Acute psychosis: community care after hospital discharge

Dr Carr is a Clinical Senior Lecturer (Honorary) at Melbourne University; and a General Practitioner at St Kilda Medical Group, Melbourne, Vic.
Professor Harris is Head of the Discipline of Psychiatry at Sydney Medical School, The University of Sydney; Clinical Director of the Brain Dynamics Centre at the Westmead Institute of Medical Research, Sydney; and Staff Specialist at the Prevention Early Intervention and Recovery Service, Western Sydney Local Health District, Sydney, NSW.
Psychotic disorders
Mental health

Successful transition of a patient back to community care after an episode of acute psychosis requires good communication between the hospital and GP, and clear planning. GPs have a crucial role in ensuring medication concordance and psychosocial support, and monitoring the patient’s physical health needs.
- Community care of patients with a psychotic illness requires good communication between specialists, GPs and mental health services; this remains a challenge.
- Antipsychotic medication is an essential foundation for recovery after an episode of acute psychosis; however, more than medication is needed.
- Patients often discontinue antipsychotic medications; careful discussion and monitoring can help improve medication concordance.
- GPs can use their knowledge of local services to refer patients for appropriate psychosocial support and rehabilitation.
- The physical health of people with psychosis is easily overlooked but is a key responsibility of the GP.
The patient with acute psychosis has seen the community mental health team and been treated in an inpatient psychiatric unit, their medication has been optimised and the psychotic symptoms are reasonably under control. The psychiatrist is now ready to transfer the patient back to the GP in the community. What happens now?
In a previous article in the April 2020 issue of Medicine Today, we discussed the important role of GPs in the initial identification and triage of patients with acute psychosis.1 Here, we describe the role of the psychiatrist and the GP in the follow-up phase, after an acute episode of psychosis has resolved and the patient is discharged back to community care.
Discharge planning
Good discharge planning starts on patient admission, is undertaken in advance of discharge, involves the patient and their supports, including their GP, and links the specialist care received in hospital with future recovery or rehabilitation. Discharge planning is often noted by its absence, when a patient arrives unannounced in the GP’s office with no paperwork and no forewarning. Planning that is done well decreases the risk of readmission and improves treatment concordance.2
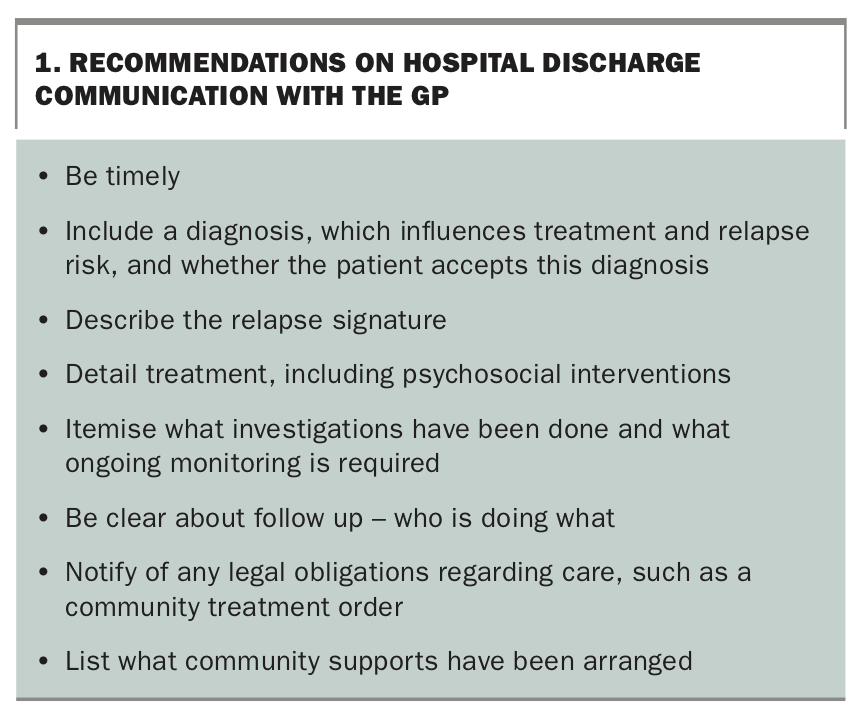
We recommend that someone from the treating team telephones the GP. This may be the psychiatrist, case manager, pharmacist or other team member, depending on local circumstances. A telephone conversation gives the opportunity to gauge the GP’s knowledge of the patient and their illness, and to clarify information and future roles. Recommended points that should be covered in good discharge communication are outlined in Box 1.
{kind=link}
A telephone call to the GP is also a matter of professional courtesy. Psychiatric patients tend to be complex, and some GPs are more comfortable than others with their management. A telephone call helps ensure that the GP is happy to accept the patient and has the skills and availability to provide the service needed. A failure in discharge planning should elicit feedback to the mental health team or inpatient psychiatric unit – this is a critical time of risk for the patient, and the mental health services must communicate clearly with the GP.
Community management after discharge
Psychosocial rehabilitation
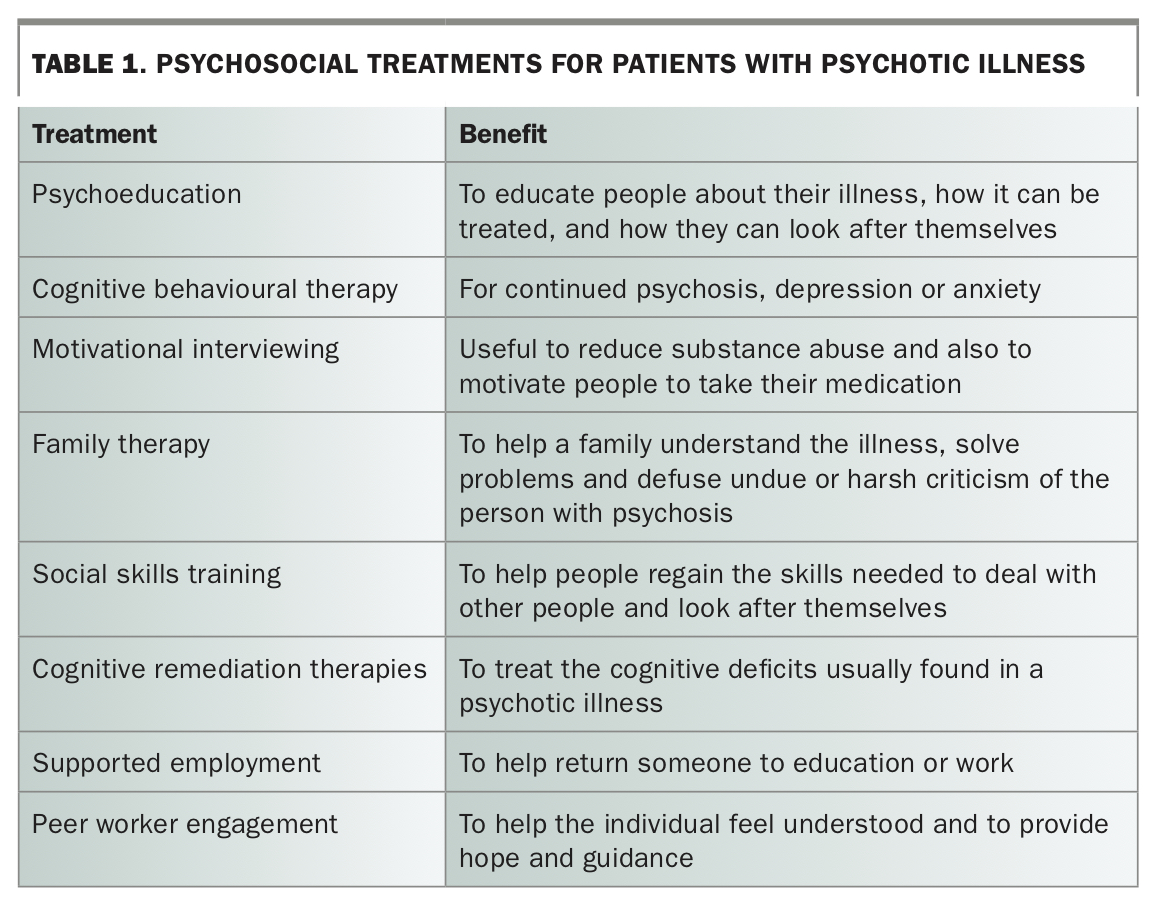
Any psychotic episode can be deeply disturbing for the patient. A first episode can be particularly distressing and destabilising. The patient is likely to have lost confidence and be anxious about the future. There is good evidence that psychosocial support and rehabilitation improve outcomes.3-5 Involving family and carers also improves outcomes.6 Some possible psychosocial treatments are outlined in Table 1.
{kind=link}
The psychosocial treatments selected will depend on the individual patient and local resources. The range, quality and availability of services vary significantly across Australia, and between urban and rural or remote settings. Community organisations such as churches, self-help groups and meal services can offer significant levels of social support.
Optimal structured treatment involves a combination of interventions offered to the individual and their family, starting with psychoeducation. An assessment of the person’s skills and cognitive function is a useful platform on which to build but requires specialist (often expensive) input from a clinical psychologist or neuropsychologist and an occupational therapist. This may be of great benefit if an application to the National Disability Insurance Scheme is being considered. Help from a community mental health specialist can often be facilitated by the GP developing a mental health care plan and referring the patient under the Better Access to Mental Health Care scheme.
Psychosis is extraordinarily isolating for the person who experiences it and for their family. Families and patients derive great psychological support from the simple act of contact, of being remembered and ‘kept in mind’.7
Medication concordance
Medication is the cornerstone of management of schizophrenia. Medication usually needs to be continued long term, as relapse is highly likely if it is ceased too soon. After the first episode of schizophrenia, the relapse rate has been estimated as 60 to 80% with medication discontinuation.8 If the broader concept of first-episode psychosis is used, the relapse rate is less, at 53% after 12 months in those who discontinue medication versus 19% in those who are maintained on treatment.9 With established schizophrenia, the risk of relapse is six times higher in those who discontinue medication and three times higher in those who only take their medication intermittently.10
Few patients like taking medications of any kind. Antipsychotic medications all have significant short and longer-term side effects, making them even less popular, and concordance harder to ensure. Nonconcordance in people with schizophrenia is common, with rates as high as 60% at 12 months.11,12
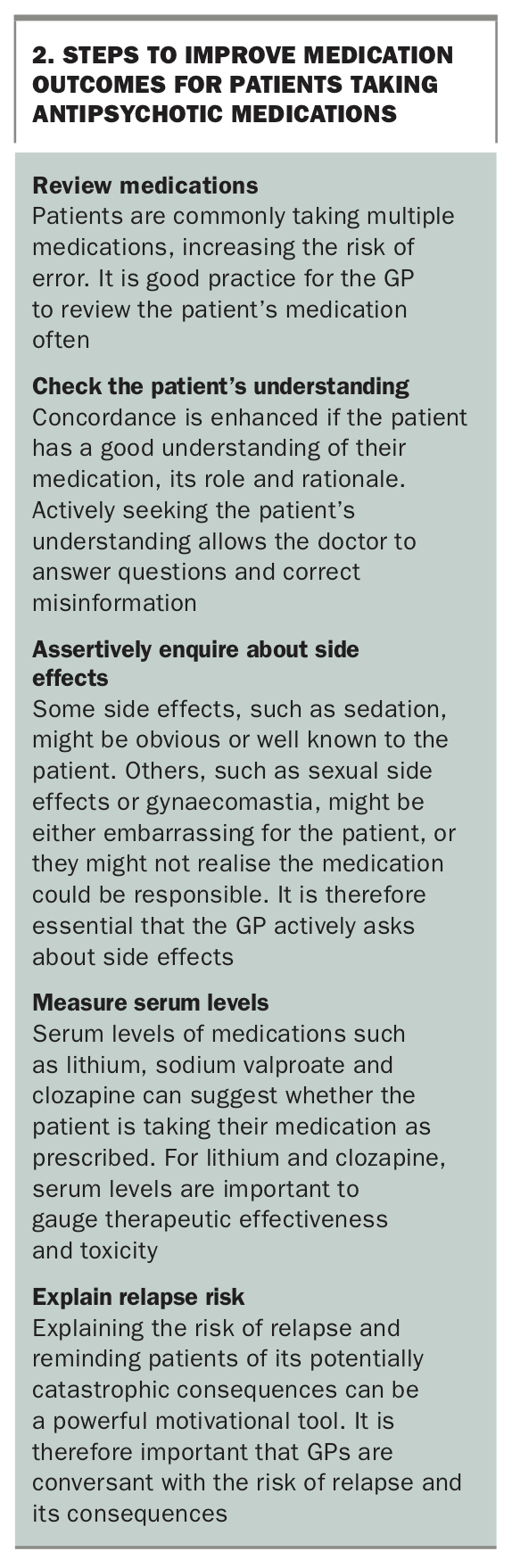
Some steps that GPs can take to help improve medication outcomes are described in Box 2. These strategies to enhance medication concordance will help reduce relapse risk. Long-acting injectable (LAI) therapy should be considered as it is associated with greater concordance and lower relapse risk than oral therapies.13-15
{kind=link}
Recovery
Recovery is a broad concept that encompasses not just the absence of acute symptoms of psychosis but also one of gaining hope, an understanding of one’s capacity and limitations, autonomy and purpose.16 Symptom recovery or absence of relapse do not return the individual to a personally productive and satisfying life; that requires broader intervention than medication alone.
What determines a productive life differs from person to person and evolves with time. Engagement with a range of consumer-oriented services within the local community may help in the process. This process is highly individualised and needs to be responsive to the person, their family and the availability of local services. The well-informed GP is in a unique position to bring this together.
Physical health
People with psychosis are often forgotten when it comes to the usual screening, vaccination and health care that are part of a GP visit. The complexities of managing the psychiatric condition can lead practitioners to relegate physical health to the bottom of their to-do list. However, physical health is of great importance, as people with schizophrenia have on average a 14.5-year reduction in life expectancy.17 Factors contributing to this reduction include a higher rate of metabolic diseases such as diabetes and dyslipidaemia, higher rates of smoking and substance use, poorer diet and less exercise, in addition to a greater risk of suicide and accidents.
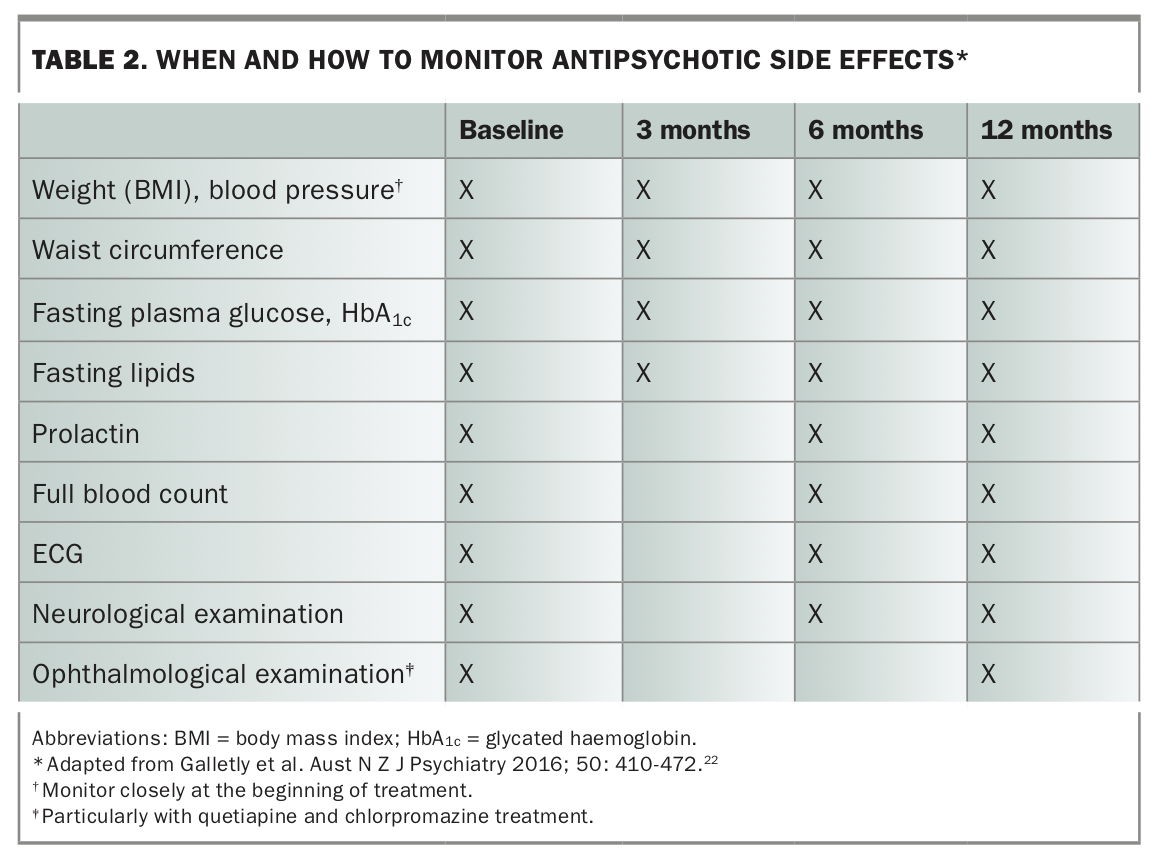
It is therefore crucial that physical health is assertively and recurrently addressed. A recommended monitoring protocol is shown in Table 2. Importantly, the consistent use of antipsychotic medication has been shown to dramatically reduce the risk of all-cause death despite side effects.18
{kind=link}
Diabetes
Schizophrenia is an independent risk factor for diabetes mellitus. In addition, the weight gain associated with many antipsychotic medications also contributes to diabetes risk, alongside the diabetogenic nature of some medicines, such as olanzapine and clozapine.
Cardiovascular disease
Hypertension and hyperlipidaemia are both common in people with schizophrenia and should be managed as for any other patients. Obesity is highly prevalent, with 45% of people with psychosis being obese versus 21% of the general population.19 Regular cardiac monitoring with ECGs should be considered, particularly if the patient is taking medications that affect the QTc interval, such as amisulpride or ziprasidone.
In addition to pharmacological interventions for cardiovascular disease, exercise and dietary interventions are equally, if not more, important for people with psychotic illness than for the general population. Not only do they benefit from improved physical health, but their levels of depression and anxiety are also known to decrease.20
Hyperprolactinaemia
Dopaminergic blockade in the anterior pituitary caused by antipsychotic medications can lead to high levels of prolactin. This in turn causes sexual side effects, gynaecomastia and galactorrhoea and may also be associated with osteoporosis. Reduction in the antipsychotic dose or change to an antipsychotic that is less associated with increased prolactin is recommended.21
Movement disorders
The widespread adoption of the newer antipsychotics has reduced the incidence of movement disorders such as parkinsonism, dystonia, akathisia and tardive dyskinesia; however, these side effects still occur. Regular monitoring for these side effects and a change to an antipsychotic with a lower propensity to cause these problems can be important.22
Smoking
About 60 to 70% of people with schizophrenia smoke, compared with about 14% of Australian adults.23
Smoking cessation
Smoking cessation is more successful when counselling is combined with medication. The three main effective therapeutic agents available in Australia are:
- nicotine replacement therapy (NRT)
- bupropion
- varenicline.
NRT comes in the form of gum, patches and vaping (not currently legal in Australia). Patches are available with PBS subsidy, and so are affordable, and are acceptable to most with few major side effects.
Bupropion is a noradrenaline (norepinephrine) and dopamine reuptake inhibitor that is used overseas as a first-line antidepressant. It is also an antagonist of nicotine receptors, and in Australia is PBS subsidised only as a smoking cessation aid. Its use in psychiatry can be limited by its interactions with other psychotropic medications and the risk of seizures at high doses.
Varenicline has documented neuropsychiatric side effects and has been underused in people with schizophrenia. Recent data suggest that these side effects are less common than previously thought and, with careful monitoring, varenicline is an appropriate option in this population.24,25 Varenicline is also, on current evidence, the most effective agent.
Counselling increases the success of smoking cessation. If face-to-face counselling is not available or not possible, the patient can be referred to Quitline, which provides a telephone counselling service (13 78 48). Quitline staff are trained in the use of quit-smoking medications and have additional training in supporting people with mental health issues.
Smoking and cytochrome induction
GPs need to be aware that smoking induces certain enzymes in the liver cytochrome system, some of which are involved in psychotropic drug metabolism. One of the most important is cytochrome P450 1A2 (CYP1A2), which is involved in the metabolism of several psychotropic medications, particularly olanzapine and clozapine.26 Patients who quit smoking can have a marked reduction in CYP1A2 activity, leading to rises in serum levels of these drugs. Doses may therefore need to be reduced. This is particularly true of clozapine, where serum levels can rise 50% on smoking cessation. The use of NRT does not prevent the rise in serum levels of drugs metabolised by CYP1A2, as it is the polycyclic aromatic hydrocarbons in cigarette smoke that induce CYP1A2 .
Screening and other health checks
People with schizophrenia should be offered the same routine screening, health checks and vaccinations as other patients. This includes:
- women’s health care – contraception, cervical screening and breast cancer screening if aged over 45 years
- sexual health counselling and screening for sexually transmitted infections
- hepatitis B vaccination and treatment of hepatitis C
- interventions for alcohol and other substance use
- prostate and bowel screening for patients aged over 50 years
- annual influenza vaccination.
Conclusion
The transfer of care of a patient back into the community after an episode of acute psychosis is complex and fraught with pitfalls. The outcome is greatly enhanced if there is early, clear communication between the inpatient team and the GP. The GP has an important role in ensuring the patient has access to psychosocial supports and promoting medication concordance, which are key to reducing the risk of relapse. The GP’s role then extends to ensuring the patient’s physical health needs are also addressed. Ensuring this care gives the patient the best chance of remaining well. MT