
The uptake of permanent contraceptive methods – female and male sterilisation – appears to be decreasing as the use of LARC methods increases. Despite the potential for reversal of some permanent methods, success cannot be guaranteed and the process can be costly. These methods should therefore be regarded as irreversible.
Decision making about permanent methods
The decision to have a permanent contraceptive procedure does not require partner consent. Although a partner may be present in the consultation, it is important to also talk with the individual alone about their decision, to ensure it has not been coerced.
Important considerations to raise before referral for a procedure are listed in Box 1. Future regret is more likely in younger women, nulliparous women and those for whom there is relationship disharmony.5-7 Women requesting intrapartum, immediate postpartum or postabortion procedures should be made aware of the increased rate of regret and a possible increased failure rate, and deferral of the procedure is advised where possible.6,8 Men considering vasectomy can also be made aware of sperm storage facilities that are available at most fertility clinics.
{kind=link}
Female and male permanent methods are classified by law in all Australian states and territories as special medical treatments. If a person lacks the capacity to consent to the procedure, the decision to proceed can only be made under the direction of the appropriate state or territory authority.
Female tubal sterilisation
Female sterilisation is achieved by occluding or disrupting fallopian tubal patency to prevent the sperm fertilising the egg. Techniques include ligating or removing a section of the fallopian tubes, mechanical blockage using clips and coagulation-induced blockage using electrical current or chemicals. The method used will depend on the expertise and preference of the gynaecologist, as well as the woman’s medical, surgical and obstetric history and personal preference. There is an association between tubal ligation and a reduction in the risk of ovarian cancer. A bilateral salpingectomy is sometimes performed, which appears to further reduce the risk of ovarian cancer.9,10
Filshie clip application or other tubal ligation, obstruction or destruction methods can be carried out laparoscopically or via laparotomy under general anaesthetic. They can be performed via mini laparotomy for postpartum sterilisation or at the time of a caesarean section. These methods have a failure rate of less than 0.5% per year, although some studies show a small increased failure rate in younger women, particularly those aged under 30 years.8,11,12
The Essure method, which involved the hysteroscopic placement of microinserts into each fallopian tube to induce permanent occlusion, has not been used in Australia since February 2018. Women and health professionals with any concerns about the Essure device can contact Bayer on 1800 008 757.
Risks and side effects
Tubal sterilisation carries surgical and anaesthetic risks, including injury to the bowel, bladder or ureter and unsatisfactory placement of clips. Mortality rates for tubal sterilisation are low (about four in 100,000 procedures).13
There is a small risk of failure with female sterilisation and, if a pregnancy does occur, the probability of an ectopic pregnancy is increased. Women who have had a pregnancy after sterilisation are at increased risk of another failure.
There is no conclusive evidence that female sterilisation methods are associated with changes to the menstrual cycle, such as heavier bleeding or an earlier age of menopause.14
Reversal
The method of female sterilisation affects the outcome of reversal. Reversal is most likely if clips have been applied to the mid-isthmus portion of the tube and much less likely with tubal destructive or excisional procedures. Hysteroscopic transcervical occlusive methods and bilateral salpingectomy are completely irreversible. Even after reversal, only about 50% of women will achieve a live birth, with much lower rates in those aged 40 years or older compared with younger women.12,15,16 There is a role for assisted conception techniques in women who have had sterilisation procedures.
Male sterilisation (vasectomy)
A vasectomy interrupts the vas deferens to prevent sperm travelling to the ampulla to mix with the prostatic and seminal vesicle fluids. Each vas is mobilised and transected through a single or bilateral scrotal incision. In ‘no-scalpel’ vasectomy, a puncture is made through the scrotum and widened sufficiently to externalise and transect the vas. Compared with the standard vasectomy technique, the no-scalpel approach results in less bleeding, a lower risk of infection, less pain during or after the procedure, a shorter operative time and a faster resumption of sexual activity.17 Vasectomy is usually carried out in the outpatient or clinic setting by trained practitioners. Significant medical problems or a history of scrotal or inguinal surgery or trauma usually require referral to a specialist setting. Precautions are required for previous scrotal injury, a large varicocoele or hydrocoele, inguinal hernia, cryptorchidism or clotting disorders.
Postvasectomy semen analysis is performed at 12 weeks and after a minimum of 20 ejaculations to ensure there are no sperm present in the ejaculate. A small proportion of men do not achieve azoospermia but have very low counts of nonmotile sperm; in these cases, cautious assurance can be provided in collaboration with the vasectomy provider.18
Vasectomy has a failure rate of 0.1 to 0.15%.1 Failure can occur due to technical errors, recanalisation (which occurs in about 0.2% of procedures) or unprotected intercourse before azoospermia is confirmed by semen analysis at 12 weeks.
Risks and side effects
The risk of immediate complications with vasectomy procedures is low, but complications may include pain, local bruising, infection and haematoma. A small haematoma can be managed with bed rest, elevation and support, cold compresses and analgesia. A large haematoma usually requires surgical drainage. Infection can result in an abscess requiring surgical drainage. Epididymo-orchitis results in rapid painful enlargement of the scrotum and is treated with antibiotics and scrotal support. Haematospermia and haematuria are rare and usually settle.
In the longer term, tender or nontender sperm granulomas may develop at the site of the vas division but are usually clinically insignificant. There is no evidence of an increased risk of testicular cancer or a causal association between vasectomy and prostate cancer, nor of any association with subsequent sexual dysfunction.19-21 Antisperm antibodies are found in most men who have undergone vasectomy, but there is no evidence of immunological disease or other adverse outcomes related to their presence.22,23
Reversal
Vasectomy reversal with microsurgical techniques results in a return of sperm to the ejaculate in 85 to 90% of men, although only about 60% of couples go on to achieve a pregnancy.11 The chance of a successful reversal appears to diminish with increasing time since the procedure and increasing age of the female partner.24 Although antisperm antibodies are common, there is no evidence they affect fertility after vasectomy reversal.25
In vitro fertilisation with intracytoplasmic sperm injection can also be considered by couples as an alternative to vasectomy reversal.
Barrier methods
The male condom
The male condom is a single-use sheath that is rolled onto the erect penis before intercourse and collects ejaculate and pre-ejaculate secretions in the space at its tip. Male condoms are easily accessible and relatively inexpensive. They are available in different sizes, colours and flavours, and most are made of thin latex rubber. Nonlatex condoms are an acceptable alternative for people with latex allergy or an aversion to or reluctance to use latex condoms. These may be made of polyisoprene or polyurethane but are more expensive and may be more susceptible to breakage than latex condoms.26
Although the male condom is self-lubricated, additional water-based lubricant may be applied to the outside. Oil-based lubricants, such as vaseline, should be avoided with latex products because they increase breakage.27,28
The male condom is also effective at reducing the risk of sexually transmitted infections (STIs) and can be used simultaneously with other contraceptive methods, except for the female condom (due to an increased chance of breakage and slippage), to provide dual protection against STIs and unintended pregnancy. So-called natural condoms made from animal products (e.g. lamb intestines) are not recommended as they do not provide protection against STIs and have not been approved for use by the TGA.
Male condoms are an effective contraceptive method when used correctly and consistently. The percentage of women in whom pregnancies occur in the first year of use of male condoms is 2% in perfect use and 13% in typical use.1,29 Effectiveness increases with user familiarity and experience.30 Improving condom negotiation skills and self-efficacy is an important strategy to increase effective condom use. Emergency contraception can be advised if there is condom breakage or slippage.
The female condom
The female condom is a loose-fitting lubricated nitrile sheath, with a flexible ring at each end, which collects ejaculate and pre-ejaculate secretions (Figure 1). It is available in a single size and recommended for single use only. It is inserted into the vagina before intercourse, and the penis is guided into the sheath. The inner ring at the closed end of the sheath is firm and slides into the vagina to act as an anchor; the outer ring at the open end spreads over the vulva. Allergy and irritation are rare, and additional water- or oil-based lubricant can be used if required. The condoms are quite slippery, so practice before use during intercourse may be useful.31
{kind=link}
The female condom protects against STIs and can be used at the same time as other contraceptive methods (except for the male condom) to provide dual protection against STIs and unintended pregnancy.
The percentage of women in whom pregnancies occur in the first year of use of female condoms is 5% in perfect use and 21% in typical use.1 As with the male condom, using the female condom requires negotiation and, to be effective, consistent and correct use. Emergency contraception is advised if the condom is displaced or torn during intercourse.
Features that can make the female condom an attractive option include that:
- it allows enhanced transmission of body heat, which may improve sensitivity
- its use does not rely on a male erection, so it may be useful with erectile dysfunction
- the penis does not need to be withdrawn while still erect
- it can be inserted many hours before sex.
Features that may limit its use include that it:
- is more expensive than male condoms (about $3 each)
- has limited availability in pharmacies (it is also available from family planning clinics and online).
The diaphragm
The diaphragm is a silicone dome with a flexible rim that a woman inserts into the vagina to cover the cervix. It prevents sperm transport through the cervix and must be kept in place for at least six hours after intercourse for spermatozoa to be incapacitated in the acidic vaginal environment.4 There is only one brand of diaphragm available in Australia, which is a single-size diaphragm said to fit 80% of women. The manufacturer recommends using the accompanying lactic acid gel on the inner side of the diaphragm.
A diaphragm costs about $90 and lasts up to two years, and the gel costs $30 for an 80 g tube with a shelf-life of three months. Multisize diaphragms, cervical caps and latex diaphragms are no longer sold in Australia.
As the diaphragm can be inserted many hours before intercourse, it does not necessarily interfere with sexual spontaneity. Some women choose to use their diaphragm almost continuously, with removal for washing at least once every 24 hours. This practice is only advised for nonmenstruating women because of the small risk of toxic shock syndrome during menstruation.32 Women using the diaphragm during menstruation are advised to remove it as soon as practical after the six-hour minimum requirement.
The diaphragm has a lower effectiveness, even with perfect use, than many other contraceptive methods, and it has not been shown to provide any protection against STIs. The percentage of women in whom pregnancies occur in the first year of use of the diaphragm available in Australia are 14% in perfect use and 18% in typical use.33 Effectiveness depends on sustained motivation to use the diaphragm with each act of intercourse, and it is a method best suited to women with reduced fertility or those who are accepting of its relatively high failure rate. Emergency contraception is advised if the diaphragm is displaced or damaged during or after intercourse (see case study in Box 2).
{kind=link}
Contraindications
The diaphragm has no significant medical contraindications to its use apart from a history of toxic shock syndrome.32 Although toxic shock syndrome is rare, a small case-control study suggested a possible increased risk in women using a diaphragm or cervical cap during menses.34 Allergy to silicone is extremely rare.
Vaginal or uterine anatomical anomalies, including prolapse, may compromise the correct placement of the device. Some studies suggest an increased risk of urinary tract infection with diaphragm use, particularly in women with recurrent infections, although it is difficult to assess the strength of the association because intercourse itself can result in urinary tract infections.35,36
Ensuring the correct ‘fit’
To use a diaphragm correctly, a woman must feel comfortable with inserting the device and confident about feeling the cervix through the diaphragm to ensure it is covered. Now that multisized diaphragms are no longer readily available in Australia, women can purchase the single-size diaphragm without the traditional ‘fitting appointment’ with a trained doctor or nurse. However, family planning organisations recommend that, where possible, women are supported by a health professional familiar with diaphragm fitting before use, to ensure it fits properly and the woman is inserting it correctly.
Spermicide use
Spermicidal products are not available in Australia.
Fertility awareness methods
FAMs include all methods based on identifying the fertile phase of the menstrual cycle. They rely on predicting the times in the menstrual cycle when a couple should abstain from unprotected vaginal intercourse. FAMs provide an alternative for women and their partners who prefer to avoid other methods, as well as those with religious beliefs that discourage the use of other contraceptives. They do, however, require a thorough understanding of the female reproductive cycle and a commitment to maintaining daily vigilance of fertility indicators.
FAMs are usually unsuitable for women with irregular or anovulatory menstrual cycles, including those who are breastfeeding or perimenopausal. Their effectiveness may also be affected by life events that have a physiological impact on the menstrual cycle, such as illness.
The effectiveness of FAMs has not been documented in the same way as for other methods of contraception.37,38 Effectiveness rates with perfect and typical use are not available for all FAMs. The percentages of women in whom pregnancies occur in the first year of use of the various methods are quoted as varying from 0.4 to 25%.1
Identifying the fertile phase of the cycle
The fertile phase can be defined as the days of potential fertility for a couple during each menstrual cycle: the time from the first act of intercourse that may lead to pregnancy to the demise of the ovum.
The survival of sperm in the female genital tract depends on the presence of alkaline cervical mucus. Although sperm survive for only a few hours in the more acidic environment of the vagina, if there are fertile cervical secretions, they can typically live up to five days in the upper reproductive tract. By seven days, there is a less than 1% probability of sperm survival.39 In contrast, the lifespan of the ovum is short, with fertilisation unlikely to occur beyond the day of ovulation.39
Overview of fertility awareness methods
The FAMs can be broadly classified as symptoms-based methods, calendar-based methods or a combination of these.
If desired and acceptable, some FAMs can be used in combination with barrier methods to enhance effectiveness and to increase the days during which the couple can safely have sex.
Women who choose to use FAMs should be encouraged to seek advice and coaching from an expert educator. Contact details can be found at the Australian Council of Natural Family Planning website (www.acnfp.com.au).
Symptoms-based methods
Temperature method
The temperature method is based on detecting the rise in body temperature (of 0.2 to 0.5°C) caused by increased levels of progesterone after ovulation. This temperature will remain elevated until the next menstrual period. The woman’s basal body temperature (BBT) must be measured immediately on waking and recorded on a fertility chart (Figure 2). Illness, alcohol consumption, too much or too little sleep and use of electric blankets can all raise the BBT.
{kind=link}
The beginning of the fertile time cannot be identified; ovulation is determined retrospectively. Intercourse is avoided from the start of menstruation until there are three consecutive days of recorded temperatures that are higher than the preceding six days. This marks the end of the fertile time, after which it is considered safe to have unprotected sex. Use of this method alone may require many abstinent days.
Mucus methods
Mucus methods are based on daily observation of the mucus secretions at the vaginal introitus, as well as a sensation of wetness or dryness at the vulva. Variations include the Billings ovulation method and the TwoDay Method.40-42
Three patterns of mucus are recognised:
- postmenstrual infertile pattern, with dense, flaky, sticky mucus and a feeling of dryness at the introitus
- ovulatory or fertile pattern with rising oestrogen levels as ovulation approaches, and with clearer, more watery and elastic mucus (similar to egg white) and a feeling of wetness at the introitus
- postovulatory pattern related to the rising level of progesterone immediately after ovulation, causing the mucus to become cloudy, thicker and sticky, with a feeling of dryness at the introitus.
Intercourse is avoided on the days of subjective heavy menstrual bleeding. Intercourse is permitted on alternate evenings during the time of the postmenstrual infertile mucus pattern, then avoided once the fertile pattern is detected, until three consecutive dry days have occurred.
Symptothermal method
The symptothermal method uses a combination of two or more signs of fertility, including changes in temperature and cervical mucus secretions. The primary indicator of the beginning of the fertile phase is the presence of fertile mucus (clear, watery, elastic mucus), whereas the end of the fertile phase is confirmed by a combination of BBT and mucus changes.
Calendar-based methods
These methods rely on documenting the menstrual cycle, often to predict future cycles. There are several tools available to help with calendar methods, including a colour-coded system of beads (www.cyclebeads.com) and smartphone apps. As there is variability in the day of ovulation between cycles, calendar-based methods are inherently less effective than symptoms-based methods.
Calendar method
In the calendar (or rhythm) method, at least three consecutive menstrual cycles must be used to calculate an acceptable range of fertile days. A woman’s fertile days are calculated by selecting the shortest and longest cycle lengths, subtracting 21 from the shortest cycle and subtracting 10 from the longest cycle. Unprotected intercourse should be avoided on the fertile days.
The calculation should be reviewed each month if there is variation in cycle length.
Standard days method
The standard days method is a variant of the calendar method. Women who record two cycles outside the range of 26 to 32 days in any year should not use this method. Taking day one as the first day of bleeding, the first fertile day is considered to be day eight and the last fertile day is considered to be day 19; intercourse is avoided on days eight to 19 of the cycle.43
Contraceptive apps
There are many apps available for recording and tracking fertility indicators. Although these are potentially helpful for planning a pregnancy, as well as avoiding one, evidence on their effectiveness is lacking.44 The exception to this is the Natural Cycles app, developed in Sweden. This app uses an algorithm to predict fertile days (red ‘unsafe’ days) and relies on the daily input of menstrual cycle and BBT data, with optional inclusion of luteinising hormone levels. The predictive accuracy of the algorithm increases with increasing data input.45 After three months of use, about 50% of days are considered safe for having unprotected sex. A study of women using the app found a typical-use efficacy of 93%, which is comparable to the typical-use efficacy of the combined hormonal contraceptive pill.46 The Natural Cycles app is licensed as a contraceptive device in Europe and the US but not in Australia. It is now under scrutiny in Sweden because of a higher than expected number of failures. There is insufficient evidence to recommend its use in Australia.
Withdrawal
Also known as coitus interruptus, the withdrawal method is widely used.47 Although not well researched, it may be relatively effective for those experienced with its use. It needs to be used consistently, can interfere with sexual spontaneity and requires the male partner to have control over his ejaculation. Failure can occur even with correct use, because about 40% of men have sperm present in the pre-ejaculate.48
Lactational amenorrhoea method
The lactational amenorrhoea method is the informed use of breastfeeding for contraception. Breastfeeding delays the postpartum resumption of ovulation due to prolactin-induced inhibition of the release of gonadotropin-releasing hormone from the hypothalamus and, hence, luteinising hormone from the pituitary gland.
Lactational amenorrhoea is an important contraceptive method worldwide, especially in countries where access to modern methods is limited. Its effectiveness can be relatively high – up to 98% when all the following criteria are met:
- the woman remains amenorrhoeic postpartum
- it is less than six months since the woman gave birth
- the baby is fully breastfed (no supplements) and there are no long intervals between breastfeeds (no more than four hours during the day or six hours at night, although no definitive guidance exists).49-51
The median time to menstruation in lactating women is about eight to nine months.50 However, as women may ovulate before the onset of menses and the length between nighttime breastfeeds can lengthen unpredictably, use of an additional method of contraception is generally recommended by family planning organisations.
Emergency contraception
Emergency contraception is used to reduce the risk of pregnancy after unprotected sexual intercourse, sexual assault or potential contraceptive failure. All women at risk of unintended pregnancy should be aware of the availability of emergency contraception methods and be provided with information about their time frames and how they work. The available methods include two types of emergency contraceptive pill (ECP) – ulipristal acetate (UPA) and levonorgestrel (LNG) – and insertion of a copper IUD.
It is important for women to know that an ECP is effective beyond ‘the morning after’, although accessing it as early as possible after unprotected sex is encouraged. Unlike the copper IUD, neither ECP provides ongoing contraception, and the dose should be repeated if unprotected sexual intercourse occurs more than 12 hours after it was taken. Repeat use of ECPs is not harmful but may be associated with menstrual disturbance. Information about ongoing alternative methods of contraception should be provided to women accessing emergency contraception (see case study in Box 3).
{kind=link}
Neither ECP increases the risk of an ectopic pregnancy, nor are they associated with a reduction in future fertility.52 They are well tolerated, with few side effects. Headache and nausea may occur, with vomiting in about 1% of women (the dose should be repeated if vomiting occurs within two hours of administration).53
Menstrual disturbance is common after hormonal emergency contraception. Most women have a menstrual bleed within seven days of the expected time, but it may occur a few days earlier or later than expected.53,54 Delayed bleeding is more common with UPA, with bleeding delayed by more than a week in 18.5% of women and three weeks or more in 4%.55
It may be difficult to distinguish between nonmenstrual and menstrual bleeding after hormonal emergency contraception, and a follow-up pregnancy test three weeks after unprotected sexual intercourse can be considered (Box 4). The standard urine pregnancy test (sensitive to a beta human chorionic gonadotropin level of 25 mIU/mL) performed less than three weeks after unprotected sexual intercourse may give a false-negative result.
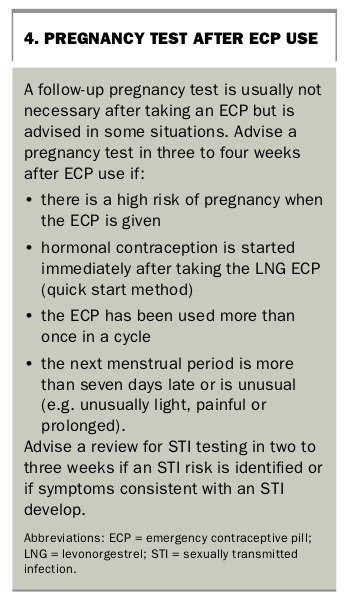{kind=link}
Ulipristal acetate
A new ECP in the form of a selective progesterone receptor modulator, UPA, is available in Australia without a prescription. UPA provides effective emergency contraception for up to five days after unprotected intercourse and has superior effectiveness over the LNG ECP at 24, 72 and 120 hours.56 It acts by preventing or delaying ovulation and, unlike the LNG ECP, can be effective even after initiation of the luteinising hormone surge.57 UPA is generally more expensive than the LNG ECP.
UPA is a single-dose 30 mg tablet. There are no evidence-based contraindications to its use except for hypersensitivity to constituents and known pregnancy (although it is not harmful to an existing pregnancy). Breastfeeding women should generally not take UPA, as the advice to pump and discard breastmilk for one week after UPA administration is impractical. UPA should be used with caution in women with severe asthma treated with oral glucocorticoids because of its high affinity for the glucocorticoid receptor.
The effectiveness of UPA is reduced by progestogen-containing contraceptives, due to progesterone receptor competition, and it is recommended that initiation of these methods be delayed for five days after administration of UPA.58,59 The effect of a high body mass index (BMI) on reducing the efficacy of ECPs appears to be greater for the LNG ECP than for UPA.60 For this reason, a copper IUD or UPA is preferred for women with a weight of more than 70 kg or a BMI of more than 26 kg/m2. If UPA is not available or suitable, a double dose of LNG ECP can be considered, but the evidence to support this is limited.61 Other considerations are noted in the Table, which compares the different emergency contraception methods.
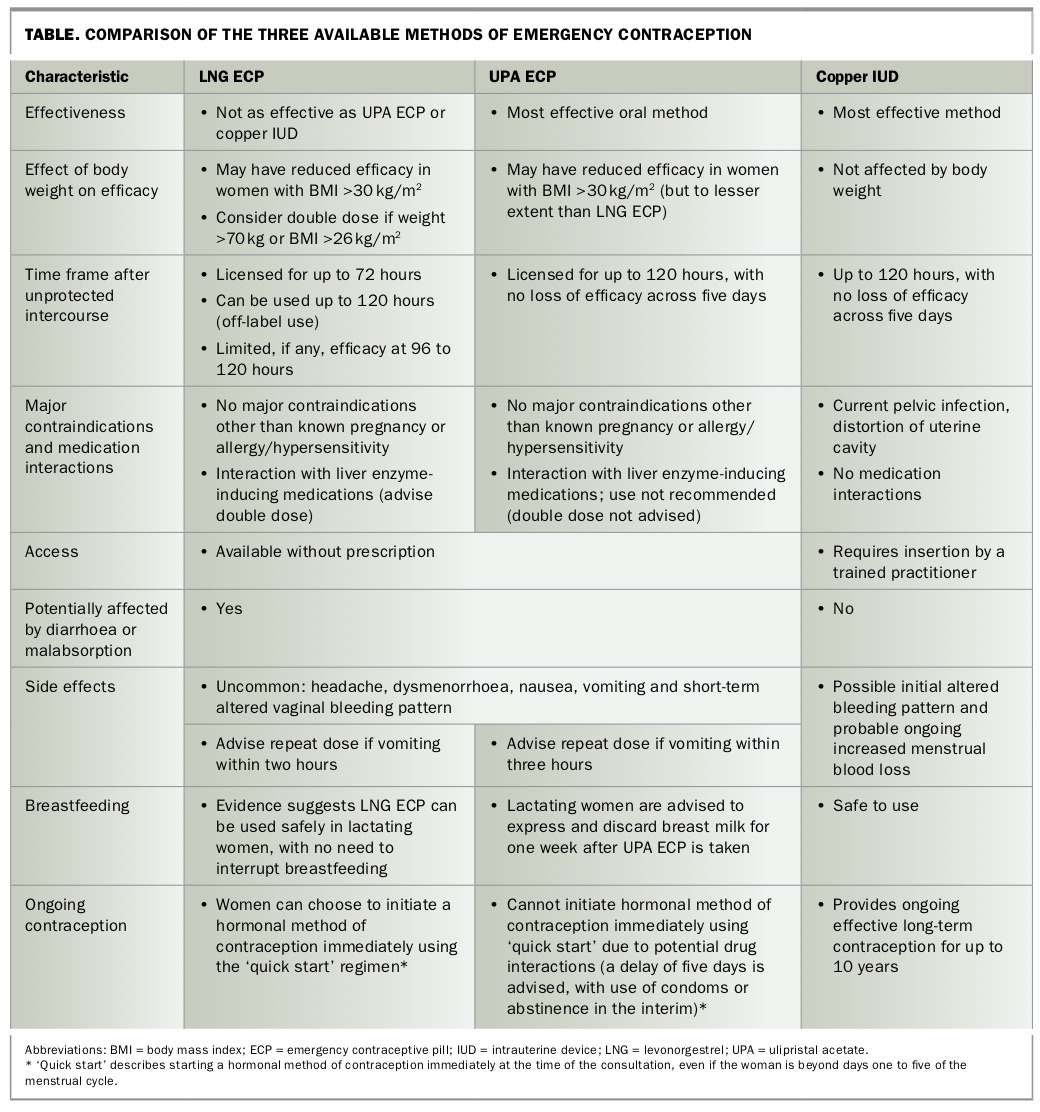{kind=link}
Levonorgestrel ECP
The LNG ECP is a single-dose 1.5 mg tablet of levonorgestrel that should be taken as soon as possible after unprotected sexual intercourse. It is licensed for up to three days after unprotected sex but has some efficacy on day four.62 The LNG ECP acts to prevent or delay ovulation by interfering with follicular development. It appears to have no effect once the luteinising hormone surge has commenced.57 There is no evidence that it prevents fertilisation or inhibits implantation once ovulation has occurred.63
There are no evidence-based contraindications to its use except for hypersensitivity to constituents and known pregnancy, although there is no evidence of harm to a developing fetus if the LNG ECP is inadvertently taken when the woman is already pregnant.64-66 It can be used by women of any age to prevent unintended pregnancy, and there are no medical reasons for restricting its use in those aged under 16 years.32 Women who are breastfeeding can use the LNG ECP off label, with no need to discard breastmilk after administration.67
Women who are using or within 28 days of stopping a liver enzyme-inducing medication (such as carbamazepine and some antiretroviral medications) can be advised to take a double dose (3.0 mg) of LNG ECP (off-label use).68 The copper IUD is the emergency contraception method of choice for women using a potent liver enzyme-inducing medication, such as rifampicin. Common nonliver enzyme-inducing antibiotics do not reduce the effectiveness of the LNG ECP.
Women taking the LNG ECP may choose to initiate an ongoing method of contraception immediately, rather than waiting for the next menses. Using the ‘quick start’ initiation regimen, a hormonal method can be initiated on the same day that the LNG ECP is taken. Additional contraceptive precautions will be required for seven days if initiated at a time other than day one to day five of the menstrual cycle, and a follow-up pregnancy test at four weeks is important to determine emergency contraception failure or contraceptive failure during the first seven days of use.4
Copper IUD
A copper IUD provides the most effective emergency contraception if it is inserted up to five days after unprotected sexual intercourse, as long as an existing established pregnancy can be excluded. The copper IUD interferes with sperm movement, inhibits fertilisation by direct toxicity and may prevent implantation of a fertilised egg. It is more effective (99%) than either of the ECPs and provides ongoing LARC.69 Despite these advantages, the upfront cost and accessing a practitioner for insertion of a copper IUD quickly can be challenging.
Conclusion
GPs play a crucial role in providing evidence-based information on all contraceptive options – including permanent methods of contraception, fertility awareness methods and barrier methods – to support informed choice, with consideration of the range of factors that influence a woman’s individual decision making. These include medical, social and cultural factors, side effects, noncontraceptive benefits, costs and personal preferences. It is important that health professionals and the public are aware of the availability and suitability of all forms of emergency contraception and its role in reducing unintended pregnancies. Printed and web-based information, which is available through the state and territory family planning organisations, should be provided to women during contraceptive consultations. MT