Holiday heart: mobile app suggests atrial fibrillation after ‘a few drinks’

Atrial fibrillation
Emergency medical services
The growing use of mobile apps and other devices that monitor heart rate is likely to increase presentations with suspected atrial fibrillation to emergency departments and to GPs.
Atrial fibrillation (AF) is a common presentation to hospital emergency departments (EDs). Many patients are not aware of the relation between AF and alcohol use. Most patients present because of symptoms. In this case, a man presented after self-diagnosis through the use of a smartphone cardiac monitoring app.
Case scenario
Your friends know that you work shifts in the ED of the local hospital as well as in your own general practice. Thus, you are not surprised when one of your friends telephones you about a relative who has been taken to the ED by ambulance with a ‘heart problem’. You promise to check on him during your ED shift later that evening and, after the ED handover, introduce yourself to the patient. He is pleased to see a familiar face and gives permission for you to be informed about his care and to read his medical notes and investigation results.
The patient, a 58-year-old successful businessman, tells you that he flew home from overseas the previous evening and had ‘a few drinks’ to celebrate his arrival. After a sleepless night and drinking more alcohol the next day, he felt tired and jet lagged and lay down to rest. Around 4.30 p.m., he experienced palpitations and felt light-headed. He had no chest pain or discomfort. He had recently bought a smartphone app to check his heart and decided to try it for the first time. This involved placing his fingers on a separate Bluetooth sensor pad and reading the result from the smartphone screen. The app showed his heart rate was about 140 beats per minute (bpm), with a diagnosis of possible AF. He called an ambulance.
In the ambulance
The ambulance officers reported that the patient appeared pale and grey but not diaphoretic. His blood pressure was 150/100mmHg, heart rate 160bpm and irregular, oxygen saturation 98% on room air, and respiratory rate 20 breaths per minute. He was afebrile. He was given oxygen 4L/min by nasal prongs, an intravenous cannula was inserted and 300mg aspirin was administered orally. He had no chest discomfort or pain, no respiratory symptoms and no obvious swelling in his legs or calves. Further examination revealed dehydration with dry mucosa.
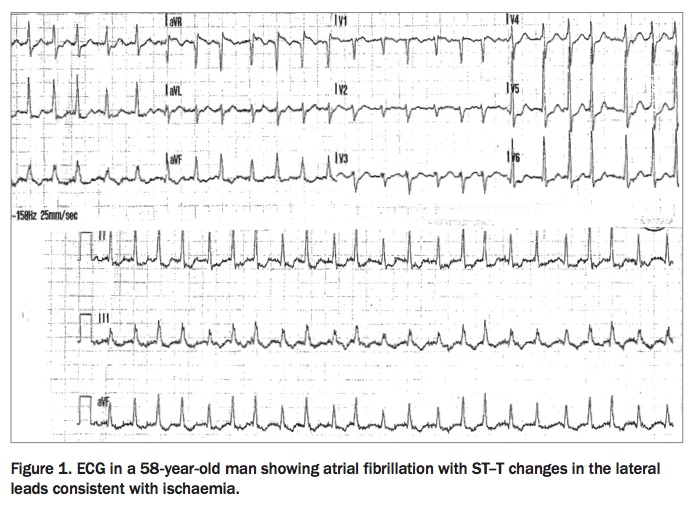
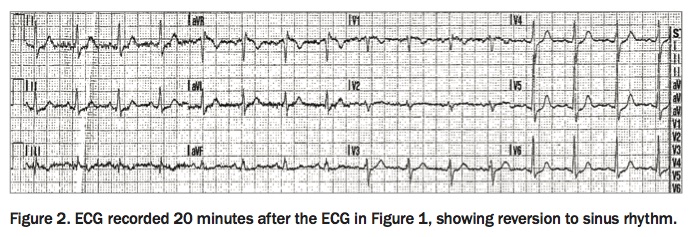
An ECG in the ambulance identified AF with ST–T changes in the lateral leads consistent with ischaemia (Figure 1). Twenty minutes later, a second ECG in the ambulance showed the patient’s heart had reverted to sinus rhythm (Figure 2).
{kind=link}
{kind=link}
In the emergency department
On arrival in the ED, the patient was assessed as urgent, triage category 2. He was taken to a resuscitation cubicle and seen within four minutes. At this time, his blood pressure was 150/105mmHg, his heart rate had dropped to 86 bpm and respiratory rate to 15 breaths per minute. History-taking revealed he had difficult-to-treat hypertension, and the previous night had ‘much more’ to drink than his usual low consumption (one to two alcoholic drinks on weekends). He was a nonsmoker with a significant family history of stroke.
A neurological examination found no abnormalities, and a portable chest x-ray gave normal results. Results of blood tests, including a troponin assay, measurement of glucose and electrolyte levels, full blood count, thyroid function tests and a thrombophilia screen, were also normal. His cholesterol level was high, and his gamma glutamyltransferase level was slightly raised.
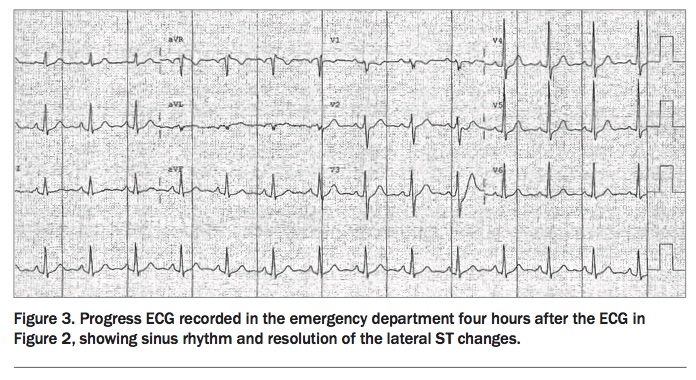
A progress ECG, four hours after the ECG in the ambulance, showed sinus rhythm with resolution of the lateral ST changes (Figure 3).
{kind=link}
Management
The patient was reviewed by the admitting cardiology team that evening and discussed with the cardiologist on call. A diagnosis of alcohol-induced AF (‘holiday heart’) was suspected.
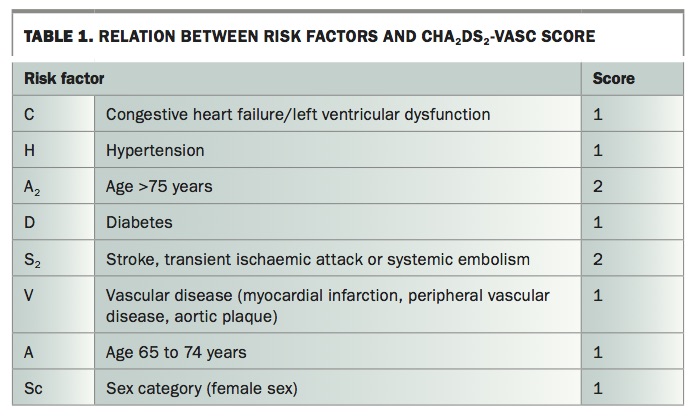
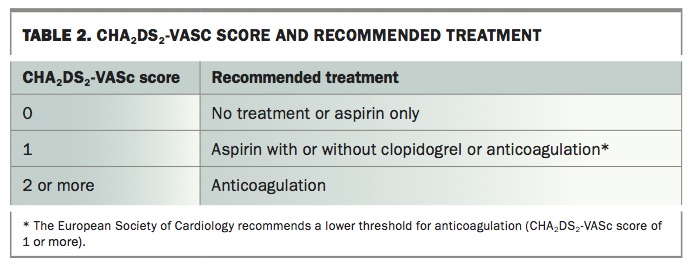
The patient was initially assessed as having a CHA2DS2-VASc score of 1, because of his hypertension, and was started on apixaban 5mg orally (Table 1 and Table 2). He underwent echocardiography, which showed aortic plaque, and his CHA2DS2-VASc score was revised to 2. The cardiology team arranged for him to be transferred to a monitored/telemetry bed for overnight observation.
{kind=link}
{kind=link}
After an uneventful night and review by the cardiologist, he was discharged home with a referral for follow up by the cardiologist within a fortnight.
The outcome
You hear later from your friend that the patient had an uneventful recovery. On two-week follow up, the cardiologist agreed with the diagnosis of alcohol-induced AF. The cardiologist also confirmed that the patient should continue apixaban and hypertension management with lifestyle changes, detailed in a letter to his GP.
You muse that the current recommended basic life support/cardiopulmonary resuscitation protocol does not include taking a pulse. Now that ‘C’ in the mnemonic ABCD refers to chest compression rather than circulation, few people learn how to take a pulse and can detect AF.
Your friend sends you a bottle of wine as a thank you gift.
Discussion
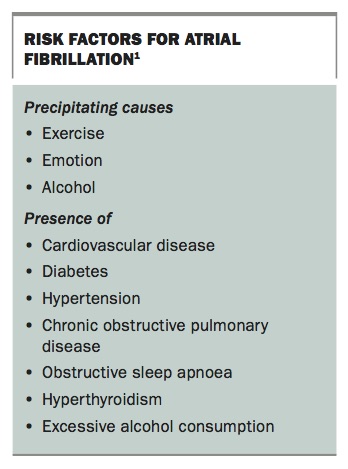
Alcohol consumption is an important risk factor for AF (Box).1 AF following excess alcohol intake, often known as holiday heart syndrome, is a common, well-characterised ED presentation.2 The term ‘holiday heart’ was first used in 1978 in a report of 24 patients hospitalised with AF after a weekend binge.3
{kind=link}
AF occurs in up to 60% of binge drinkers with or without underlying cardiomyopathy.4 Most cases of AF occur during or following weekends or holidays involving increased alcohol intake. Heavy alcohol consumption (e.g. more than three drinks per day), mainly in men, is associated with an increase in AF. However, even modest amounts of alcohol can trigger AF in some patients.4
Alcohol-induced AF usually recovers spontaneously. In the case described above, the patient reverted to sinus rhythm soon after the ambulance was called. Arguably, if he had not checked his heart with the mobile app, prompting him to call the ambulance, the AF might not have been detected and he would not have been started on anticoagulant therapy.
The growing use of mobile apps and other devices that monitor heart rate, such as blood pressure monitors, is likely to increase presentations with suspected AF both to EDs and to GPs. The use of mobile apps has been proposed for AF screening. However, there is controversy over the benefits and harms of these devices, which vary in sensitivity and specificity and are subject to artefacts and false positives.5 Ultimately, the diagnosis of AF requires an ECG.
Nevertheless, the capacity of mobile apps and other patient devices to enable accurate real-time capture of cardiac rhythm, similar to Holter monitoring, may be useful in diagnosing episodic rhythm abnormalities. Many patients who experience episodic dysrhythmias, some with serious symptoms, cannot be diagnosed because clinicians have not been able to capture the dysrhythmia when it occurs. Mobile apps and other patient devices that monitor heart rate may help these patients obtain a diagnosis and appropriate management.