Farewell over-the-counter codeine: the TGA’s upscheduling of low-dose codeine

Pain
Low-dose codeine is now a prescription-only medication in Australia. We are highlighting this article, which featured in a recent Medicine Today supplement, as it includes practical tips for managing patients with codeine dependence.
- Over-the-counter analgesics and cold and flu preparations that contain low-dose codeine were upscheduled by the TGA to Schedule 4 ‘Prescription Only’ from 1 February 2018.
- Codeine alone is a poor analgesic, and there is little evidence to show adding low-dose codeine (<30 mg) to nonopioid analgesics provides additional pain relief.
- Combining simple analgesics (e.g. paracetamol plus ibuprofen) may provide more effective pain relief than adding codeine at higher doses (30 to 60 mg) to paracetamol.
- Codeine dependence is a well-recognised problem in Australia, and can cause serious gastrointestinal, renal and hepatic problems, usually due to excessive intake of ibuprofen and paracetamol in codeine-containing combination analgesics.
- Codeine dependence can be identified by careful questioning regarding recent codeine use patterns, reasons for use and withdrawal symptoms on cessation, and surveillance for signs and symptoms of complications due to overuse of secondary nonopioid analgesics.
- The TGA resource ‘Tips for talking about codeine: guidance for health professionals with prescribing authority’ provides practical guidance for health professionals when talking to patients about codeine, including tips for discussing rescheduling, ongoing pain management options and codeine dependence.
Codeine is a low-potency opioid widely used for its analgesic, antitussive and antidiarrhoeal properties. In Australia, more packets of codeine are sold each year than of all other opioids, with data showing that packs of prescription and over-the-counter codeine accounted for two-thirds of all opioid packs sold in 2013.1
Codeine itself possesses little affinity for the mu-opioid receptor, and therefore relies upon conversion to morphine by the polymorphic cytochrome (CYP) 450 2D6 enzyme to exert is pain-relieving effects. As a result, the analgesic effects and safety of codeine are governed by the patient’s CYP2D6 activity, with poor metabolisers experiencing virtually no appreciable analgesia, ultra-rapid metabolisers being at risk of opioid-related adverse effects and intermediate and extensive metabolisers falling between these two extremes.
Following a comprehensive review and consultation process, the Therapeutic Goods Administration (TGA) determined all combination analgesics that contain low-dose (8 to 15 mg) codeine would be removed from the Schedule 3 ‘Pharmacist Only’ listing and would become Schedule 4 ‘Prescription Only’ medicines from 1 February 2018. Similarly, over-the-counter cold and flu preparations containing codeine as a cough suppressant would be rescheduled from Schedule 2 ‘Pharmacy Only’ to Schedule 4 ‘Prescription Only’.
How effective is codeine in providing pain relief?
Despite codeine being the most commonly consumed opioid globally,2 interpatient variability in the conversion to morphine renders codeine an unreliable analgesic. As with more potent opioids, codeine has a limited role in managing chronic pain and is not recommended for managing migraine. In acute nociceptive pain, codeine as a single agent provides only a marginal benefit over placebo, and is less effective than nonopioid analgesics like NSAIDs.3 The Australian therapeutic guidelines for analgesia suggest adding codeine 30 to 60 mg when moderate pain is not adequately relieved by paracetamol and/or an NSAID.4
The size of the benefit of adding codeine to nonopioid analgesic regimens containing paracetamol and/or anti-inflammatories such as ibuprofen is poorly defined. Evidence to support the incremental benefit of low-dose codeine (<30 mg) in particular is scarce. A recent systematic review commissioned by the TGA found only three randomised controlled trials have compared low-dose codeine in combination with nonopioid analgesics to the same doses of nonopioid analgesics alone, and of these two found no increase in analgesia with the addition of low-dose codeine.5-8
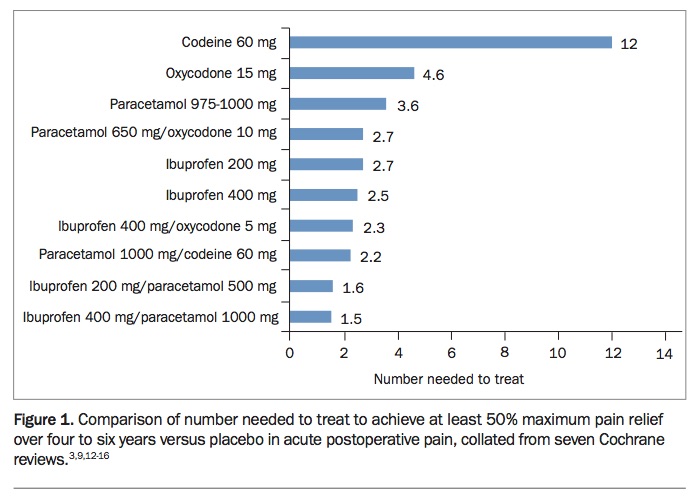
A 2009 Cochrane review reports a number needed to treat (NNT) of 2.2 for paracetamol (1 g) in combination with 60 mg of codeine versus placebo in pain due to inflammation following tissue injury; the addition of codeine increased the proportion of patients achieving at least 50% pain relief by 10 to 15%.9 In contrast, recent studies have not detected such a benefit. In a 2017 trial, codeine 60 mg added to a regimen of paracetamol 1 g and ibuprofen 400 mg did not improve analgesia after third molar surgery, and in a 2016 study, adding either codeine 60 mg or oxycodone 10 mg to a combination of paracetamol 1 g and ibuprofen 400 mg provided no additional analgesia, compared with the addition of a nonopioid control (thiamine).10,11
The efficacy of analgesics in treating acute pain can be crudely compared by reviewing the NNT to achieve 50% maximum pain relief at four to six hours for each product. The NNT to achieve this pain reduction following one dose of a single-agent analgesic or a combination preparation, taken from seven separate Cochrane reviews, is shown in Figure 1.3,9,12-16 Although these collated data do not derive from head-to-head studies, such comparisons highlight the relative efficacy of nonopioid analgesics, especially combination paracetamol plus ibuprofen products.
{kind=link}
What problems are associated with codeine use?
Although codeine was once thought to pose a low abuse potential, codeine misuse and dependence have now been clearly documented in numerous case series and observational studies.17 Such studies report patients taking excessive amounts of codeine, commonly consuming a packet each day and in some cases taking up to 10 times the recommended daily dose, for months or even years.18,19
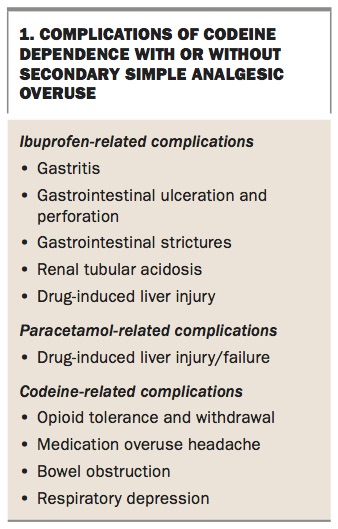
Harms associated with codeine misuse may relate directly to acute opioid intoxication or prolonged high-dose opioid intake. However, many serious observed harms result from the overconsumption of ibuprofen or paracetamol found in codeine-containing combination products. Commonly reported consequences of primary codeine dependence with secondary nonopioid analgesic overuse include gastrointestinal ulceration and perforation with associated bleeding and anaemia, as well as renal and hepatic impairment (Box 1).18,20,21 Codeine dependence can also have social and financial consequences on par with other forms of opioid dependence, impacting on relationships and employment.
{kind=link}
Additionally, some individuals, especially children and ultra-rapid metabolisers, are at risk of experiencing other serious adverse events when given codeine, such as difficulty breathing and death. National Coronial Information System data show increasing rates of fatal codeine-related overdoses in Australia, and that over a 13-year period codeine toxicity was a contributing factor in more than 1400 deaths and the attributed cause of death in 113 cases.22
Why has the TGA decided to upschedule low-dose codeine?
Access to codeine requires a prescription in the USA, Japan, Hong Kong,
India, Russia and most European countries – few countries currently permit over-the-counter supply. Mounting evidence suggests that in countries with less strict regulations around codeine supply there is generally more abuse and misuse of low-dose codeine-containing medicines.
In Australia, discussions about rescheduling of over-the-counter codeine have spanned a decade. The National Drugs and Poisons Schedule Committee formed a Codeine Working Party in 2008, in response to increasing abuse of ibuprofen plus codeine products. In 2010, low-dose codeine-containing analgesics were moved from the Schedule 2 ‘Pharmacy Only’ listing to Schedule 3 ‘Pharmacist Only’, yet this change proved insufficient to limit medication misadventure. In 2015, codeine upscheduling was again on the agenda for the Advisory Committee on Medicines Scheduling, with the initial proposal, the interim decision and the final decision generating much controversy. The final decision to reschedule low-dose codeine products to Schedule 4 – requiring a prescription – was made in December 2016, to be implemented from 1 February 2018.
In view of the evidence, the risks associated with low-dose codeine supplied over the counter, including unpredictable morphine production, codeine dependence and death, were determined to outweigh any extra benefit for low-dose codeine over alternative medicines without codeine, to the extent that over-the-counter accessibility is undesirable. This change also aims to encourage patients with chronic pain in particular to see their GP for a comprehensive pain assessment and management plan, rather than self-managing with codeine.
How common is codeine dependence?
The prevalence of codeine dependence in Australia is unclear. In 2016, 1967 people across Australia reported entering opioid- substitution therapy specifically for codeine dependence. This is no doubt an underestimate of the codeine-dependent population in Australia, as the opioid of dependence was not reported for 36% of substitution therapy patients, and earlier data from an online survey indicate that only a quarter of codeine-dependent Australians have sought treatment.23
How can we recognise codeine dependence?
Detection of codeine dependence is often delayed, contributing to morbidity. Frequently, dependence is not recognised until after the patient presents with serious consequences of analgesic overuse.
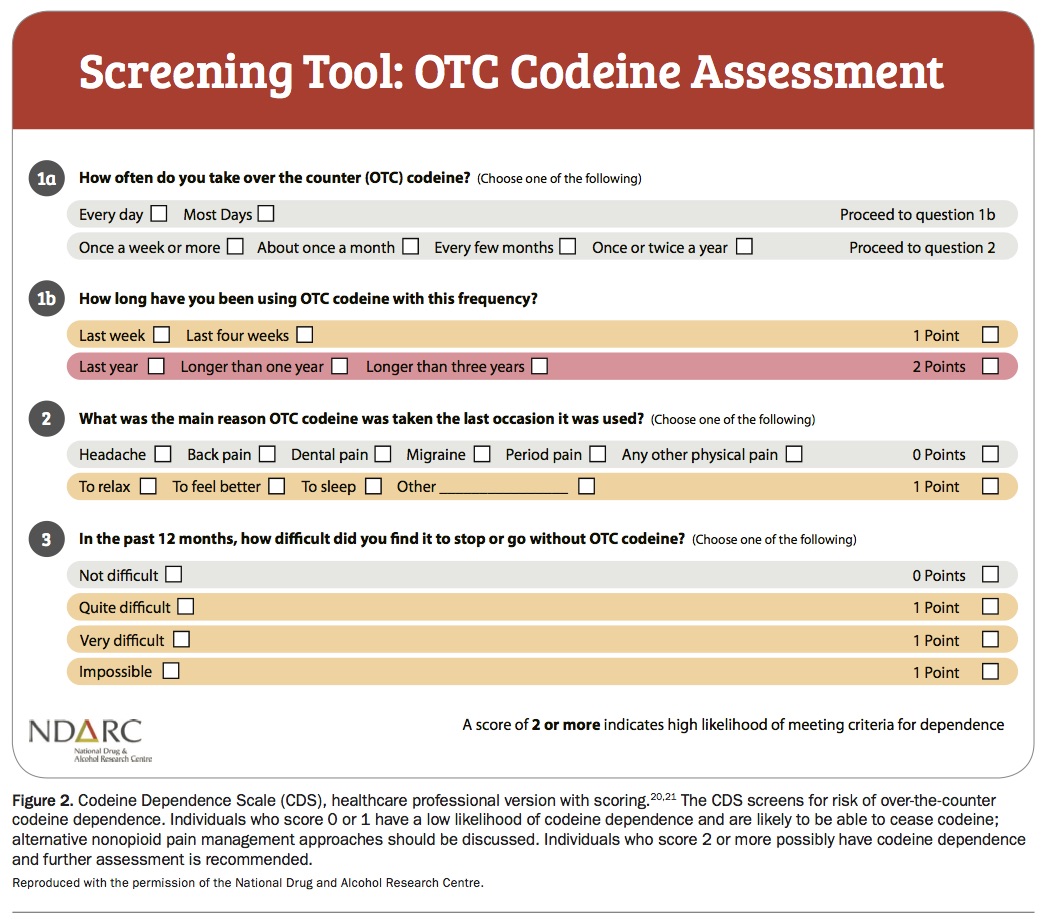
In general practice, careful questioning is required when patients present requesting pain relief, to ascertain past use of over-the-counter codeine and identify when further assessment for dependence is necessary. To aid detection of problematic codeine use, a short four-item screening tool, the Codeine Dependence Scale, has been developed recently by the National Drug and Alcohol Research Centre (Figure 2).24 This tool asks about duration and frequency of codeine use, the reasons for its use and difficulties experienced when stopping it.
{kind=link}
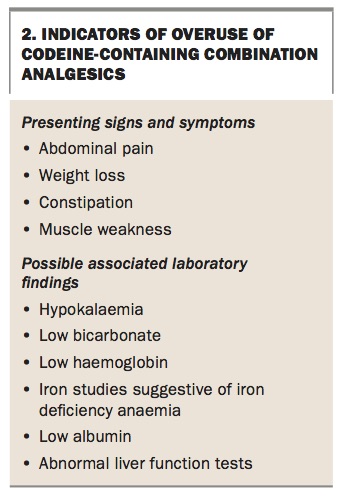
Flags suggestive of the common complications of overuse of codeine-containing combination analgesics can also prompt further questioning regarding analgesic intake. Commonly reported presenting signs and symptoms and laboratory findings in patients with codeine dependence associated with combination analgesic overuse are listed in Box 2.18,20
{kind=link}
How should we talk to patients about codeine dependence?
The TGA has published a useful resource providing guidance for health professionals when talking to patients about codeine, including tips for discussing rescheduling, ongoing pain management options and codeine dependence. This guidance document, titled ‘Tips for talking about codeine: guidance for health professionals with prescribing authority’ is available on the TGA website (https://www.tga.gov.au/tips-talking-about-codeine-guidance-health-professionals-prescribing-authority).
Conclusion
On its own, codeine is a poor analgesic. Its clinical use is limited by low affinity for the mu-opioid receptor and its highly variable metabolism to morphine, which is dependent on an individual person’s expression of the polymorphic CYP2D6 enzyme. Evidence for an incremental benefit when adding low-dose (below 30 mg) codeine to nonopioid analgesics is scarce. Even in higher doses (e.g. 60 mg), in many cases combination analgesics containing codeine appear to be no more effective than combinations of nonopioid analgesics such as paracetamol and ibuprofen.
As with all pharmaceutical opioids, codeine use has the propensity to cause opioid dependence, and codeine dependence is associated with serious and well documented harms. Harms secondary to codeine dependence are increased beyond the consequences of opioid toxicity, as the vast majority of codeine-dependent individuals ingest combination analgesics and therefore receive supratherapeutic doses of nonopioid analgesics as well. Careful questioning regarding codeine use patterns, reason for codeine use and symptoms on codeine cessation, as outlined in the Codeine Dependence Scale, together with surveillance for the signs of nonopioid analgesic toxicity, can identify patients with problematic codeine use for whom formal evaluation for opioid dependence is recommended. MT