Chronic nausea: investigation and management

Digestive diseases
Assessment of a patient presenting with bothersome nausea requires knowledge of a broad range of possible causes and overlapping disorders. Investigation aims to determine whether hydration and nutrition are adequate and establish a cause so treatment can be targeted. If functional nausea is diagnosed, dietary measures are the mainstay of management. Supportive approaches, psychological therapies and medication may also help, but long-term use of antiemetics is rarely advised.
Remember
- Chronic nausea is an ill-defined subjective sensation of the imminent need to vomit that does not necessarily result in emesis. It is recognised as one of the most frustrating and debilitating functional gut symptoms for patients, largely because of its pervasive nature and a lack of effective therapies.
- Data on its prevalence are limited, but it is a common disorder. Chronic nausea poses a significant diagnostic and therapeutic challenge for clinicians because of its poorly understood pathophysiology, its association with other complex body systems and its overlap with various functional gut disorders.
- Chronic nausea is defined as bothersome nausea (i.e. severe enough to impact on usual activities) occurring at least one day per week for at least three months, with symptom onset six months before diagnosis.1 It may be associated with dry retching or vomiting, but not necessarily.
- The aetiology should be established whenever possible. The most common causes of chronic nausea are functional gut disorders, especially in young patients. In older patients, this symptom should prompt evaluation for organic abnormalities. A thorough medication review is essential.
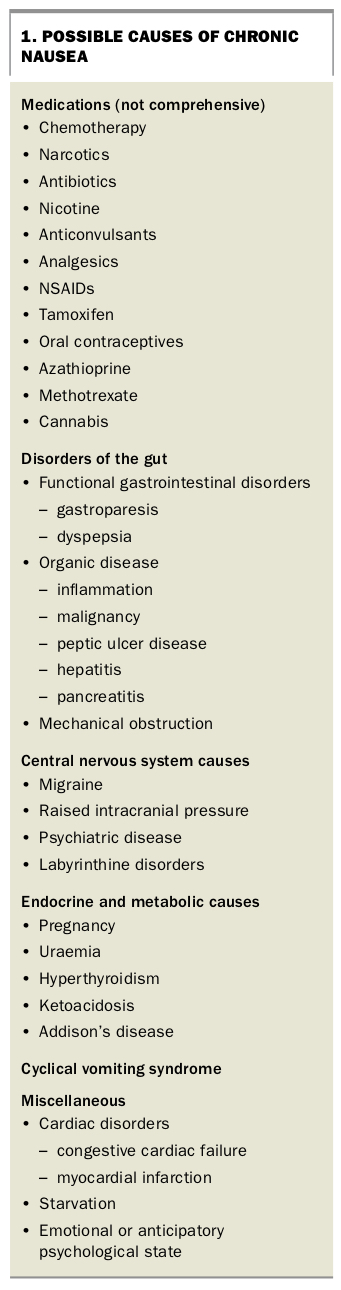
- Distinguishing the cause of chronic nausea is difficult, because the differential diagnoses encompass both pathological and physiological conditions of the gastrointestinal system, central nervous system and endocrine system, and metabolic and psychological disorders (Box 1). Establishing a cause requires thorough history-taking and clinical examination to guide further investigations.
- If functional nausea is diagnosed there is often overlap with other functional gut disorders such as irritable bowel syndrome, functional dyspepsia and chronic constipation. The diagnosis of functional nausea implies a disorder of gut-brain interaction, which is true for all functional gut disorders.2 This interaction is bidirectional and as a result nausea is highly associated with anxiety and depression, irrespective of the premorbid psychological state of the individual.
- Nausea may be the presenting symptom in people with psychological morbidity, especially anxiety and depression. These conditions should be actively asked about and treated individually. Similarly, people with eating disorders may present with chronic nausea and careful screening for these conditions should be considered.
- A careful history regarding the use of cannabis needs to be sought as cannabis use is known to precipitate chronic nausea, especially when it is associated with emesis. Cannabis is generally perceived to improve nausea, but chronic use can certainly contribute to nausea and vomiting. Rome IV has recently included cannabis hyperemesis as a new diagnosis.2
- Patients who have chronic reflux disease or gastritis can present with nausea without other typical symptoms. A gastroscopy is valuable to determine whether these conditions are present. Such patients may be responsive to therapy with proton pump inhibitors.
{kind=link}
Investigation
- Investigation should be tailored to determine a cause and assess for complications of chronic nausea.
Blood tests
- Routine blood tests to screen for endocrine and metabolic conditions are appropriate. Initially, tests for liver function, renal function and thyroid function and measurement of C-reactive protein and fasting glucose levels are suitable, as well as serological testing for coeliac disease. Measurement of beta human chorionic gonadotrophin levels should be performed when indicated. More specialised testing such as a synacthen test and measurement of fasting cortisol and specific drug levels are reserved for appropriate clinical settings.
Imaging
- If emesis is problematic and bowel obstruction seems likely, cross-sectional imaging may be warranted. Initially, an abdominal x-ray should be performed, but a CT scan may also be appropriate depending on the clinical setting.
Endoscopy
- Gastroscopy is often required to diagnose reflux oesophagitis, gastritis, Helicobacter pylori infection, peptic ulcer disease, coeliac disease and subacute gastric outlet obstruction.
Gastric emptying studies
- More detailed studies of gastrointestinal motility such as gastric emptying studies are sometimes used to establish a diagnosis of gastroparesis but should be used cautiously. These tests can be difficult to interpret and may complicate the clinical picture, so are best performed in a specialist setting.
- Up to 75% of patients with chronic nausea will have some delay in gastrointestinal motility, but this does not necessarily mean the aetiology is gastroparesis. Some patients will have normal gastric emptying, and in a few gastric emptying may be rapid.
- The rate of gastric emptying seen with gastric emptying studies rarely correlates directly with symptoms or severity.3 Therapies aimed at improving motility rarely improve features on the diagnostic test, irrespective of clinical improvement, which casts doubt on the usefulness or validity of the gastric emptying test.
Management
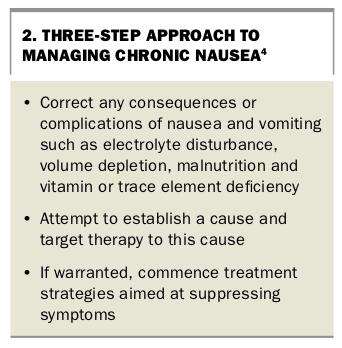
- Immediate management of a patient with nausea and/or vomiting involves correcting any consequences or complications such as electrolyte disturbance, volume depletion, malnutrition and vitamin or trace element deficiency. If a cause can then be established, appropriate therapy may be started with strategies aimed at suppressing symptoms if this is warranted
(Box 2). - The patient should always be assessed for malnutrition and dehydration. These need to be managed appropriately with nutrition support and intravenous fluids when appropriate. Hospital inpatient treatment may be required for severe cases.
- Diet and nutrition are the mainstay of management and referral to an experienced gastrointestinal dietitian is valuable. Diet is primarily designed around adequate nutrition and correction of deficiencies. Generally, a gastroparetic diet is the most effective, with four to five small meals per day that are low fat and low fibre.5 Periods of fasting and bingeing should be avoided. A liquid component may be better tolerated (soup, smoothies etc). There is some evidence that nausea improves on a low-FODMAP (fermentable oligosaccharides, disaccharides, monosaccharides and polyols) diet, but all the evidence for this is from studies among patients with irritable bowel syndrome. Whenever possible, treatment should target an established cause.
- Constipation should be managed with simple laxatives to achieve adequate laxation.
- Anecdotally, acid suppression with proton pump inhibitors can improve nausea for some patients. A four-week therapeutic trial may be worthwhile, although there is little evidence to support this in the absence of gastro-oesophageal reflux disease or gastritis.
- Withdrawal of cannabis is recommended when this is likely to be contributing, especially if nausea is associated with emesis.
- Psychological disorders are commonly associated with chronic nausea. These conditions must be addressed, and referral to a psychologist or psychiatrist is recommended. Antidepressant therapy is often beneficial. Patients with suspected eating disorders should be referred to appropriate clinicians and support services.
- If functional nausea has been diagnosed, reassurance and education are crucial to improving symptoms. Giving the patient a clear explanation about the role of the gut-brain axis and the role of stress, anxiety and depression in symptom generation and escalation is invaluable.
{kind=link}
Medical therapy
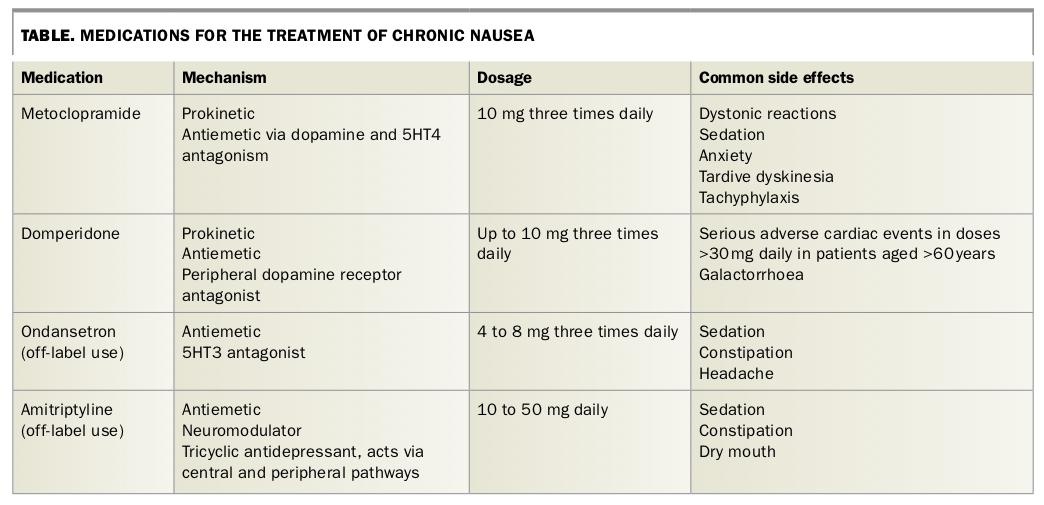
- Medical therapy is broadly characterised into three groups (Table):
{kind=link}
— antiemetics (act centrally)
— prokinetics (improve gastrointestinal motility and motor function)
— neuromodulators (reduce gastric hypersensitivity).
- Medications used for acute nausea and vomiting, such as metoclopramide and domperidone, may have limited efficacy in chronic nausea owing to their side effects and tachyphylaxis. Care must be taken to avoid the accumulation of unhelpful medications; polypharmacy may contribute to ongoing symptom generation.
- Use of prochlorperazine is limited by its side effects, especially sedation and extrapyramidal reactions, and there is little evidence to support its effectiveness in chronic nausea.
- Low-dose erythromycin is sometimes used to promote motility in the setting of chronic nausea, particularly in the presence of gastroparesis. Use is off label and often hampered by side effects, particularly gastrointestinal side effects.
- Cisapride is thought to have some prokinetic activity, but it has serious side effects, most notably prolongation of the QTc interval. It is TGA approved for gastroparesis, but it is thought its efficacy has been overestimated in the past and the benefit is overshadowed by serious toxicity risks. For this reason, its use is limited, especially in general practice.
- 5HT3 antagonists such as ondansetron may have an additional antinociceptive effect via mediation of visceral hypersensitivity. This would make them an attractive option for treating functional nausea; however, there is little evidence to support their use, side effects need to be monitored (e.g. constipation) and nausea is an off-label indication, which could make these agents prohibitively expensive.
Antidepressants
- There is evidence for the off-label use of low-dose tricyclic antidepressants in the treatment of chronic nausea.6 Starting a patient on a low dose and titrating to the maximum tolerated dose is useful but is often hampered by side effects, especially somnolence. Low-dose tricyclic antidepressants are given with the aim of reducing visceral and central sensitisation, rather than treating anxiety or depression per se. If these conditions are present, effective management is necessary either with psychological support or antidepressant medication most suited to the individual presentation.
- There is little evidence on the use of newer antidepressants such as selective serotonin reuptake inhibitors in chronic nausea. From a mechanistic perspective, mirtazepine may be an attractive option because of its effect on improving gastric motility, improving appetite and weight gain. More studies are required to establish its role.
Psychological therapies
- Psychological approaches such as cognitive behavioural therapy or gut-directed hypnotherapy are increasingly recognised as effective strategies for managing irritable bowel syndrome even in the absence of coexistent psychological comorbidity. There is some evidence that hypnotherapy can reduce nausea in these patients and that the response is sustained.7 It should be considered for patients with chronic nausea.
Alternative therapies
- Many patients turn to alternative therapies given the lack of efficacy of conventional antinausea medications. Alternative therapies such as ginger, herbal remedies such as STW5 and acupuncture may provide symptomatic relief but are not well studied.
Conclusion
Management of chronic nausea can pose a dilemma for doctors because of the complex pathophysiology of the condition. Investigation and treatment should be focused on establishing a cause and directing therapy when appropriate, ensuring adequate nutrition and reducing symptoms. Failure of conventional antinausea medication in patients with chronic nausea should prompt the physician to think more along a functional paradigm and include dietary therapies, supportive approaches and psychological therapies to improve symptoms. MT