Travellers’ diarrhoea: a guide for GPs

Travellers’ diarrhoea is one of the most common problems faced by travellers. Although most travellers present to their GP primarily for relevant travel vaccinations and/or malaria prophylaxis, it is important to spend time discussing both the risk of acquiring travellers’ diarrhoea and self-treatment strategies.
Correction
A correction for this article will be published in the July 2019 issue of Medicine Today. The online version and the full text PDF of this article (see link above) have been corrected.
Travellers’ diarrhoea (TD) is widely acknowledged as one of the most common diseases occurring in travellers with 30 to 70% affected either when away and/or on their return.1-3 Although the disease may be mild, progression to moderate or severe disease can occur, which can be incapacitating. Diarrhoeal disease remains a relevant cause of death in young children in developing countries; however, mortality from TD is extremely unlikely.4
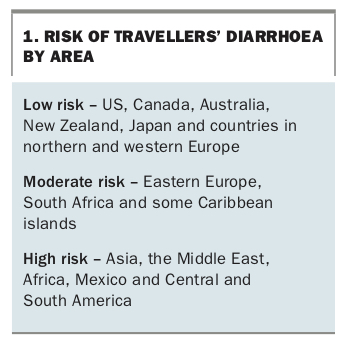
The risk of acquiring TD is generally higher in developing countries, but also in any destination or establishment without carefully managed food and water safety precautions (Box 1). Risk is also higher in travellers with lowered immunity from any cause, as well as in some individuals who are just prone to symptoms.
{kind=link}
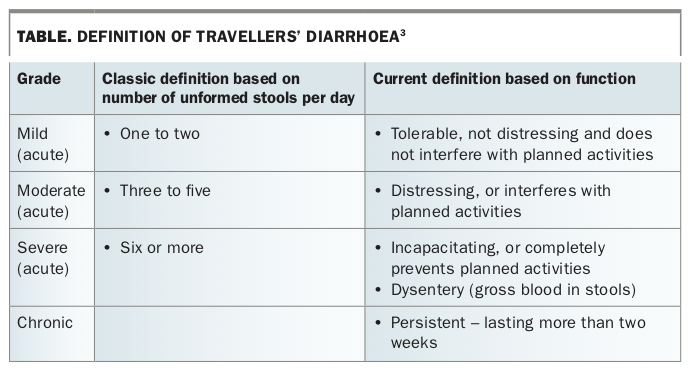
Until recently, the generally accepted or ‘classic’ definition of TD found in any textbook on infectious diseases or in published articles has been based on the number of unformed bowel motions per day. However, in 2017, the International Society of Travel Medicine released new guidelines based on the evidence- based GRADE system (Grading of Recommendations Assessment, Development and Evaluation).3 This has redefined TD based on function – that is, the degree to which a person is affected and whether this interferes with planned activities – and TD is now graded as mild, moderate, severe or chronic (Table). Dysentery is graded as ‘severe’ and redefined as blood in the stool (not associated with haemorrhoids); chronic diarrhoea is redefined as ‘persistent’ if lasting for more than two weeks.3 This approach is more appropriate for travellers in that it recognises individual variation in tolerance of symptoms and rationalises treatment options.
{kind=link}
Aetiology
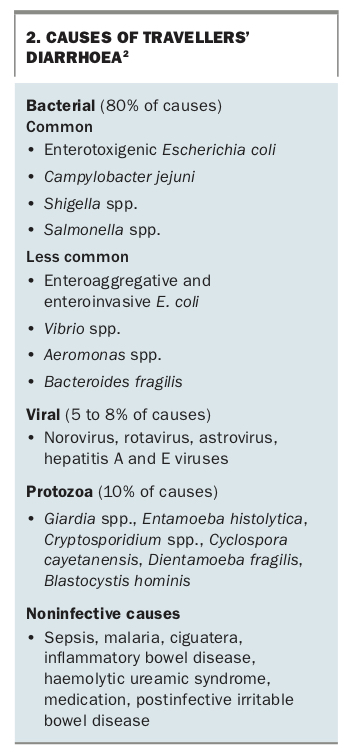
The causes of TD have been studied for decades, with a consistent 80% of causes known to be bacteria, 5 to 8% viruses and 10% protozoa, with the latter being a more likely cause in persistent TD (Box 2).2
{kind=link}
The role of organisms such as Blastocystis hominis, Dientamoeba fragilis and Cryptosporidium spp. is unclear as they are generally regarded as commensals by most microbiologists unless symptoms occur, in which case treatment is recommended.
Postinfectious irritable bowel syndrome or functional bowel disease can occur following TD with no underlying gastrointestinal disease and negative microbiological aetiology.3 If no infectious cause is found but blood tests are abnormal and/or symptoms are persistent, it is important to consider excluding serious diseases such as inflammatory bowel disease, diverticular disease and bowel cancer. These conditions require referral for endoscopic investigation.
Prevention
Food and water precautions
The WHO has produced the ‘Five keys to safer food’ strategy, which is based on the following principles:
1. Keep clean
2. Separate raw and cooked
3. Cook thoroughly
4. Keep food at safe temperatures
5. Use safe water and raw materials.5
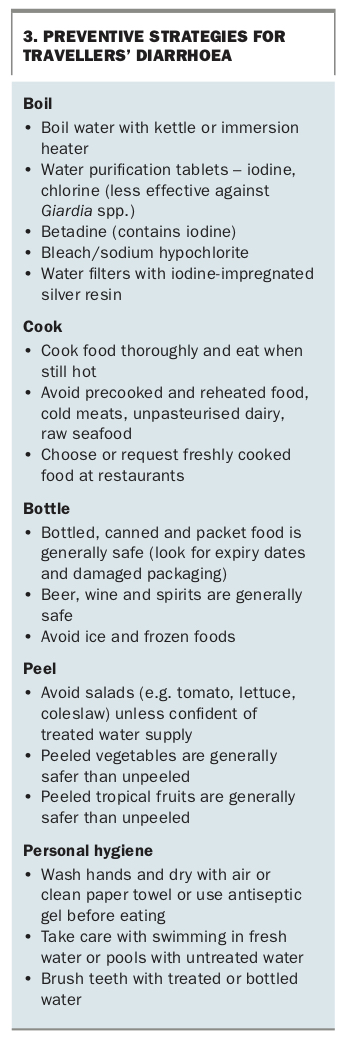
A more detailed explanation of the five key areas is available from the WHO website; however, prevention is primarily based on common sense food and water precautions with the mantra ‘boil, cook, bottle or peel’ and ensuring that hands are clean before eating and during food preparation (Box 3). In practice this is difficult advice to follow, especially in higher risk countries. In the real world, most travellers are not able to or simply do not follow this advice.
{kind=link}
Vaccines
There are several vaccines, such as those against hepatitis A, typhoid and polio viruses and rotavirus (children only), that are routinely recommended for the prevention of food and waterborne disease in high-risk areas. A cholera vaccine is available in Australia; however, it is recommended only for people in a few specific high-risk situations such as workers and local inhabitants in outbreak areas. The vaccine offers up to 86% efficacy against heat-labile forms of enterotoxigenic Escherichia coli, which equates to about 30% of all E. coli diarrhoea but less than this for all causes of diarrhoea.6 Travellers at high risk or desiring maximum protection should be given this information when offered the vaccine.
Nonantimicrobial products
A number of probiotics and bovine colostrum-based products are available over the counter, some of which have gained popularity. However, it is important for GPs to be aware of the absence of a scientific basis or evidence for the use of these products. They are not recommended in any current guidelines.3
Antibiotic prophylaxis (chemoprophylaxis)
Antibiotics are generally not recommended for prophylaxis in travellers.3 They offer no protection against nonbacterial causes; may alter the normally protective gut microbiome; can result in resistant infections in the host including Clostridium difficile; add to the global burden of multidrug-resistant organisms; and may result in allergic reactions or other undesirable side effects. However, antibiotics may be considered for immune-compromised travellers who are at high risk of severe infectious disease.2 Rifaximin is recommended in this situation (off-label use) as it primarily works in the lumen of the gut and has minimal systemic absorption.3
Self-treatment
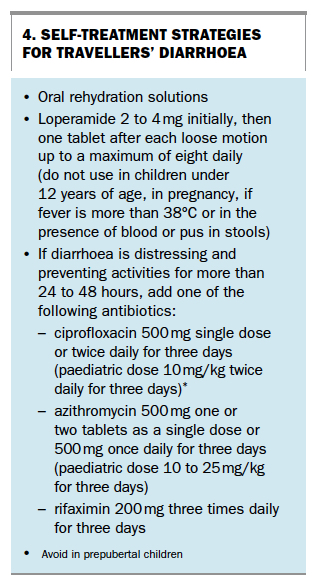
As a first step for the self-treatment of TD, the use of an oral rehydration solution is important as it helps avoid dehydration, a common reason for hospital admission and treatment. This is especially important in children, women who are pregnant and in the elderly.
As a second step, loperamide is recommended as an additional way to prevent dehydration. It is preferred over diphenoxylate/atropine owing to the risks of adverse reactions to this combination, but is not approved for use in Australia for children under 12 years of age, women who are pregnant and those with a fever of more than 38°C or with blood or pus in their stools. However, even when used in this setting loperamide has been shown to be more effective when combined with an antibiotic than when used alone (and shortens the duration of diarrhoea).7 Self-treatment strategies are outlined in Box 4.
{kind=link}
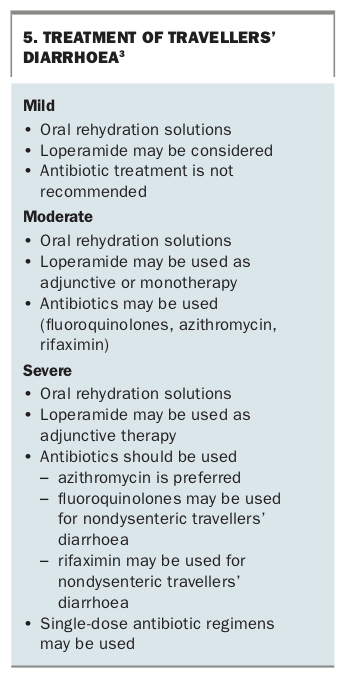
As a third step, antibiotics may be considered for moderate diarrhoea and should be used for severe diarrhoea (Box 5).
{kind=link}
It is important to give the traveller both verbal and written instructions on self-treatment of TD, and there are a number of resources to aid in this (Box 6). In addition to the following advice, travellers need to be encouraged to seek professional medical advice if their condition worsens or fails to improve over 48 hours, if they develop a high fever, blood in stools or if they are concerned. If medical help is not available locally, most travel health insurance companies provide an emergency contact number for initial phone advice and recommendations about the nearest medical assistance.
{kind=link}
Although using antibiotics for prophylaxis is problematic and therefore generally avoided, their use for the treatment of severe TD is recommended. Although most TD is mild and will resolve within one week (whether treated or not), some will progress to severe disease with consequent restriction of their ability to travel. Self-treatment is recommended and more realistic for travellers who are unable or prefer not to access medical care when away. This typically applies to destinations where an adequate or acceptable standard of medical care may not be available (e.g. trekking or in underdeveloped settings) or in cases of professionals on a short trip who, for example, cannot afford to miss a meeting or lecture. Although resistance to antibiotics is increasing worldwide, this is generally recognised as being due to overuse of antibiotics in stock feed and some community settings rather than due to GP prescribing or traveller self-treatment.8,9
Fluoroquinolones have been used for many years with good effect and have the advantage of being generally safe and of having a low risk of adverse reactions. Norfloxacin is no longer available in Australia, so ciprofloxacin has become the most commonly prescribed quinolone for use in travel health. The use of this class has been somewhat tempered due to concerns regarding the potential for resistance, adverse effects on the gut microbiome and rare adverse reactions such as Achilles’ tendon rupture. Although resistance to treatment of Campylobacter and Shigella species has been described in Southeast Asia, there is little evidence of significant treatment failure in TD. Ciprofloxacin remains useful for short-term self-treatment for most travellers for TD, and has the additional benefits of use for skin, urine and respiratory infections.
Azithromycin is as equally efficacious as fluoroquinolones in the treatment of TD and is preferred for dysentery and in those with a high fever. It has the advantages of being effective for Campylobacter and Shigella species in Southeast Asia, can be used in young children and in women who are pregnant, and covers many bacterial upper respiratory infections. However, it notably can cause gastrointestinal side effects and is generally not as well tolerated as ciprofloxacin. Tinidazole or metronidazole are recommended where Giardia lamblia is suspected, such as in those who have persistent TD. Rifaximin recently became available in Australia and works primarily as an endoluminal antibiotic due to it being poorly absorbed. For this reason, it is not recommended where systemic infection due to invasive organisms is suspected, such as may occur in travellers with high fevers or bloody stools.
Diagnostic testing
Microbiological testing is recommended for returned travellers who have persistent symptoms with or without prior treatment. Stool microscopy and culture lacks sensitivity so when a negative result is given, or a rapid result is required, molecular diagnostic testing (polymerase chain reaction) should be considered. Most community-based laboratories now offer it. The combination will have greater sensitivity in detecting some parasites and will also detect some viral diseases, alleviating the need for antibiotics.
Conclusion
Travellers’ diarrhoea remains one of the most common problems faced by travellers both locally and internationally. Although most travellers present to their GP primarily for vaccinations and/or malaria prophylaxis, it is important for the clinician to spend some time discussing the risk of acquiring TD and providing prevention strategies. This will involve consideration of the area to be visited, type of travel and type of traveller. The responsible use of antibiotics in self-treatment in particular needs to be clarified bearing in mind the risks and potential benefits for each traveller’s individual circumstances. MT