Herpes zoster vaccines: the new and the old

Immunisation
A new recombinant herpes zoster subunit vaccine has been shown in clinical trials to be efficacious and safe. It holds promise for reducing the burden of herpes zoster and its complications, particularly the pain of postherpetic neuralgia, for older people and immunocompromised patients, who are most at risk. However, until the new vaccine becomes available in Australia, the existing live attenuated vaccine has an ongoing and important role in clinical practice.
Herpes zoster (HZ), or shingles, is caused by reactivation of latent varicella zoster virus (VZV). During initial infection with VZV, which presents clinically as chickenpox, the cervical and peripheral sensory ganglia become latently infected, probably through the bloodstream. VZV then remains latent in the sensory ganglia for life.1 As 95% of adults in the developed world who were born in the pre-varicella vaccination era have had varicella by the age of 30 years, most are at risk of developing HZ.
HZ is characterised by a dermatomal papulovesicular rash that evolves through pustular and crusting stages, usually accompanied by pain in the same area. Pain may start before the rash appears (prodromal pain) and can persist for weeks to months, even after resolution of the rash, as postherpetic neuralgia (PHN).2 PHN is usually defined as pain of at least moderate severity that persists for more than 90 days after onset of the rash.
The incidence of HZ increases with age, owing to the decline in immunity that accompanies ageing (immunosenescence). About 60% of HZ cases occur in people aged 50 years or older. HZ also occurs more often in patients with immunocompromising illnesses, such as HIV infection, or those receiving chemotherapy, high-dose corticosteroids, biological modifiers or haematopoietic stem cell or organ transplantation. The severity of HZ is related to the degree of immunocompromise.3
The most important complication of HZ is the prolonged and severe pain of PHN, followed by superinfection of the rash, ocular involvement (including uveitis and blindness) and neurological disease. The likelihood of complications also increases with age.4 This is particularly so for PHN, which is less common in those under the age of 50 years. This prolonged severe pain can have a profound effect on the quality of life of many older people.5
The introduction of a live attenuated HZ vaccine was an important advance in reducing the burden of HZ in older adults. However, the declining efficacy of this vaccine with age, especially in those over the age of 70 years, has left a substantial unmet medical need in this growing population. Furthermore, the live attenuated vaccine is contraindicated in severely immunocompromised patients, in whom HZ is common and often severe. The development of a new recombinant subunit vaccine against HZ combined with adjuvants (HZ/su) addresses these issues, but the new vaccine is not yet available in Australia. This article discusses the efficacy and safety of the new recombinant vaccine and provides guidance on what should be done for patients until it becomes available.
New recombinant herpes zoster subunit vaccine
The new recombinant vaccine has some key advantages over the existing live attenuated vaccine. First, its adjuvant system stimulates strong cellular and humoral responses to protein antigens – these immune responses prevent HZ after VZV reactivation in the neuronal ganglia – and circumvents the potential hazards of administering a live but attenuated virus to immunocompromised people. In addition, its simpler manufacture should allow easier supply to the large and increasing ageing population.
HZ/su consists of 50mcg of VZV glycoprotein E and the AS01B adjuvant system.6 Glycoprotein E is the most abundant protein in VZV-infected cells and is essential for viral replication.7,8 However, it was selected as the HZ/su vaccine antigen mainly because it is a major target for antibody and cellular immune responses during VZV infection.9,10 HZ/su also contains the novel AS01B adjuvant system to improve the modest stimulatory immune effect of glycoprotein E alone. AS01B consists of liposomes containing two immunostimulants: MPL (3-O- desacyl-4'-monophosphoryl lipid A) and QS-21 (Quillaja saponaria Molina, fraction 21).11
Phase I and II clinical trials showed that HZ/su could stimulate strong humoral and cellular immune responses to glycoprotein E in adults aged 50 years or older, especially in those over 70 years, and that the adjuvant was essential for these responses.6,12,13 A single dose of HZ/su was found to be clearly immunogenic, but two doses administered two months apart were needed for optimal immune responses.12
Recombinant vaccine efficacy against HZ
Two large phase III studies, the Zoster Efficacy Study in Adults 50 Years of Age or Older (ZOE-50) and the Zoster Efficacy Study in Adults 70 Years of Age or Older (ZOE-70), were designed and conducted with 29,311 participants to assess the efficacy of HZ/su in preventing HZ in immunocompetent adults in two age groups: 50 years or older (ZOE-50) and 70 years or older (ZOE-70).14,15 These blinded, randomised, placebo-controlled studies were conducted in parallel at the same study sites in 18 countries. The participants were followed up for the development of HZ and PHN for a mean of 3.2 years.14,15 The ZOE-70 study was needed to collect additional efficacy and safety data for adults aged 70 years or older, as they are the population at highest risk of HZ and with the highest incidence of PHN.14
In the ZOE-50 study, HZ occurred in six HZ/su recipients (0.3 cases/1000 person-years) and 210 placebo recipients (9.1 cases/1000 person-years), giving a vaccine efficacy of 97.2%.15 In each of the three age strata (50 to 59 years, 60 to 69 years and 70 years or older), vaccine efficacy was similar (96.4% to 97.9%) and statistically significant (p<0.001). In ZOE-70, which was stratified into two age groups (70 to 79 years and 80 years or older), HZ occurred in 23 HZ/su recipients (0.9 cases/1000 person-years) and 223 placebo recipients (9.2 cases/1000 person-years) during a mean follow-up period of 3.7 years, giving a vaccine efficacy of 89.8% (p<0.001).14 These trials show that HZ/su efficacy appears to be unaffected by age at the time of vaccination, with efficacy greater than 90% seen even in participants aged 80 years or older.
In the pooled results from the ZOE-50 and ZOE-70 studies, HZ/su protection was also durable, as its efficacy did not differ significantly between years one to four, at 97.6%, 92.0%, 84.7% and 87.9%, respectively (p<0.001). Long-term evaluation of HZ/su recipients is ongoing to assess the persistence of vaccine efficacy beyond four years.
Recombinant vaccine efficacy against PHN
The ZOE-50 and ZOE-70 studies also examined efficacy of HZ/su against PHN. In the pooled study results, four cases of PHN occurred in HZ/su recipients (0.1 case/1000 person-years) and 46 cases occurred in placebo recipients (0.9 cases/1000 person-years), giving a vaccine efficacy against PHN of 91.2% in adults aged 50 years or older (p<0.001).14,15 Efficacy was similar (88.8%) for those aged 70 years or older (p<0.001). No cases of PHN occurred in HZ/su recipients younger than 70 years, compared with 10 cases in age-matched placebo recipients.14
These studies found that the efficacy of HZ/su was similarly high against HZ and PHN. Its efficacy against PHN is therefore attributable to prevention of HZ, with no additional demonstrable efficacy against PHN in ‘breakthrough’ HZ, unlike with the live attenuated vaccine, although the few cases in vaccine recipients made this difficult to assess.14 However, HZ/su did significantly reduce the severity and duration of HZ-associated pain in those with breakthrough HZ.16 Therefore, HZ/su reduced both the risk of HZ and the severity of pain in vaccine recipients with breakthrough disease.17
HZ/su also significantly protected against other complications of HZ, including disseminated disease, ophthalmic disease (most common), neurological disease including vasculitis and stroke, and visceral diseases. This was mainly achieved by preventing HZ itself rather than by preventing complications in breakthrough disease (one HZ/su recipient and 16 placebo recipients developed an HZ complication other than PHN, giving a vaccine efficacy of 93.7%).18
The number needed to vaccinate with the HZ/su vaccine to prevent one HZ case ranged from eight to 11, and to prevent one case of PHN ranged from 39 to 53.19
Safety and reactogenicity of recombinant vaccine
In the ZOE-50 and ZOE-70 studies, a total of 14,645 adults aged 50 years or older received HZ/su and 14,650 received the saline placebo, allowing direct comparison of serious adverse events. There were no differences in serious adverse events (10.1% vs 10.4%) or fatalities (4.3% vs 4.6%) between vaccine and placebo recipients.14,15,20
As HZ/su contains the previously unlicensed adjuvant AS01B, which could theoretically induce or exacerbate autoimmunity, the incidence of potential immune-mediated diseases was also compared between vaccine and placebo recipients and found to be similar (1.1% vs 1.3%).20 Furthermore, there was no temporal relationship between potential immune-mediated diseases and vaccine administration.
These studies show that HZ/su has an acceptable safety profile in older adults. Post-licensure studies will further monitor HZ/su safety for potential immune-mediated diseases.
Reactogenicity, which may be local at the injection site or systemic, was compared in 4460 HZ/su and 4466 placebo recipients for seven days after administration (Table 1).15 Injection-site reactions were much more frequent in recipients of HZ/su than placebo (81.5% vs 11.9%). The most common local reaction was pain. Systemic reactions, most often myalgia and fatigue, were also more frequent after HZ/su than placebo (66.1% vs 29.5%). The more important reactogenicities are the severe or ‘grade 3’ local and systemic reactions, which are defined as those preventing normal daily activity. These occurred much more frequently in vaccine recipients (local reactions 9.5% vs 0.4%). However, these reactions to vaccine were transient; the median durations were only one to three days overall and one to two days for grade 3 reactions.
{kind=link}
Although the reactogenicity of HZ/su was relatively high, so was second-dose compliance, at about 95% in both the ZOE-50 and ZOE-70 studies.14,15 This was comparable to compliance in the placebo groups (91% of recipients with grade 3 vaccine reactions returned for a second dose). Thus, the vaccine was generally well tolerated.
Recombinant vaccine in immunocompromised populations
Unlike live vaccines, nonreplicating vaccines are safe to use in severely immunocompromised patients. The risk of live HZ vaccine has been highlighted by a report from postmarketing surveillance of several cases of disseminated HZ that occurred in severely immunocompromised patients who received the live attenuated HZ vaccine and were proven to be caused by the vaccine strain.21
HZ/su can be safely used in immunodeficient patients at high risk of HZ. The safety and reactogenicity of HZ/su have been examined in several immunocompromised populations, including autologous stem cell transplant recipients, adults with HIV infection, renal transplant recipients and people with haematological or solid organ malignancies.17,22-24 No safety concerns arose in any immunocompromised group. Furthermore, in all cases, the HZ/su reactogenicity profile was similar to that observed in older adults in the ZOE-50 and ZOE-70 trials and did not affect the underlying disease.
Licensing of recombinant vaccine
HZ/su was licensed in the US, Canada, Europe and Japan in 2017 and in Australia in 2018 for individuals aged 50 years or older. It has now been rolled out in the US and Canada, and demand in those countries is high. A recent cost-effectiveness review of HZ/su in the US showed that, at a price of US$280 per series ($140 per dose), HZ/su would cost less than the live attenuated vaccine.25
Europe and Japan will be the next markets to receive access to the vaccine, with Australia to follow, probably in one to two years.
Other considerations
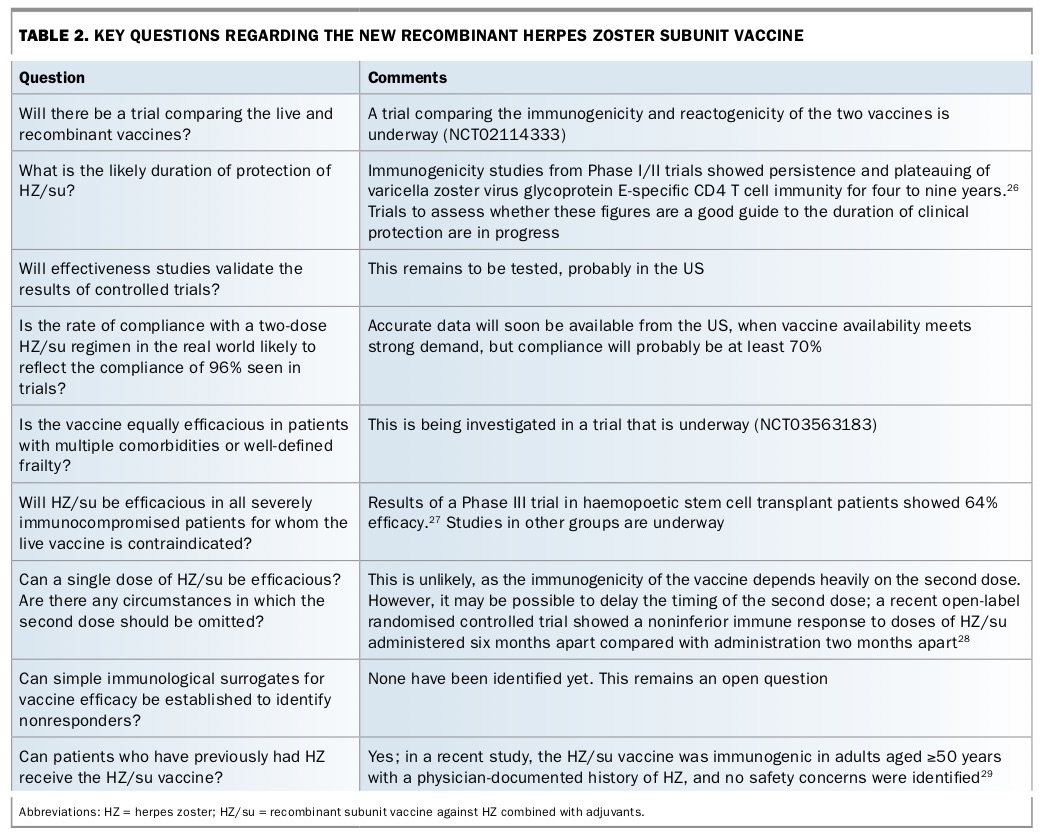
Key questions that are being addressed in clinical trials or are yet to be conclusively answered regarding HZ/su are shown in Table 2.26-29
{kind=link}
The high efficacy of HZ/su suggests that use of one or a few target antigens combined with relevant adjuvants could in future be extended to improve the limited efficacy of other vaccines, such as influenza and pneumococcus vaccines, in ageing people.
What should Australians do while waiting for the new vaccine?
Although the new recombinant vaccine is highly efficacious and safe, it will likely be one to two years before it is available in Australia. Until then, the existing live attenuated vaccine still has an important place in therapy for certain groups of people.
The live attenuated vaccine has an efficacy of about 65% against PHN, although a lower efficacy (51%) against HZ itself.30 Vaccine effectiveness against HZ lasts for eight to 10 years, and probably longer for PHN. The contraindications to the live attenuated vaccine have been extensively outlined elsewhere but include severe immunocompromise, pregnancy and previous anaphylactic reaction to a VZV-containing vaccine or vaccine component.30,31
The live attenuated zoster vaccine is far less reactive than HZ/su, with the latter having a much higher incidence of local reactions (Table 1). Mild injection-site reactions, such as pain, swelling and redness, are likely to occur in about half of patients receiving the live attenuated vaccine.31 Systemic reactions occur in about 24% of recipients.
Older immunocompetent people
The live attenuated vaccine is registered for use in people aged 50 years or older as a single dose. It is particularly recommended for adults aged 60 years or older who are not immunocompromised.31 Vaccination is also recommended for people aged 50 years or older who are household contacts of a person who is or is expected to become immunocompromised.31 It is freely available on the National Immunisation Program for Australians aged between 70 and 79 years. The catch-up program for those aged 71 to 79 years is funded only until October 2021.
Although disease burden is also high in people aged 80 years or older, live attenuated vaccine efficacy is lower in this age group. Nevertheless, real-world evidence has shown that individuals in this age group may still benefit from this vaccine.32
HZ/su, when it becomes available, can be administered to previous recipients of the live attenuated vaccine without increased reactogenicity and with similar immunogenicity, so future administration should not be prejudiced.33
Immunocompromised people
There is currently no vaccine for severely immunocompromised patients, although the live attenuated vaccine can be safely administered two to four weeks in advance of impending immunosuppression. However, this is often impractical.
GPs and other vaccine providers should assess whether a patient is severely immunocompromised. The first step is to complete a prevaccination checklist.31 It is very important that severely immunocompromised patients do not receive the live attenuated vaccine, as there have been several cases of severe morbidity and even death.21
Evidence on safety of the live attenuated vaccine in moderately immunocompromised patients is still accumulating. In some moderately immunocompromised patients, such as those receiving anti-tumour necrosis factor therapy, it seems safe.29,34,35
In adults with haematological malignancies receiving anti-CD20 monoclonal antibodies, an inactivated zoster vaccine was well tolerated and resulted in statistically significant VZV-specific T-cell responses at about 28 days.34 However, it is not known whether or when this inactivated vaccine will become available.
Conclusion
HZ/su is a new vaccine against HZ with two advantages over the currently available live attenuated zoster vaccine. First, it provides much more protection against acute HZ and its major complication, PHN. Second, it is a non-live vaccine, so it can be safely used in immunocompromised patients. Further studies are underway to provide evidence of effectiveness in all major immunocompromised groups.
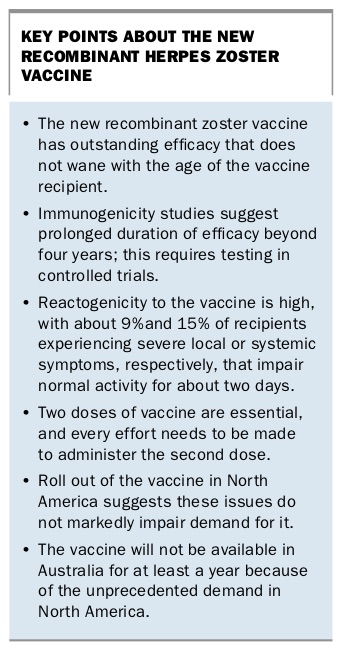
The main drawback of HZ/su is its much higher rate of local reactions (81.5% vs 48.3% overall; 9.5% vs less than 1% for severe reactions) and systemic reactions (66.1% vs 24%) compared with the live attenuated vaccine, although these effects are transient.14,15 In addition, two doses of HZ/su are required to provide protection. The need for two doses and the higher rate of local and systemic adverse effects may influence compliance with HZ/su vaccination once it becomes available in Australia. However, this was not apparent in the trials and has not prevented major demand for the vaccine in North America, where three million doses were dispensed in the first year of licensure. Key points regarding HZ/su are shown in the Box. MT
{kind=link}