Vulval lichen sclerosus – diagnosis and treatment

Women's health
Vulval lichen sclerosus (VLS) is an important condition that occurs in women of all ages, although it is most common in those over 50 years. Significant scarring and deformity and malignant squamous neoplasia of the vulva are serious complications of untreated VLS that can potentially be prevented by early treatment with topical corticosteroids. Proactive management can modify the long-term course of the disease.
- Vulval lichen sclerosus (VLS) can occur at any age and is uncommon but becomes more prevalent in women over 50 years. It is probably underdiagnosed.
- If treated inadequately it can lead to scarring and permanent deformity of the vulva.
- Long-term maintenance treatment with topical corticosteroids is a safe option that can keep VLS in remission and potentially reduce the risk of malignancy.
- Patients with VLS require long-term follow up even after initial remission is achieved, with a physician who is adequately experienced in managing this condition, as it may continue to silently progress or reappear without causing symptoms.
- VLS is unrelated to sexually transmitted infections. Lichen sclerosus is a skin disease and is not infectious.
Lichen sclerosus (LS) is an uncommon and potentially serious skin disease that has a predilection for the genital skin and is much more often encountered in females than males. The prevalence in the whole population is unknown because of underdiagnosis and referral bias and it may be underestimated. Vulval LS (VLS) occurs in all age groups, including children. The mean age of onset is in the mid to late 50s with about one-third of cases occurring in women under 50 years. Paediatric disease accounts for 7 to 15% of all cases. It was believed that prepubertal VLS resolved at puberty, but recent evidence has shown that this is not consistently true.
VLS is an important condition to diagnose correctly and manage actively for two reasons. First, if not treated aggressively it may significantly scar, shrink and deform the vulva and cause stenosis of the introitus with a resultant impact on quality of life. Second, it is a risk factor for malignant squamous cell neoplasia of the vulva with a lifetime risk in untreated or inadequately treated disease of 2 to 6%.1,2 However, recent research suggests that both outcomes can be prevented by early intervention, and even with later intervention cancer and further scarring can be arrested;3 therefore, patients with VLS require lifelong observation and encouragement to continue treatment. This fact has been underinvestigated and is lacking in much of the existing literature on the subject.
Aetiology
The true aetiology of LS remains unknown. Studies have shown high rates of autoimmune disease in patients with LS and even higher rates of detection of autoanti-bodies, but this does not confirm that LS itself is an autoimmune disease. The two diseases seen most often in association with LS are autoimmune thyroid disease and vitiligo. It is not uncommon to find positive low-titre antinuclear antibody levels in patients with LS, but this is rarely significant enough to warrant further investigation. If thyroid autoantibodies are present further investigation is warranted. Even in the presence of thyroid autoantibodies thyroid function is often normal.
Morphoea, alopecia areata and pernicious anaemia have been linked to LS. More recently, LS has been found to have a higher incidence in patients with Turner syndrome. LS can run in families although it more commonly occurs by chance.
Clinical presentation of VLS in adults
Symptoms
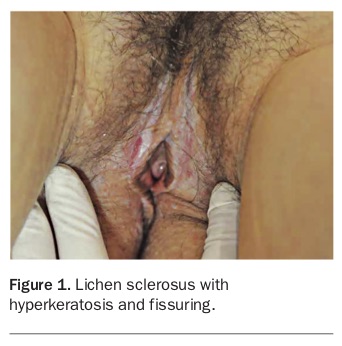
Symptomatic VLS can have a significant impact on quality of life and sexual functioning. The most common presenting symptom of VLS is vulval itch, which is often severe, disrupting life and sleep. There is sometimes pain as a result of excoriation or fissuring. Distressing clitoral hyperaesthesia may occur, and dyspareunia is very common. Other symptoms include dysuria, difficulty voiding, sexual dysfunction and bleeding from skin fissures of the vulva and perianal skin (Figure 1).
{kind=link}
Occasionally VLS can be completely asymptomatic, discovered by chance by the patient or by the GP during a cervical screening test. This is rare but important because the disease may be advanced at presentation as a result. This situation can be dangerous, as asymptomatic disease may not be noticed by the patient until carcinoma arises.
Appearance
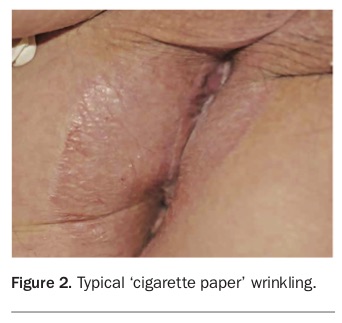
The appearance of a well-defined white sclerotic plaque with an atrophic wrinkled surface is typical of LS (Figure 2); however, there are many variations. These include:
{kind=link}
- multiple white papules or macules producing a speckled appearance
- thickened hyperkeratotic plaques
- plaques limited to small areas such as the tips of the labia minora or the clitoris or clitoral hood
- oedema on a background of pallor
- telangiectasia, purpura and/or haemorrhagic blistering on a background of pallor
- angiokeratomas on a background of pallor
- fissures and traumatic ulcers
- erosions
- blisters
- LS associated with vulval psoriasis, which appears erythematous
- brown hyperpigmentation similar to postinflammatory hyperpigmentation, which can supervene.
Distribution
The distribution of VLS is variable. The classic textbook description is of a figure of eight encircling the vulva, perineum and perianal skin; however, it can affect only the perianal region, clitoris, the internal surfaces of the labia majora and labia minora, and the vaginal introitus. VLS very rarely involves the vagina proper superior to the hymen. If the vagina is involved, VLS may coexist with another condition such as lichen planus or chronic vulvovaginal candidiasis, both of which affect the vagina.
Anatomical abnormality
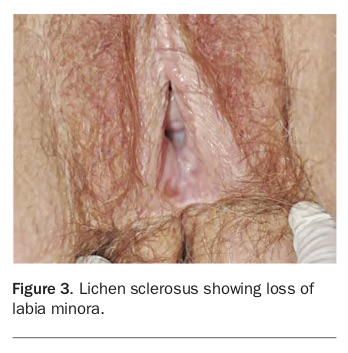
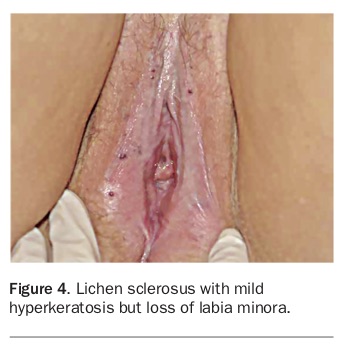
A key point in recognising VLS, particularly in the late stage, is that the vulval shape is often not normal. While it is true that the size of the labia minora is highly variable, almost all women develop them. If they are completely missing (with the absence of sebaceous glands and presence of visible lines of resorption) or if the clitoris appears shrunken or buried under scar tissue this is very suggestive of VLS (Figure 3 and Figure 4). The only other conditions that can result in this appearance are lichen planus, graft-versus-host disease and the very rare mucous membrane pemphigoid, all of which are erosive conditions. In some cases VLS and lichen planus can occur concurrently in an overlap condition with VLS of the vulval skin and lichen planus involving the vestibule and vagina.
{kind=link}
{kind=link}
VLS obeys the Koebner phenomenon, and therefore localises into areas of friction and trauma. This possibly explains why it is usually most recalcitrant on the perineum and the inner surfaces of the labia minora. It also raises a question regarding the role of urinary incontinence, particularly in the setting of treatment resistance.
The course of VLS in adults
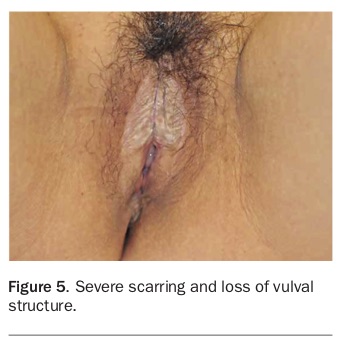
The course of VLS is unpredictable. If left untreated, about one-half of patients lose structure of the vulva, with the labia minora eventually becoming reabsorbed and the clitoris becoming entrapped and buried, revealing an overall atrophic, shiny, white vulva that is missing normal anatomy. The timeframe over which this happens is, anecdotally, a few years but has never been accurately estimated. It is very typical for the labia minora to fuse, with the labia majora laterally and with each other subclitorally. The fusion line is brittle and easily tears during intercourse. Perineal fissuring and tearing is also common. Eventually the vaginal opening may become significantly stenosed, with pooling of urine within the vagina simulating urinary incontinence. Once scarring has occurred it is irreversible, although fusion between the clitoris and clitoral hood can reverse with treatment. In advanced disease gross distortion of vulval anatomy may occur (Figure 5). There have not been any studies to determine which patients are prone to scarring.
{kind=link}
Among untreated or inadequately treated patients with VLS, 2 to 6% will progress to malignancy; however, which patients are prone to this is not predictable and it is therefore necessary to regard all as being at risk. Progression to carcinoma has not been reported in children although there have been several case reports of vulval melanoma in association with paediatric VLS. Early-onset squamous malignancy has been reported in adults in whom VLS first appeared in childhood.
In the past there has been controversy regarding the possibility that the course of the disease could be modified by treatment, and this led to a nihilistic approach that addressed only symptoms and not signs. This approach is still evident in the latest guidelines from Europe and the UK.4,5 However, a recent study showed that ongoing topical corticosteroid (TCS) maintenance treatment that is matched to the severity of the disease so that it is suppressed will prevent both scarring and carcinoma.3
Little is known of the course of the disease in pregnancy. Recent data suggest that it is unchanged and that treatment should be continued during pregnancy without adjustment from nonpregnant treatment. TCS use is considered safe in pregnancy. Patients with LS can usually have a normal vaginal delivery.6
Histopathology
The definitive diagnostic test for LS is a skin biopsy, which should be taken from the most densely white area. The histopathological characteristics are distinctive and uniform across all ages. The epidermis is often atrophic with hydropic degeneration of basal cells and a homogeneous pale zone of hyalinisation in the upper dermis. In the dermis there is a variable lichenoid infiltrate of mononuclear cells.
Although VLS has a characteristic clinical appearance, a skin biopsy taken from the affected site at first presentation provides diagnostic confirmation and exclusion of alternative diagnoses. A positive biopsy result is also helpful in counselling the patient about the important long-term consequences and the need for follow up, and useful if the patient changes location or medical practitioner. The vulval skin in treated disease may appear normal and some experts have called for biopsy before treatment whenever possible so that there is a clear, histopathological record of the diagnosis. In children, a clinical diagnosis is almost always sufficient because biopsy is traumatic, the list of possible differential diagnoses is small and neoplastic transformation has never been reported to occur in children with VLS.
Clinical presentation of VLS in children
The average age of presentation of children with VLS is about 5 years and studies indicate that many children are affected for long periods before being diagnosed and treated. The most common presenting symptoms are vulval itch and soreness. Other symptoms or noted signs at presentation are purpura, bleeding, dysuria, constipation, genital erosions and extragenital lesions. Night waking and night terrors are common. Like adults, children can uncommonly be asymptomatic. Although children present with itch and pain, about two-thirds also report dysuria and pain with defaecation leading to constipation. This is quite different to adults, who normally present with itch and dyspareunia. It is not uncommon for children with VLS to be referred to urologists and enterologists.
Some children with VLS have reportedly been referred to child protection units when purpura has been present. However, in VLS purpura may occur without significant trauma. When purpura is caused by physical damage in normal vulval skin it resolves quickly, unlike the purpura of LS, which is persistent.
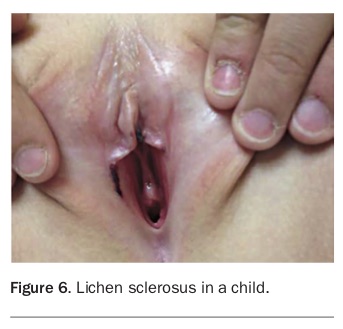
The morphology of VLS in children does not differ from that in adults. Older texts again describe a ‘figure of eight’ appearance encircling the vulva and perianal skin, but any part of the vulva, perineum and perianal skin may be affected individually (Figure 6). Scarring also occurs in children, and in rare circumstances a child will present with loss of architecture without the typical epithelial changes. Fissuring is common and is responsible for pain.
{kind=link}
The course of VLS in children
As in adults, if VLS is not treated in a child progressive loss of the vulval architecture occurs. The child may not ever develop labia minora and the clitoris may be buried. The clitoral hood may become nonretractile.
Older reports have suggested that LS in children will resolve at or after puberty. This is not always the case and recent studies show that although there may be improvement, true remission cannot be assumed.7
As in adults the course of the disease can be modified by treatment. A confounding problem in VLS is the adolescent years. During this time, in my experience, compliance issues often arise linked to embarrassment and refusal to be examined or aided by a parent. Even the most trusting doctor-patient relationship may flounder at this time.
Further, compliance can be a problem in managing children when parents are unwilling or unable to supervise. When treatment is left entirely to small children it is understandable that it may be sub-optimally applied.
Differential diagnosis
The differential diagnosis in adults includes lichenification most often associated with dermatitis in atopic individuals, extramammary Paget’s disease, genital warts, vitiligo, nonpigmented seborrhoeic keratosis and vulval intra-epithelial neoplasia. Although lichen planus may be characterised by white striations known as Wickham’s striae, it is not usually densely white; however, the scarring associated with it may simulate end-stage VLS. Graft-versus-host disease and mucosal pemphigoid have more in common clinically with lichen planus than VLS but are also scarring conditions. Additionally, VLS may coexist with lichen planus, producing a confusing clinical picture.
When psoriasis coexists with VLS the clinical picture is also confusing as the skin may not appear white and the clue is the textural change, which may be subtle. Similarly, when it coexists with vitiligo textural change and loss of architecture will help to differentiate the two conditions clinically. Vitiligo lacks the epithelial changes seen in LS, presenting with sharply marginated white macules that fluoresce under ultraviolet light. If there is any doubt, a vulval biopsy can be done to confirm the diagnosis.
In peri- and postmenopausal women atrophic changes often coexist with VLS and add a degree of confusion. There may be a reduction in the size of the labia minora and pallor of the vestibule due to oestrogen deficiency, which can simulate VLS.
It is important to differentiate the recently described condition vestibular sclerosus from VLS. Vestibular sclerosus involves only the vestibule and does not have histological features of LS. There is still some controversy as to whether this condition is a subset of VLS; however, it is not sensitive to corticosteroid treatment.
In children, VLS has a characteristic clinical appearance and there is little to consider in the differential diagnosis. Although lichenified atopic dermatitis can simulate VLS in adults it is much less likely to do so in children. Vulval intra-epithelial neoplasia, which may have the appearance of a white plaque, has not been reported in prepubertal children. Vitiligo in children is usually not difficult to differentiate owing to a lack of epidermal changes.
Malignancy associated with VLS
The appearance of a vulval squamous cell carcinoma can include nodules, persistent fissures, hyperkeratotic plaques, nonhealing ulcers and fungating tumours. Any change in an area of LS that does not promptly resolve with potent TCS treatment must be biopsied.
The association of VLS with genital malignancy has very important implications for management. Patients must be aware of the risk, be educated about what to look for and be regularly treated and followed up.
Anecdotally, experts have long suspected that adequately treated VLS might have a malignancy rate much lower than the usual 4 to 6%. The suggestion has therefore been made that the risk of malignancy is reduced in uncomplicated VLS that has been diagnosed and treated appropriately. A prospective study of VLS in 507 adult women compared patients who adhered to treatment and those who did not. It demonstrated that TCS treatment that kept the skin objectively normal also resulted in minimal scarring and greatly reduced the risk of cancer.3
The effect of VLS on quality of life and sexual activity
VLS has a major impact on quality of life that is not always improved simply by treating the skin disease. Returning the skin to normal in VLS does not always ensure that the impact on the patient has been reduced. Although pain and itch may have resolved, patients often have ongoing issues: the need for maintenance treatment and regular examinations can, in itself, be a burden, particularly for children and their families. Concerns about the future, particularly relationships, pregnancy and cancer, can have significant emotional effects.
In my experience, patients with VLS can usually resume sexual activity with treatment. In postmenopausal women this is complicated by changes related to genitourinary syndrome of menopause. Patients with significant scarring may not be able to resume normal sexual activity until the scarring has been corrected surgically. Women with a long history of painful sex may have significant pelvic floor overactivity and physiotherapy may be needed to overcome this. Some develop an aversion to sexual intercourse and need psychological help, and some decline any help because their lack of interest in sex has been legitimised by their disease. In general, it should be possible to return almost all motivated patients to a normal sex life as long as a treatment regimen can be found that they find acceptable and easy to comply with.
Management
VLS in adults is a lifelong disease that can be suppressed with treatment; however, most patients are unable to stop treatment without eventual relapse, although this may take many months. It is important when counselling to emphasise that treatment should be assumed to be for life.
In unusual instances when the condition appears to have remitted without further treatment patients either need to be kept under long-term observation or told to report any change as, in my experience, VLS can reactivate after years of dormancy.
Before a decision about treatment is made it is important to decide on the severity of VLS. As yet, there is no universally accepted severity grade. Two studies have suggested using hyperkeratosis grade as a guide to choosing topical therapy.3,8
After a response to therapy, function usually returns and the impact on life is reduced. Although minor structural change may partially reverse, scarring is not affected by medical treatment and surgical management is usually required if there is functional impairment. In my experience not all scarring results in loss of function, particularly if the patient is not sexually active.
Topical therapy
There are two phases of treatment for VLS:
- induction of remission, carried out over a period of up to a year
- maintenance treatment, which is lifelong.
The first study using a superpotent TCS to treat VLS was published in 1991 and it is now accepted that treatment with a potent TCS is the gold standard for obtaining remission in VLS. Many studies of potent and superpotent TCS treatments have confirmed they are safe and highly effective in children and adults.
VLS is so responsive to TCS that failure to improve should be reason to suspect that the diagnosis is wrong, the patient is not using the treatment or there are other factors confounding symptomatic response, such as malignancy, allergy, superinfection or oestrogen deficiency. In rare cases of severe hyperkeratotic disease, however, potent TCS alone can be inadequate to achieve complete control.
Initially, most published data on TCS therapy in VLS were for clobetasol propionate, a product that is not commercially available in Australia. More recent studies compared its efficacy with that of mometasone furoate 0.1%. However, it should not be assumed that VLS can only be treated by these two products; in almost all cases other TCS of similar potency will produce good outcomes. The clinician should first decide if the lesions are more or less hyperkeratotic and match the potency of the TCS to the severity of the skin disease. There is no one preparation that is superior to the other. The relative severity and choice of treatment appropriate to it is what is relevant to management. In general terms, medications in ointment bases rather than creams tend to be better tolerated and more effective on the vulva.
Therefore, in my opinion, the main focus of treatment should not be on the product used but the end result: attaining and maintaining normal or near-normal skin. There is no single way to do this and clinicians can make their own judgement relative to the severity of the patient’s disease and their preference for daily or intermittent treatment. Many patients relate that daily regimens are easier to recall than intermittent ones. Regular follow up encourages ongoing compliance.
Induction of remission
Regimens to induce remission vary but the common theme is that a potent or superpotent TCS should be used initially. There is no single way to induce remission and therapy should be guided by individual response.
A recent Australian study recommended the following treatment regimens based on hyperkeratosis grade.3
- Severely hyperkeratotic disease (very thick, white plaque): ultrapotent TCS (compounded clobetasol propionate 0.05% ointment) twice daily until itching has ceased (usually one to two weeks) then daily until review at six weeks. Be aware that some pharmacists may mistakenly dispense ‘clobetasone’ ointment instead of ‘clobetasol’. Clobetasone is not compounded and is a weak TCS.
- Hyperkeratotic disease (moderately thick white plaque): superpotent TCS (e.g. betamethasone dipropionate 0.05% ointment or optimised vehicle, or mometasone furoate 0.1%) twice daily until itching has ceased then daily until review at six weeks.
- Mild disease with only pallor and very little hyperkeratosis: moderate-potency TCS (e.g. triamcinolone acetonide 0.02%, methylprednisolone aceponate 0.1%) daily until review at six weeks.
When a potent TCS is used on the vulva it is important to review the patient at about six weeks of treatment to assess effect and tolerability. Patients are usually feeling much better and many assume they are cured. They may not have understood initially how important ongoing treatment is, so this visit is an opportunity to emphasise that treatment must now be maintained even if there are no symptoms and to explain that the reason for this is to prevent cancer and scarring.
The initial potency of TCS is continued until the skin texture and colour have returned to normal or as close to normal as possible. There may be residual hyper- or hypopigmentation; however, the texture of the surface of the skin usually improves markedly. Once this has been achieved patients progress to maintenance therapy. Symptom resolution occurs quickly but resolution of abnormal signs takes longer. Patients must therefore continue their regular treatment even after symptom resolution.
Long-term management
Although the correct diagnosis and initial management of VLS is of great importance, treatment does not stop there and it is long-term control that ensures the safety of the patient.
Regimens for maintenance treatment are difficult to research due to the challenges of conducting a long-term follow-up study. Typically, reviews and published articles state that the condition does not spontaneously resolve and has to be controlled; however, there is no international consensus on what long-term control involves.
The time taken to achieve remission of VLS is variable but in my experience is usually about three to six months of continual potent TCS treatment. The weakness of most published studies is that they observe patients for the first three to six months only. Long-term observational studies of adequate numbers of treated patients are few; the longest period of observation documented is three years.
The Australian study of 507 women is the best evidence we have to confirm what most experienced practitioners know: that although use of TCS easily induces remission, it does not cure VLS.3 Furthermore, a large French study reported an 84% recurrence rate if treatment was ceased.9
These studies suggest that treatment might change the course of the disease, reducing the risk of cancer and scarring, and the Australian observational study has now provided compelling evidence that this is the case. In this study patients were reviewed every three to six months and potency of the TCS was slowly titrated down to a moderate-to-mild potency for maintenance therapy. This was achievable in about 75% of patients. The other 25% required long-term therapy with a more potent TCS.3
The main problems that have been postulated with long-term use of TCS treatment on the genital area are TCS-related atrophy, periorificial dermatitis and Candida superinfection. In practice only periorificial dermatitis is common and it is frequently asymptomatic as long as the dose of TCS is titrated to the severity of the condition. Despite this, patients are often quite fearful of long-term TCS treatment and need substantial reassurance to continue to comply, particularly if they are given conflicting information by a pharmacist who may not understand the diagnosis and the need for long-term treatment. The argument that long-term TCS treatment will produce atrophy is not valid in VLS. TCS applied to normal skin over long periods of time might induce atrophy, but this does not occur when an active inflammatory disease such as VLS is being treated. Other authors have confirmed this observation.10
Patients often ask what the best time of day is to apply the TCS. Since an important aspect of treatment is to establish a regular routine, the best answer is to apply the treatment at a time that they can regularly comply with. For some this is before bed and for others it is after showering. Patients often say they get into bed having forgotten their treatment and are then too tired to get up. They should be encouraged to decide what works best for them.
In practice, a treatment review every six months will determine the lowest TCS potency and maintenance regimen that will ensure continuing remission. TCS treatment is constantly titrated to the degree of hyperkeratosis (Figure 1 and Figure 4). If hyperkeratosis severity increases, the strength of treatment is increased. If corticosteroid dermatitis occurs treatment strength is reduced. Managing patients with VLS long-term with TCS has been shown to be safe, inexpensive and effective.3,11
None of the compliant patients in the Australian study developed cancer and more than 95% had no further disease progression or scarring. More than 90% had complete and sustained symptom control, and of those who were sexually active more than 90% no longer experienced dyspareunia. For most, complying with treatment was not difficult.
In light of this study, regimens that are used on an ‘as-needed’ basis to control symptoms only may need to be re-evaluated. Symptom control in VLS is not difficult to achieve, but objective disease suppression should be the target outcome, or the patient is still at risk of complications. It is common that patients who develop cancer or disease progression as a result of poor treatment compliance remain asymptomatic.
A recent retrospective study of 46 children with VLS, comparing compliant patients with noncompliant, showed that when normal skin was attained and maintained progression of the disease ceased and scarring and atrophy did not occur. Scarring that was present before treatment, however, did not reverse.12
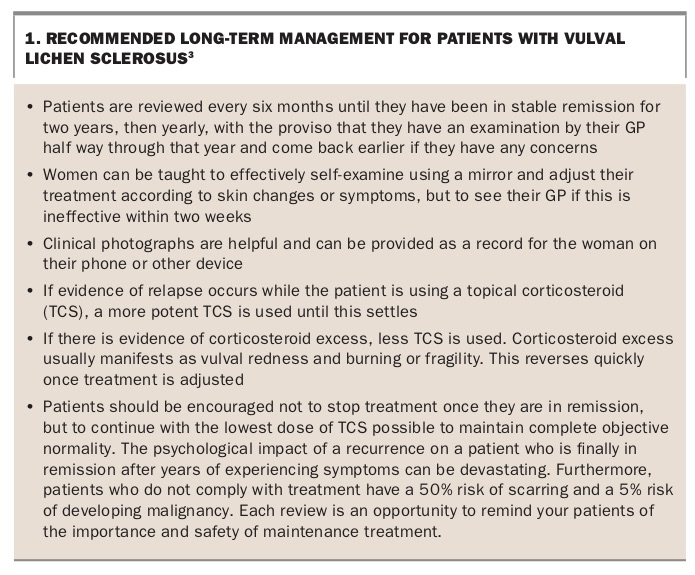
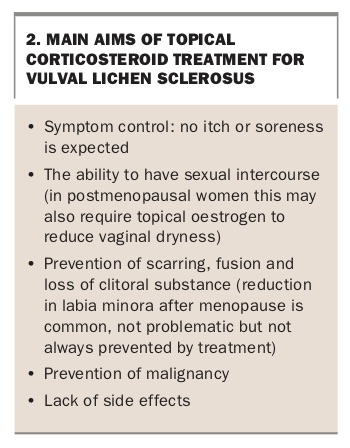
An approach to long-term management of patients with VLS is shown in Box 1.3 The aims of treatment are symptom control, enabling sexual intercourse, preventing scarring and anatomical changes, preventing malignancy and avoiding side effects of TCS use (Box 2).
{kind=link}
{kind=link}
Other topical therapies
Topical immunosuppressive agents, such as tacrolimus and pimecrolimus, have been described as potentially playing a role in the treatment of VLS in children and adults. Those who recommend them state that they are less likely to cause atrophy; however, atrophy is very rare from properly titrated TCS, and when it occurs it invariably improves with a lower potency product.
The theoretical disadvantage of topical immunosuppressive agents is an increased risk of malignant transformation due to local immunosuppression. This is arguably an important consideration given the well-described association of VLS and malignancy. Squamous cell carcinoma has been reported in adults with VLS in association with pimecrolimus treatment.
At the time of writing, there are insufficient data to recommend topical immunosuppressive agents to treat LS, and no justification for their use because TCS treatment is effective and safe. Topical immunosuppressive agents have no advantage over TCS. They are more expensive, very likely to sting and burn and their long-term safety has not been established.
Historically, topical testosterone has been used to treat VLS. However, there is no longer any role for it, as it is ineffective and may produce androgenisation in girls.
Similarly, topical oestrogen is of no value in treating VLS per se, other than to reduce hypo-oestrogenic atrophy in postmenopausal women. However, ongoing pain from vaginal dryness and fragility, which are part of the genitourinary syndrome of menopause, may make it difficult to assess outcomes of treatment for concurrent VLS and should therefore be addressed concurrently.
Many patients who are being treated with TCS also benefit from the use of a moisturiser during the day. There is no one product that is superior to others and patients should use a product that does not sting or feel greasy.
Physical therapy: surgery, laser, stem cells and lipoinjection
Historically, vulvectomy has been performed in adults for VLS, but the disease recurs despite this. This is no longer considered an acceptable method of treatment and is completely contraindicated.
Various surgical procedures have been used to treat labial and periclitoral adhesions. Simple division of adhesions gives a very satisfactory result, provided that potent TCS are used daily after the operation until healing is complete. Unless this is done, refusion is likely. It is sometimes necessary to apply the postoperative steroid on a dilator. Surgery is rarely appropriate therapy in the paediatric population unless significant fusion of the labia has occurred.
Newer treatments for very recalcitrant hyperkeratotic VLS include intralesional platelet-rich plasma, which has been termed ‘stem-cell treatment’ in the lay press, and lipoinjection. Unfortunately, these as yet unproven and very expensive treatments have attracted attention in the media and some patients see them as a potential cure that is naturally more attractive than a lifetime of maintenance treatment. Convincing clinical trials are lacking.
In some patients with hyperkeratotic disease ablative carbon dioxide laser treatment can be a useful adjunct to treatment but is not a substitute for topical therapy, which must be continued subsequently to maintain clinical response. There is no role at all for vaginal rejuvenation laser therapy in VLS.
Conclusion
Although the aetiology of VLS remains unknown, knowledge of how to manage it has progressed in the past five years. Once thought to be a difficult-to-manage condition with a poor prognosis, it is now known that the course of the disease can be modified by treatment that is safe and effective in the long term. With regular TCS treatment patients can remain symptom free and clinically stable, returning to a state of normal wellbeing for long periods. MT
References
Further reading
J Reprod Med 2007; 52: 329-331.