Three tools for managing vertigo in the frontline

Vertigo is a challenging symptom in general practice. With access to three tools – a focused history, eye examination and a management algorithm – a large proportion of vertiginous patients could be managed effectively by GPs. This practical guide seeks to increase the skills and confidence of frontline practitioners when managing vertigo.
Linked videos
There are videos available for this article, which can be accessed here.
- A structured history (Tool 1) enables identification of the vestibular syndrome underlying vertigo symptoms. Vertigo can be subdivided into acute, episodic and chronic vestibular syndromes.
- An eye examination (Tool 2) identifies the aetiology of the syndrome. For example, is the episodic vestibular syndrome due to benign positional vertigo?
- A management plan (Tool 3) guides the practitioner in offering a treatment specific to the diagnosis.
- Acute vestibular syndromes are best assessed by a specialist.
- The most common episodic vestibular syndrome, benign paroxysmal positional vertigo, can easily be diagnosed and treated in general practice.
- The preferred treatment for chronic vestibular syndrome is vestibular rehabilitation.
Vertigo is a common condition. It has a one-year prevalence of 5%, and prevalence is higher in older age groups.1 Although rarely lethal, its disease burden is large owing to restrictions in daily activities and a lower quality of life, heavy utilisation of healthcare resources and occupational disability among people with vertigo.2-5
The GP may be the first and only doctor to assess vertigo in a patient. GPs manage over 80% of vertigo patients without referral to specialist care.6,7 Not all GPs feel confident to manage vertigo, and readily available vestibular treatments are underutilised.8,9 The fear of missing a life-threatening stroke or fear of performing an examination or intervention that might unleash projectile vomiting is daunting for many able practitioners. Also, nystagmus (the repetitive eye movement that accompanies vertigo) is shrouded in mystery and considered difficult to interpret by many doctors. Consequently, management is sometimes restricted to offering a vestibular suppressant and organising a scan to exclude stroke.
We, the authors, believe vertigo should be viewed differently and that it is worthwhile for GPs to master its management. Vertigo can be considered an exciting challenge in general practice. Often, vertigo has a benign cause; and, with three simple tools (a history, an eye examination and a management plan), many types of vertigo could be both diagnosed and treated by a trained GP. A GP can ‘fix’ most patients with benign paroxysmal positional vertigo (BPV) within 15 minutes and consequently make a great difference to many patients.
Vertigo can be caused by various disorders of the inner ear and brain. A focused history helps to identify the vertigo syndrome by determining the timing and triggers of the patient’s vertigo symptoms and whether they fit the criteria for an acute, episodic or chronic vestibular syndrome (Tool 1). The characteristics of each vestibular syndrome are described below. Once the vestibular syndrome has been identified, the examination is used to diagnose the underlying vestibular disorder (Tool 2). When the best-fit diagnosis or diagnoses have been reached, the management algorithm can be used to investigate further and guide treatment (Tool 3).
Tool 1. The dizzy history
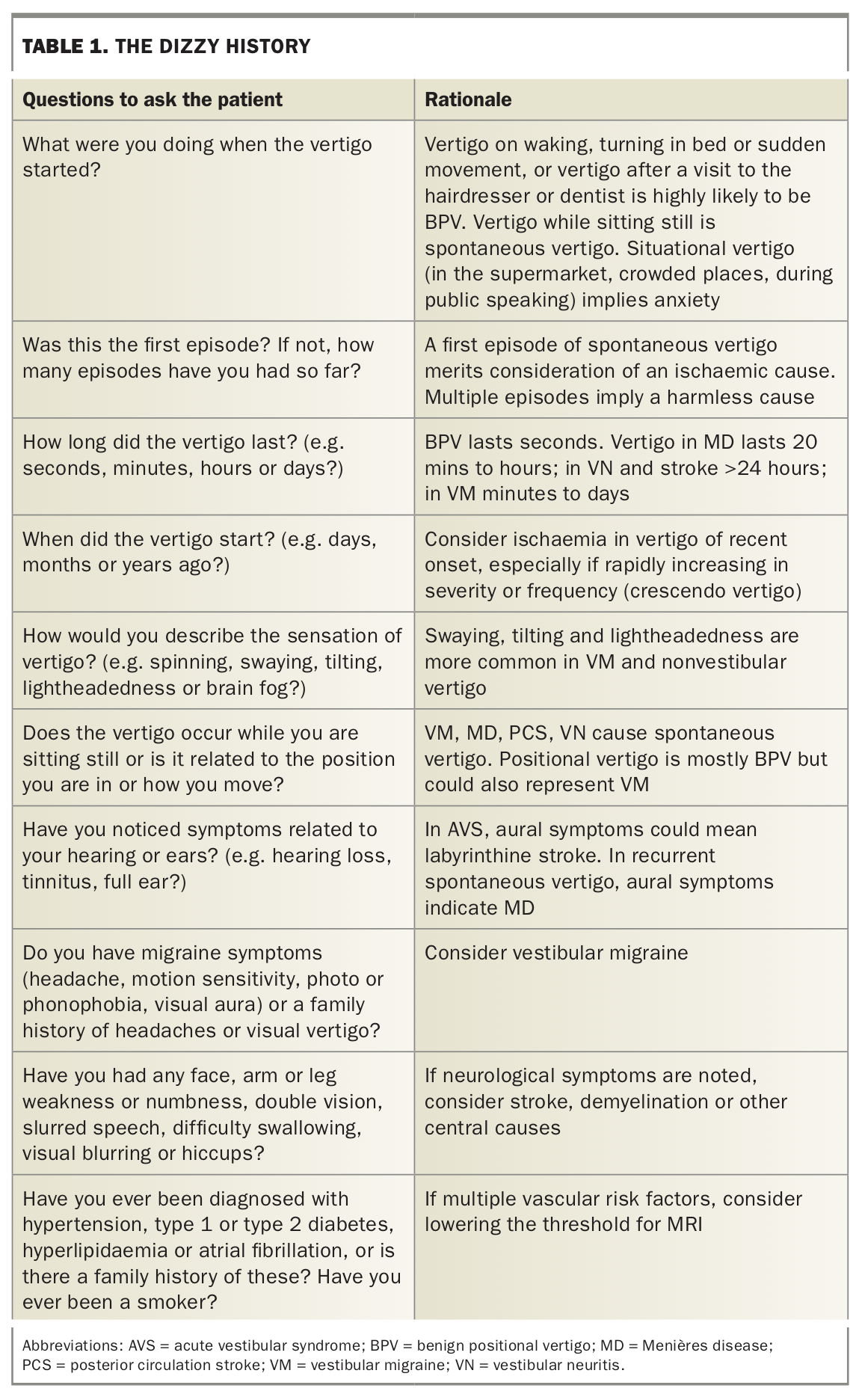
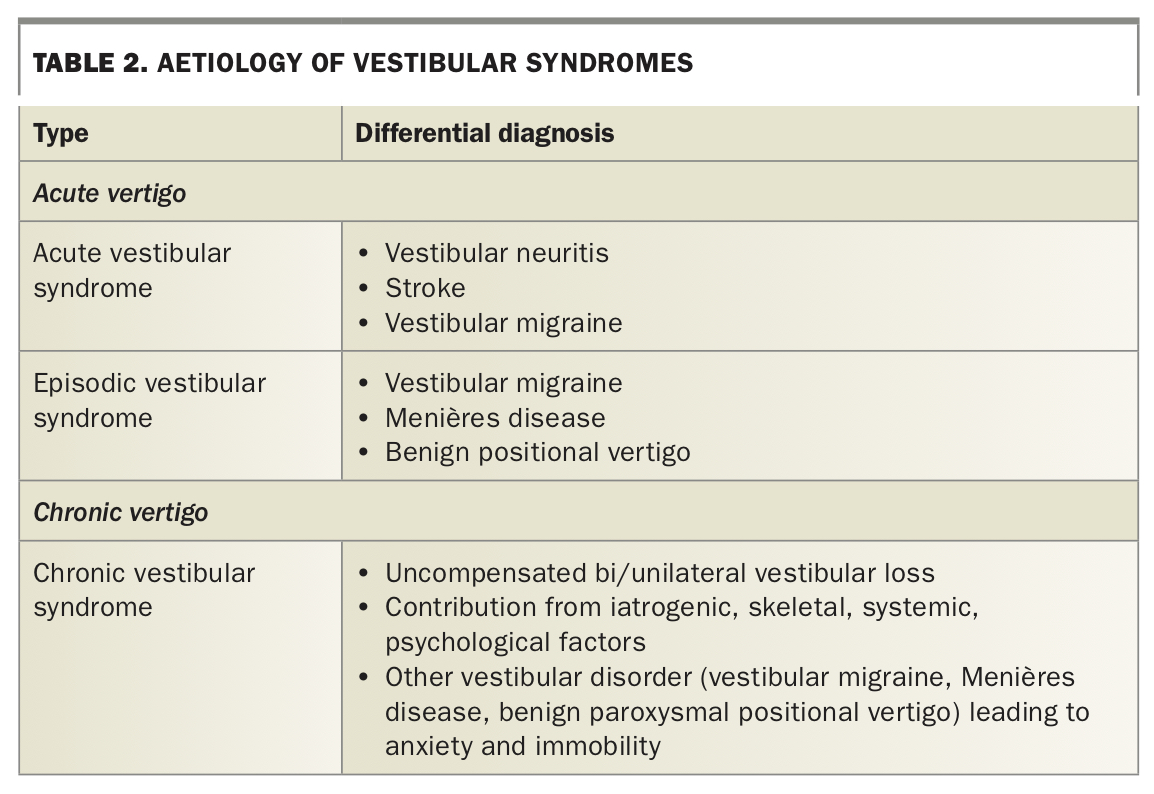
History taking is without doubt the most important step in assessing a patient with vertigo. Table 1 outlines the questions that are worth posing to every patient and why they are important, and it could be used as a template for history taking. The history shows whether the patient has an acute, episodic or chronic vestibular syndrome, each of which has a short list of differential diagnoses (Table 2). Sometimes the history will establish the diagnosis before the examination.
{kind=link}
{kind=link}
Acute vestibular syndrome history
In an acute vestibular syndrome (AVS) there is acute-onset, continuous vertigo, lasting days to one week. The vertigo is persistent for a day or more, which differentiates it from an episodic vestibular syndrome. The symptoms may be exacerbated by moving the head, but movements do not actually trigger the vertigo. This distinction will need to be carefully elicited in the history.
AVS could represent vestibular neuritis or stroke. Vestibular neuritis (VN) is thought to be a viral or postviral inflammatory disorder affecting the vestibular end organs or vestibular portion of the eighth cranial nerve. In strokes that cause AVS there is generally vertebrobasilar ischaemia of the brainstem or cerebellum. Both stroke and VN can present with isolated vertigo, and therefore the history may not help separate them. Sometimes, stroke may be accompanied by new neurological symptoms such as headache, dysarthria, dysphonia, diplopia, face or limb weakness, ataxia or sensory disturbance. Sometimes VN may have a viral prodrome. Sudden hearing loss and tinnitus are not encountered in VN and are red flags for a labyrinthine stroke. Patients with an acute vestibular syndrome should be referred to the emergency department (ED).
Episodic vestibular syndrome
An episodic vestibular syndrome is characterised by recurrent vertigo attacks, lasting seconds to hours or, rarely, days. In between attacks patients are asymptomatic. Recurrent vertigo could be caused by changes of the head position (recurrent positional vertigo) or it could be vertigo that occurs without an obvious positional trigger (recurrent spontaneous vertigo).
Recurrent positional vertigo
Recurrent positional vertigo is almost always caused by BPV, the most frequent cause of vertigo encountered by GPs. BPV is believed to be caused by calcium carbonate particles or ‘crystals’ being dislodged from our gravity sensors, or otolith organs, into the semicircular canals where they activate vestibular afferent neurons, causing vertigo. Although all three semicircular canals can be affected, the posterior canal is the one involved in more than 90% of instances.10 Head movement (turning in bed, getting in and out of bed, reaching for a bookshelf, hanging out clothes, tying shoelaces, instilling eye drops) causes sudden spinning vertigo, lasting seconds to a minute. Vertigo after a visit to the hairdresser or dentist is highly suspicious for BPV. As patients age, they may not provide this classic history but instead present with recurrent falls or a wobbly gait.
Recurrent spontaneous vertigo
When vertigo is recurrent but occurs spontaneously (when sitting quietly) two diagnoses should be considered: vestibular migraine (VM) and Menière’s disease (MD). Vestibular migraine, although relatively newly defined, is by far the more common cause of recurrent spontaneous vertigo.11 It can be considered a migraine variant with vestibular symptoms, although the exact pathophysiology is still poorly understood.12 Ideally, there would be a temporal association between vertigo and headache, photophobia or phonophobia, but this is not always clear.13 Sometimes the patient may have a lifelong history of motion sensitivity or a past history or family history of migraine. The vertigo attacks last minutes to hours and can be triggered by excessive stress and lack of sleep, food or fluids.
It can be difficult to distinguish vestibular migraine from MD. Thought to be caused by excessive build-up of endolymphatic fluid in the inner ears, MD is better known but far less common than VM. In MD, the spontaneous vertigo attacks also last minutes to hours, but they are more often associated with aural symptoms such as hearing loss, tinnitus or aural fullness. As MD progresses over the years, the vertigo attacks often diminish and hearing loss becomes permanent. However, the history and physical examination are not always enough to differentiate between VM and MD and referral to a specialised dizziness clinic is sometimes needed.
Chronic vestibular syndrome
Chronic vestibular syndrome is characterised by chronic persisting disequilibrium that lasts for months to years and can be caused by many conditions. Finding out when the vestibular symptoms first started is useful. Patients may have experienced an acute vestibular syndrome caused by vestibular neuritis, with incomplete recovery resulting in chronic vestibular symptoms. Episodic vestibular syndrome caused by MD or vestibular migraine may result in chronic symptoms of imbalance and ataxia in between vertigo attacks.
It may be impractical to find the cause of the chronic vestibular syndrome in general practice. Instead of solely focusing on the cause it is also important to find out what triggers unpleasant vestibular symptoms in daily life. When the vestibular system is injured, central mechanisms (vestibular compensation) are activated that eventually reduce symptoms of vertigo. If this repair mechanism fails, chronic vestibular symptoms occur. Insufficient stimulation of the vestibular system is always an important and modifiable factor in chronic vestibular syndromes. Fear of vertigo may prevent patients from moving their head or undertaking activities, but this will cause symptoms to persist in the long term. Comorbidities such as psychiatric disorders, musculoskeletal problems, sensory impairment and long-term use of vestibular suppressants are also associated with the development of chronic vestibular syndrome. The history should be aimed at determining triggers of vertigo and reasons that prevent patients from challenging their vestibular system.
Tool 2. The dizzy examination
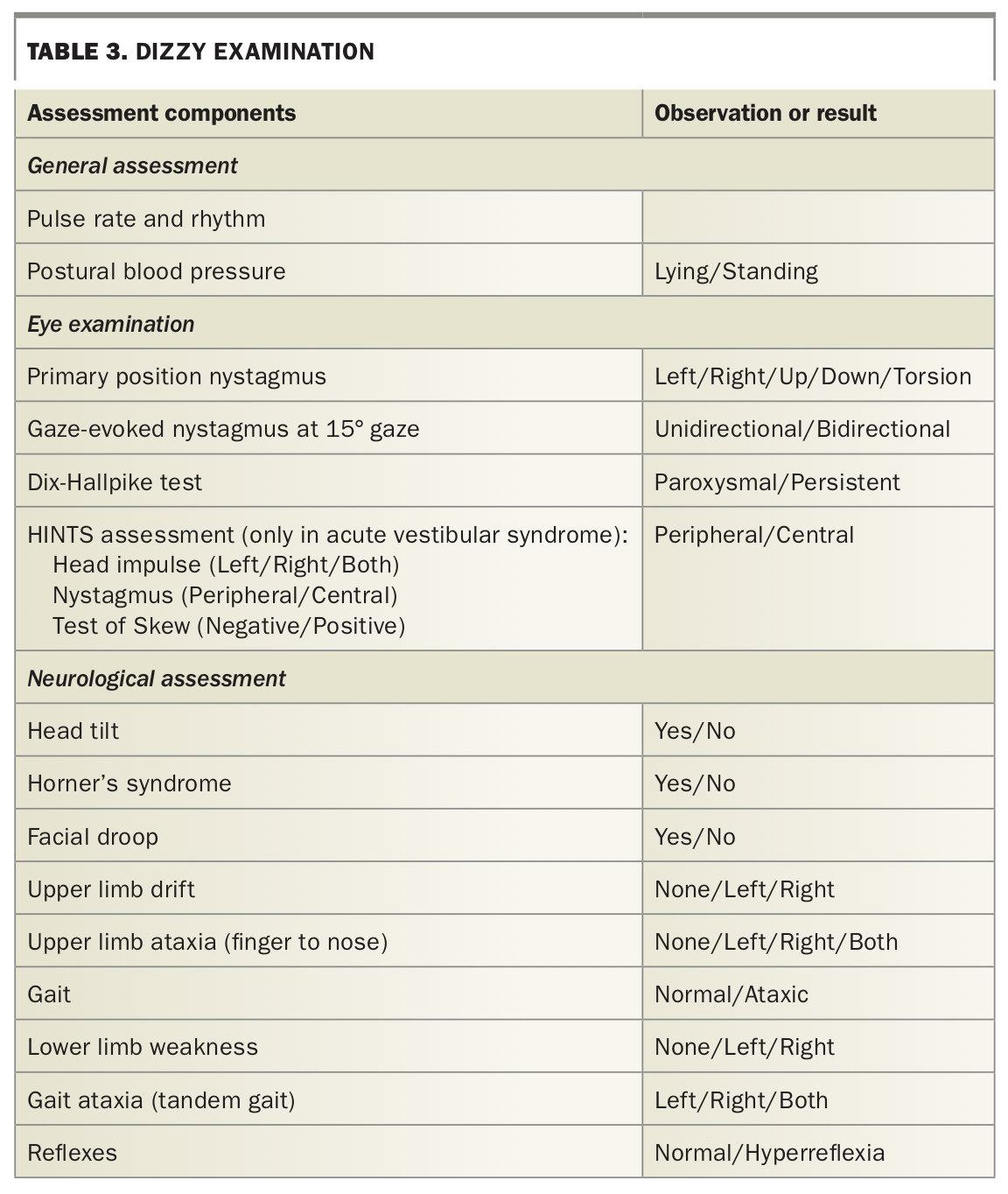
The physical examination consists of a general assessment, screening neurological assessments and a focused eye examination and is outlined in Table 3, which could be used as a checklist template. Often, history and examination (Tools 1 and 2) together may suffice to diagnose your patient’s condition.
{kind=link}
Acute vestibular syndrome
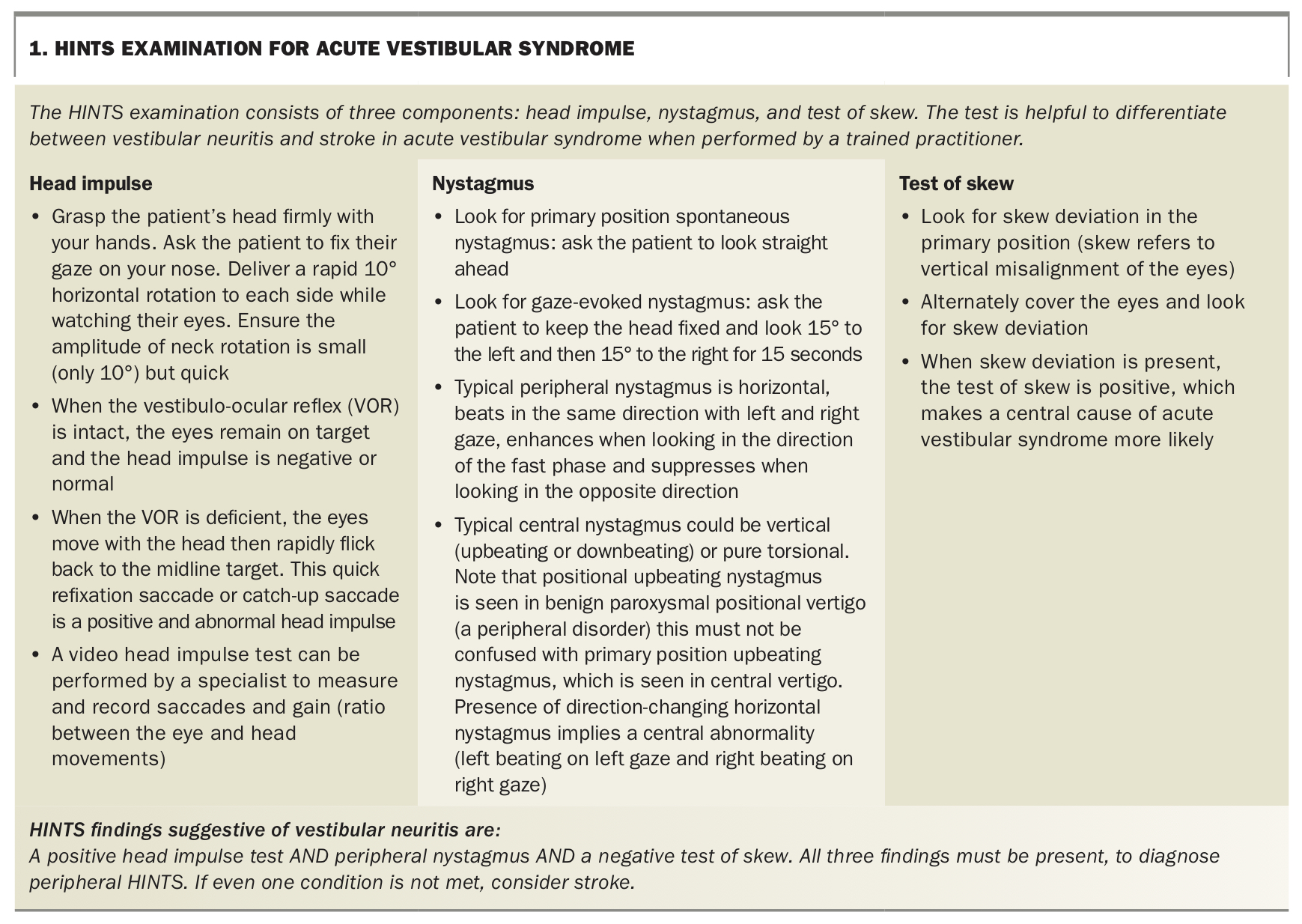
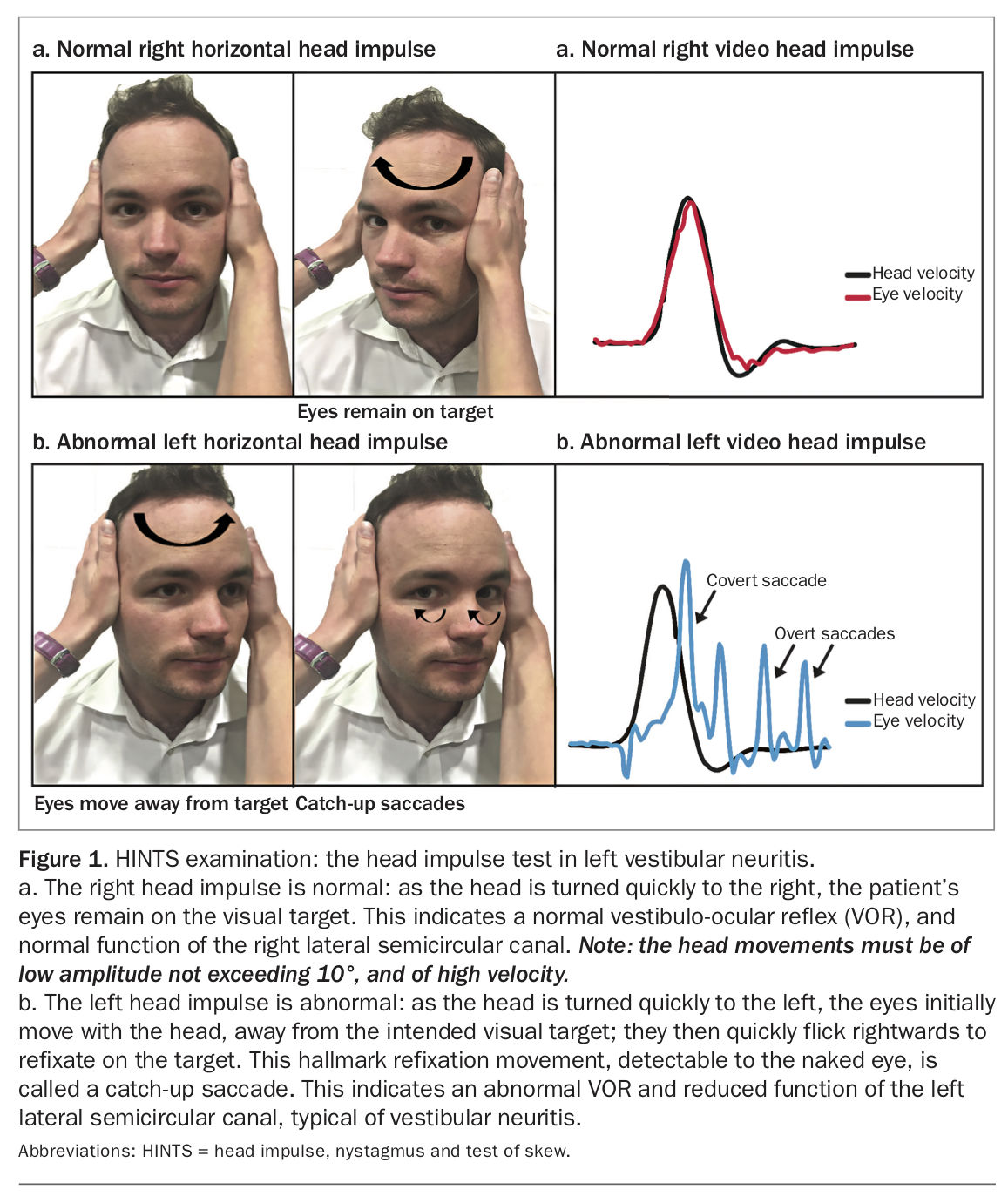
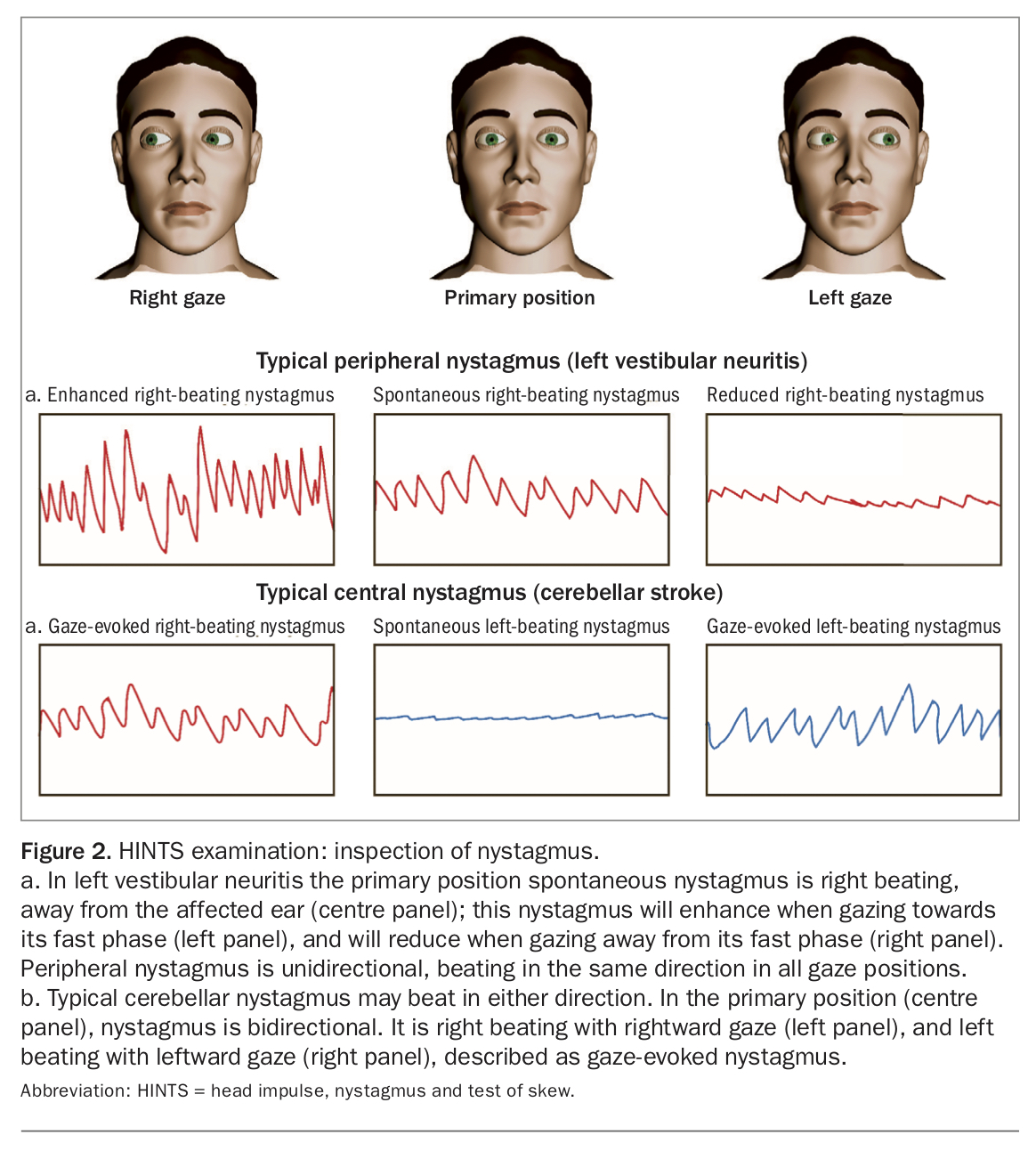
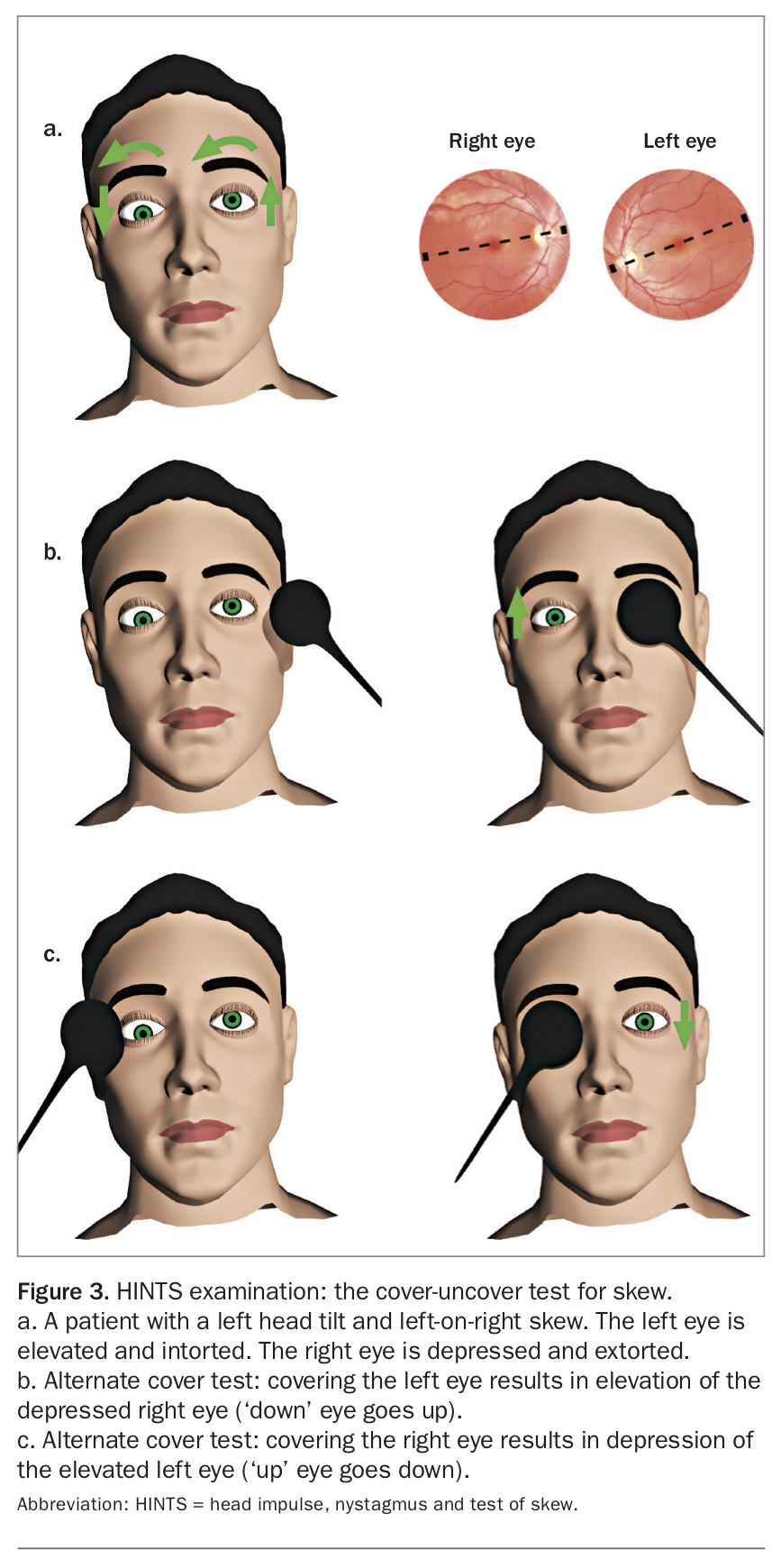
The physical examination can help to further differentiate between the two most common conditions that cause AVS: vestibular neuritis and stroke. Pulse rate and blood pressure may be increased in both vestibular neuritis and stroke, and a newly discovered irregular heart rhythm may indicate a potential embolic source for stroke. The HINTS (head impulse, nystagmus, test of skew) examination, a careful examination of eye movements, is a promising diagnostic tool for differentiating vestibular neuritis from stroke when conducted by a trained practitioner (Box 1; Figure 1, Figure 2 and Figure 3; Videos 1, 2a to 2d and 3 [videos are available with the online version of this article at https://medicinetoday.com.au/vertigovideos]).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Studies have shown that the HINTS examination can be even more sensitive than neuroimaging when conducted properly by a trained physician. It is important that GPs develop experience using the HINTS assessment. Since experience using HINTS is variable, however, we advise referral of all patients with an acute vestibular syndrome to the ED to exclude stroke.
Episodic vestibular syndrome
In patients with episodic (recurrent) vestibular syndrome, the general and screening neurological assessment may show no abnormalities. In patients with recurrent spontaneous vertigo, primary position spontaneous nystagmus may be observed if they happen to be assessed during an attack. In MD, primary position nystagmus is almost always horizontal. In VM it could be horizontal, vertical or torsional. If the attack has abated, there may be no primary position nystagmus. Many nystagmus types are suppressed by bright light and are therefore undetectable.
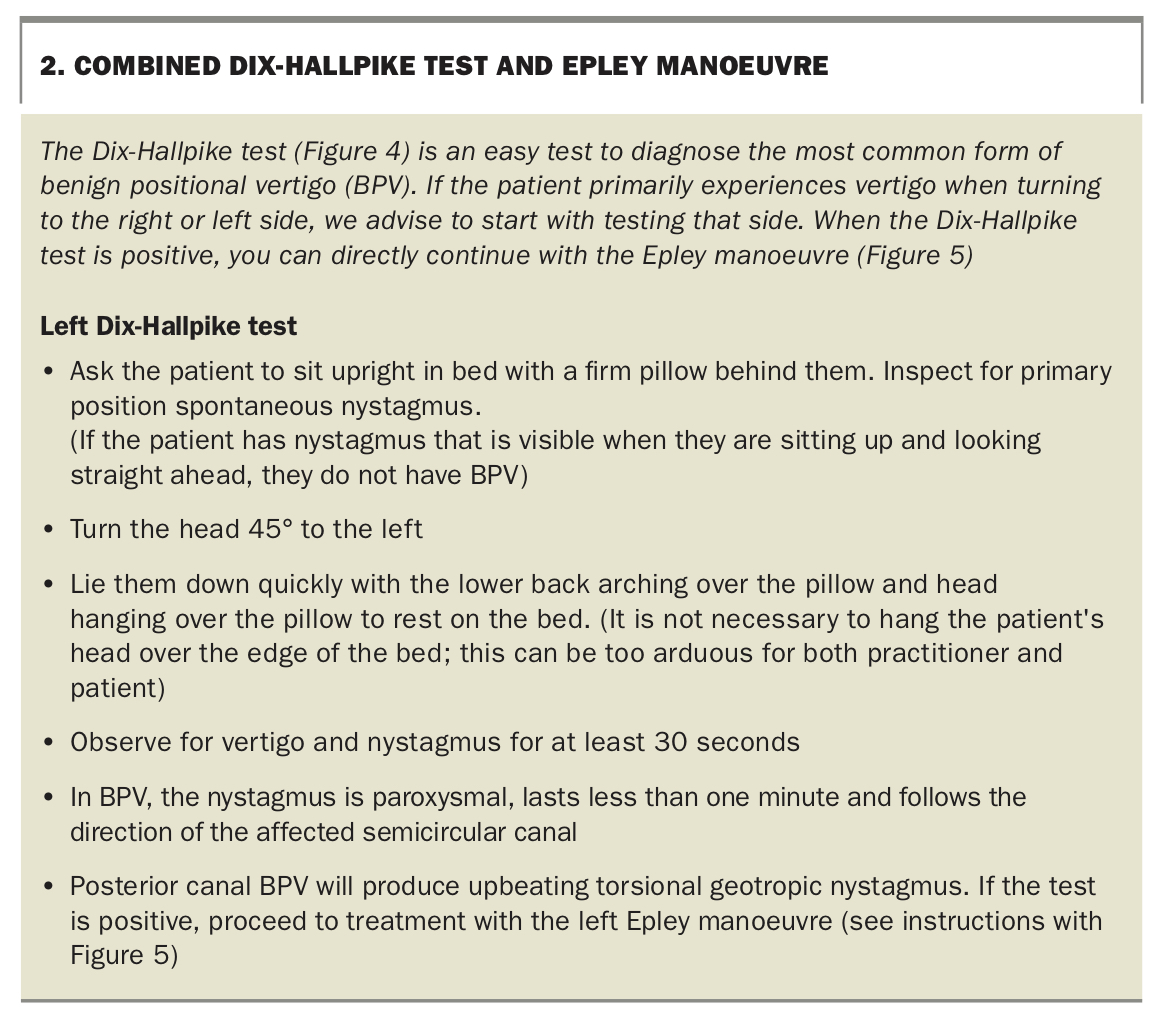
If the patient’s history indicates recurrent positional vertigo, a definitive diagnosis of BPV can be made by performing the Dix-Hallpike test (Box 2; Figure 4; Videos 4a and 4b [https://medicinetoday.com.au/vertigovideos]). The diagnosis of posterior canal BPV is confirmed when the Dix-Hallpike test causes vertigo and, after a short latency period, torsional upbeating nystagmus is seen. We advocate performing a Dix-Hallpike test on all patients presenting with vertigo, since it offers an opportunity to detect and alleviate an easily treatable cause of vertigo.
{kind=link}
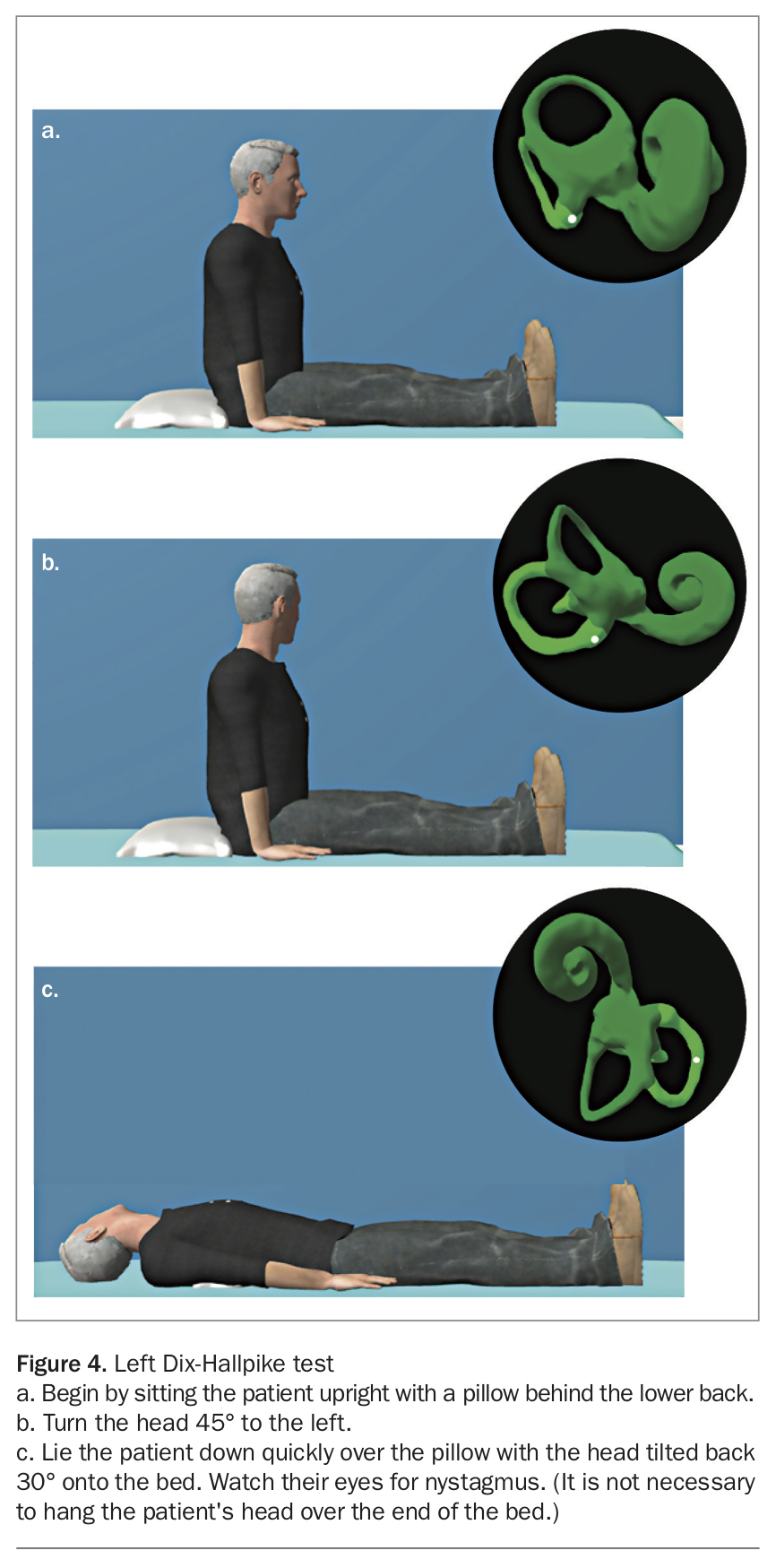{kind=link}
In patients with spontaneous vertigo of any cause (VM, MD, VN, stroke) who have spontaneous nystagmus, enhancement of this nystagmus will occur in the Hallpike position. Typical BPV is paroxysmal; the nystagmus begins and stops within the span of one minute. If the nystagmus continues for as long as the head remains in the Hallpike position, it is unlikely to be posterior canal BPV.
Chronic vestibular syndrome
In chronic vestibular syndrome the physical examination may not always identify the cause of the symptoms, but it helps determine factors that contribute to the vestibular problem. Orthostatic hypotension, a drop in systolic blood pressure of more than 20 mmHg on standing up, should be screened for in every patient. The head impulse test may reveal uni- or bilateral vestibular loss. Primary position nystagmus may be absent if the vestibular event occurred a long time ago. Patients with bilateral vestibular loss also have difficulty performing a matted Romberg test (standing on foam with eyes shut) or a tandem Romberg test (tandem stance with eyes shut). Gait can be wide-based, and tandem gait may be ataxic in patients with peripheral and central vestibular system dysfunction (as well as in cerebellar ataxia and severe peripheral neuropathy). We recommend assessing all patients with chronic vestibular syndrome for BPV, as older patients with untreated BPV often present with chronic imbalance.
Tool 3. The dizzy management plan
Our management plan for patients with vertigo in primary care is presented in the Flowchart. All patients with an acute vestibular syndrome require assessment in the ED. After discharge, patients with persisting vertigo should be offered vestibular rehabilitation. In patients with episodic vestibular syndromes, positional vertigo requires a search for and treatment of BPV.
The Epley manoeuvre is a relatively simple and proven treatment for posterior canal BPV (Box 2; Figure 5; Video 5 [https://medicinetoday.com.au/vertigovideos]). It is safe, effective and within the capability of any medical practitioner, although it is currently underutilised, owing to false perceptions of complexity.9,14,15 We encourage widespread use of the Epley manoeuvre as a most rewarding treatment in general practice, since many patients with BPV can be ‘cured’ with a single treatment performed in less than 15 minutes.14
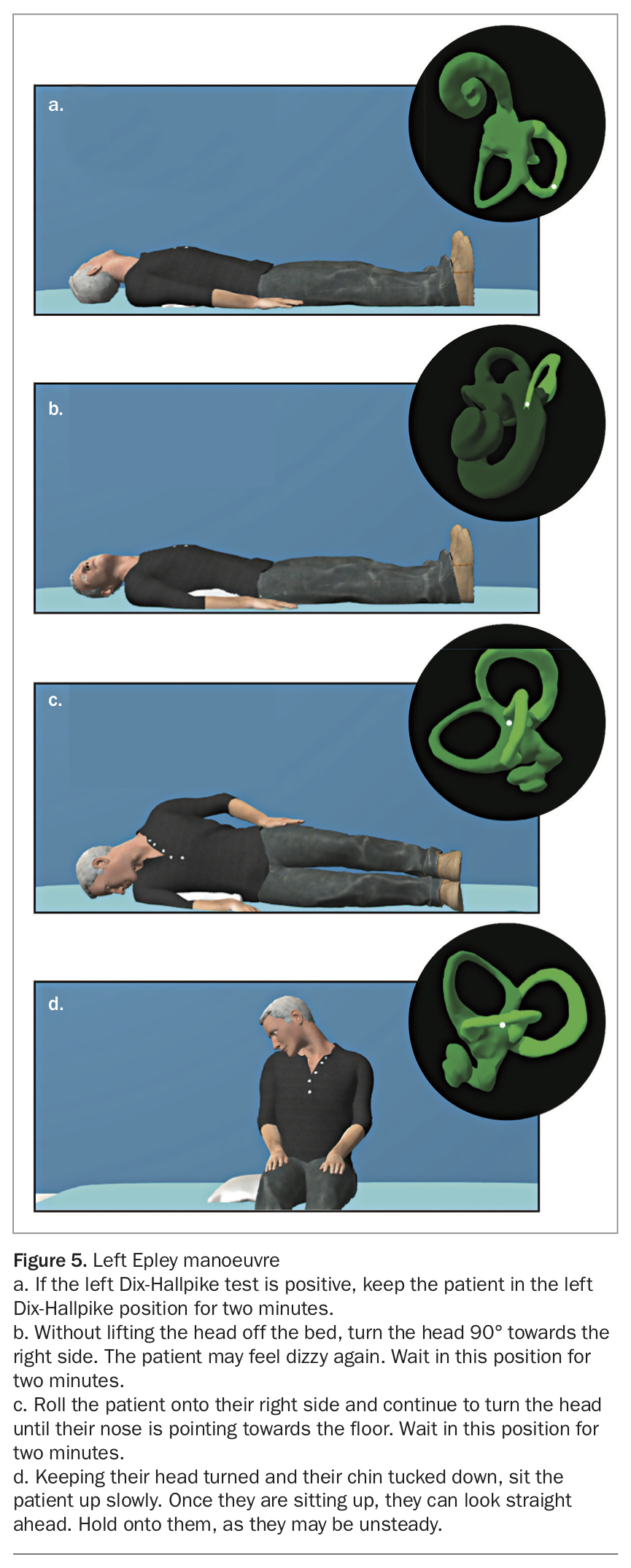{kind=link}
If the patient is nauseated, they could be premedicated with prochlorperazine and ondansetron 15 minutes before carrying out the manoeuvre. If the patient is obese, consider requesting the assistance of a colleague. A patient who is unable to arch backwards due to scoliosis or a stiff neck could benefit from being treated while on a trolley that can be tilted backwards.
For patients with episodic spontaneous vertigo, diagnostic work-up can be started in general practice while awaiting review in a dizzy clinic. The audiogram is an essential test that may reveal fluctuating hearing loss diagnostic of MD (Figure 6). For patients with vestibular migraine, it is important to reassure them that, as for other forms of migraine, the condition is bothersome but not dangerous. Common migraine triggers such as excessive stress or lack of sleep, food or fluids should be avoided, and regular exercise can reduce symptoms of vertigo.16 When the vertigo attacks are frequent and disabling, prophylactic medication should be considered. Riboflavin (400 mg daily) and magnesium (300 mg equivalent Mg) could be started. In suspected MD, patients should be advised to initiate a low-salt diet. All patients with recurrent spontaneous vertigo should be provided with emergency drugs (e.g. prochlorperazine 5 mg or cinnarizine 25 mg for vestibular suppression, and ondansetron 4 to 8 mg for nausea). Patients should be instructed to carry the drugs with them and use them sparingly to alleviate vertigo, but never to use them when they are symptom-free.
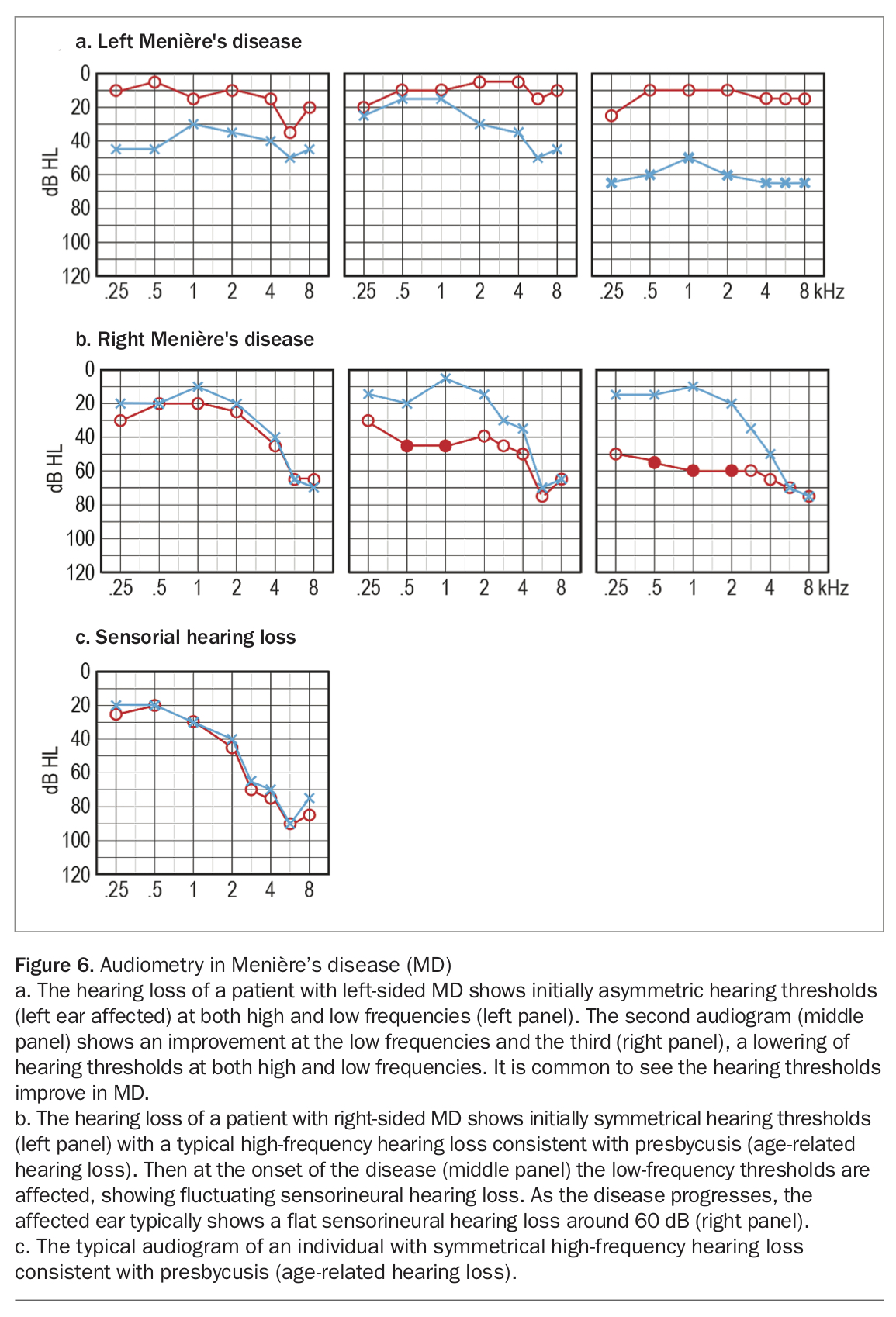{kind=link}
Chronic vestibular syndromes require a meticulous work-up for the underlying causes (Flowchart) and initiation of self-directed or supervised balance rehabilitation. Vestibular rehabilitation is a safe and effective treatment for chronic imbalance.17 GPs can refer patients to a specialised physiotherapist for treatment, or direct patients to a freely available online vestibular rehabilitation intervention developed by the University of Southampton (https://balance.lifeguidehealth.org).18 If there is a significant contribution from anxiety, consider referral to a psychologist with experience in treating dizzy patients.
Referring the dizzy patient
Vertigo affects one to two million Australians each year. To optimise their management, the combined efforts of GPs, otolaryngologists, nurse-practitioners, neurologists, physiotherapists and emergency physicians are needed. We believe that vertigo should not fall exclusively in the domain of the ‘neuro-otologist’ and can be managed effectively by many healthcare professionals with access to the correct tools. We expect that, in the future, GPs with subspecialty expertise in vertigo will exist in Australia.
Patients with acute vestibular syndromes are best referred to the ED; yet there may be instances (e.g. regional general practice settings) where the practitioner is more skilled in vertigo assessment than the ED service. In these instances, it is best that the GP undertakes the HINTS assessment, organises urgent MRI scanning for those patients with a central cause of vertigo (since CT scanning to exclude posterior circulation stroke is not conclusive) and initiates antiplatelet therapy pending review by a neurologist. BPV can often be managed successfully by the GP without specialist referral unless it is refractory to bedside treatment. Many GPs will correctly choose to refer ‘difficult’ patients to an expert physiotherapist, ear, nose and throat specialist, or neurologist who is experienced in treating BPV. Patients with episodic spontaneous vertigo could start their diagnostic work-up (audiometry) and management (lifestyle changes, salt restriction, trial of magnesium or riboflavin for migraine) while awaiting review by an otolaryngologist, neurologist or dizzy clinic. Patients with chronic vestibular syndromes may be referred to a neurologist or ear, nose and throat specialist or dizzy clinic for initial diagnostic work-up and managed by a team led by the GP with the participation of the specialist, a physiotherapist and a psychologist as required.
Conclusion
The first step when assessing patients with vertigo in general practice is to determine whether the symptom is acute, episodic or chronic. Once the syndrome is identified, the history and examination will help identify possible vestibular disorders. Using the three tools described, assessment and management of vertigo may prove easier and more rewarding for the GP. MT