Laser and energy-based devices. Use in common dermatological conditions

Laser and energy devices are increasingly being used for a growing number of dermatological indications from vascular and pigmented abnormalities to resurfacing and rejuvenation. Currently, there are no cohesive regulations surrounding the operation of laser and energy devices in Australia. It is therefore important that GPs advise patients to seek adequately trained providers for best outcomes.
- Lasers can be ablative or nonablative. Ablative lasers are destructive and are used for skin resurfacing. Nonablative lasers target pigment, such as vascular or pigmented lesions.
- Lasers typically emit a specific wavelength, and therefore specific devices are required to target particular molecules.
- Intense pulsed light (IPL) devices offer a spectrum of wavelength emission, thus a single device can be used to treat a range of problems.
- Lasers and energy devices can result in side effects including swelling, scarring and postinflammatory pigmentation changes.
- There is currently no consistent regulation for the qualifications and training of treatment providers across Australian states and territories.
- Most injuries from laser and energy devices are the result of inadequate knowledge and experience of the treatment provider. It is therefore important that GPs recommend or advise patients to seek treatment from adequately certified and experienced practitioners.
Lasers (light amplification by stimulated emission of radiation) were first used in dermatology in the early 1960s, when Leon Goldman described the effect of a laser beam on the skin for pigmentation.1 Since then, the applications of lasers and energy devices such as intense pulsed light (IPL) have expanded to include the treatment of:
- vascular lesions seen in rosacea, vascular malformations (port wine stains) and telangiectasias (dilated capillaries)
- pigmented lesions such as lentigines and birthmarks
- unwanted hair
- tattoo removal
- skin remodelling such as acne scarring and removal of benign skin tumours.
This article will review how lasers work, common laser and energy devices and their current uses.
How lasers work
Einstein first proposed in 1906 that light delivers its energy in discrete units called photons. He further proposed that photons, when stimulated, could stimulate identical photons from excited atoms.2 However, the practical application of his idea was not achieved until 1960 when the first laser was constructed by Theodore Maiman, using ruby as the medium.3 It thus took almost 50 years for Einstein’s theories to be proven in practice.
Lasers amplify light that has been stimulated via a specific medium to emit radiation, which can then be directed at a specific target (also called a chromophore). Electrical fields are used to excite electrons within a medium to a higher energy level. As the electrons decay, they each emit a photon. The photons are then directed at a chromophore, and pass on their energy. The frequency of the photons produced is determined by the medium used; therefore, selection of the medium determines the frequency of the radiation emitted.
A chromophore is a particle that absorbs radiation at a specific wavelength, depending on its absorption coefficient, and so different chromophores can be targeted by lasers using different mediums. Common chromophores targeted by dermatological lasers include haemoglobin (red), melanin (brown) and water. As seen in Figure 1,4,5 haemoglobin has an absorption coefficient curve with multiple absorption peaks at 418 nm, 524 nm and 577 nm in the visible range of the electromagnetic spectrum.4-6 The wavelength emitted by the laser not only determines the chromophore targeted, but also the depth of penetration from the skin surface. A greater depth is achieved by a longer wavelength.6
Common lasers and their current uses
Lasers can be categorised as ablative and nonablative. Ablative lasers destroy their target structures and have been used for skin resurfacing. Nonablative lasers target chromophores such as pigment and blood. Current lasers and their common uses are listed in the Table.7-10
Resurfacing and rejuvenation
There are two techniques for laser resurfacing. The first technique uses confluent consecutive shots or traditional horizontal laser resurfacing. The second technique is fractionated resurfacing, which uses a computer that allows the operator to generate a grid of the area to be treated with a suitable depth of laser energy and density of shots in the field. Both result in skin remodelling and rejuvenation; however, the first technique requires a longer healing time. When treating surgical scars, individual shots of varying size and frequency are used. In the treatment of acne scars, both techniques can be used for optimal outcomes.
Ablative lasers
Before the 1990s, dermabrasion was the treatment of choice for skin resurfacing.11 Subsequently, ablative laser resurfacing emerged as the gold standard for skin resurfacing procedures.6 Ablation involves the destruction of tissue, with neocollagenesis in the surrounding healing zone of thermal coagulation and results in skin tightening and smoothing. Ablative lasers were originally used for skin resurfacing, targeting the chromophore water.12 The first ablative laser was the carbon dioxide (10,600 nm) laser, originally developed in the 1980s as a cutting tool.13
A subsequent ablative laser is the erbium laser.12,14,15 The erbium laser has a shorter wavelength (2940 nm) and causes less deep destruction, resulting in less thermal damage and faster healing.11,13-15 It has a better recovery profile for swelling, discomfort and oedema compared with carbon dioxide lasers.14
Ablative devices were previously used in photoageing and wrinkle reduction treatments. Today, they are treatment options for facial resurfacing, severe acne scarring, skin tightening and removal of exophytic lesions such as warts, skin adnexal tumours, benign hamartomas and rhinophyma.12,13
Unfortunately, the side effects of treatment with ablative lasers can be more substantial compared with nonablative lasers. These include pain, swelling, bleeding, infection, scar formation, post inflammatory pigment changes and erythema.13,15
Fractionated lasers
The benefit of less downtime and faster recovery led to the development of fractionated nonablative lasers, followed by ablative fractionated lasers. Instead of treating the entire target area, or painting (e.g. the face), fractionated lasers perforate spots in a grid pattern and only laser a small percentage of the area to be treated. The process still stimulates neocollagenesis while preserving epithelial function. This results in less downtime and reduced complications in patients undergoing laser rejuvenation.11,13,15 Treatments with fractionated ablative lasers are also faster; however, the results are not as substantial as nonfractionated ablative lasers, so more treatments are required.6,11,13,14 The case study in Box 1 (Figure 2) illustrates the efficacy of fractionated ablative lasers in treating aggressive acne scars.
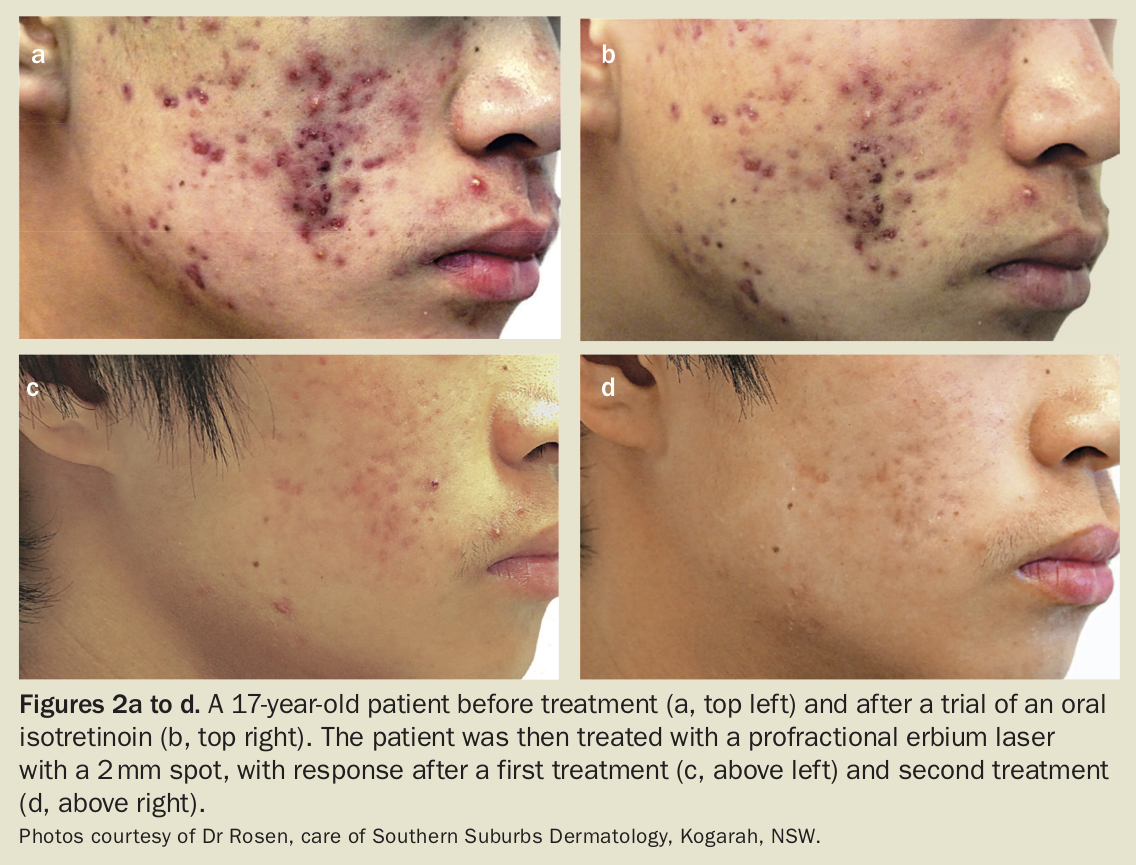{kind=link}
Treatment with fractionated nonablative lasers involves multiple small columns of heat (rather than destruction) directed at the skin, creating microscopic treatment zones (MTZs).15 The skin around each MTZ acts as a reservoir for healing. Fractionated nonablative lasers have the benefits of:11,14
- less pain
- faster treatment
- faster wound healing
- decreased risk of postinflammatory pigmentation changes
- decreased risk of persistent erythema
- lower risk of infection and scarring.
The first laser of this type was the fraxel laser.12,14
Vascular lesions
Nonablative lasers are used in the treatment of vascular lesions such as telangiectasias (Figure 3). These can be found in sun-damaged skin as well as conditions such as rosacea. Nonablative lasers can also treat vascular malformations, the commonest being port wine stains and haemangiomas.
The target chromophore (red) in vascular lesions is haemoglobin. The earliest lasers used for these lesions were continuous and released a constant stream of monochromatic light. This continuous energy dissipated as heat into surrounding tissue, not just in the target lesion (chromophore), resulting in damage to nontarget areas.
In 1973, the Nd:YAG (neodymium: yttrium-aluminium-garnet) laser was introduced for the treatment of superficial and deep vascular lesions. The Nd:YAG crystal is used as a medium for these solid-state lasers. The laser can be used to treat patients with deeper vascular lesions and spider veins in the legs up to 3 mm in size. However, it is less selective for haemoglobin, and so requires more energy. Combined with the longer pulse duration needed for larger vessels, the risk of nonspecific thermal side effects such as swelling, scarring and postinflammatory pigmentation are also more likely.16
Selective photothermolysis (proposed by Anderson and Parish in 1983) is the idea of thermal relaxation time.17 Thermal relaxation time is defined as the time required by an object to cool down to 50% of the initial temperature achieved. This allows us to selectively destroy tissues. In general, smaller targets have shorter thermal relaxation times and need to be matched with a shorter laser pulse delivery time. This concept is exploited with the nanosecond or picosecond lasers where the pulse duration is in the order of one billionth to one trillionth of a second, and is very useful for targeting minute tattoo granules.
Other lasers include the pulsed dye lasers that emit wavelengths of 585 nm and 595 nm.6,12,14 They are used to treat:12,16
- infants and children with capillary malformations
- infantile haemangiomas
- poikiloderma of Civatte
- facial telangiectasias
- rosacea
- superficial port wine stains.
The relatively shorter wavelength of pulsed dye lasers precludes their use for the treatment of deeper leg veins and deeper port wine stains.
Pigmentation
Melanin
Lasers that target melanin include potassium-titanyl-phosphate (KTP) lasers (532 nm), ruby lasers (694 nm), and alexandrite lasers (755 nm).6 KTP lasers were developed in the 1980s and are created by passing energy through a KTP crystal to produce light at a wavelength of 532 nm.18 This light is absorbed competitively by oxyhaemoglobin, melanin and tattoo pigment, making KTP lasers ideal for targeting both haemoglobin and melanin.16 The targeted melanin is in skin or hair, and tattoo ink. Often used with long pulses, the epidermis is cooled by a chilled sapphire or glass plate to prevent injury.12 Care is required in treating pigmented lesions due to the risk of missing a melanoma. Common conditions treated by these lasers include solar lentigines on the face and the back of hands (liver spots), melasma, pigmented actinic damage and pigmented birthmarks.6,16
Tattoo removal
Laser tattoo removal is an increasingly common cosmetic procedure. Different coloured tattoos require lasers of different wavelengths. Common media used in lasers that are ideal for tattoo removal include:16
- KTP at a wavelength of 532 nm to target yellow and red pigments
- ruby and alexandrite at wavelengths of 694 and 755 nm, respectively, for black, blue and green pigments
- Nd:YAG at a wavelength of 1064 nm for the removal of black and blue pigments.
These wavelengths are found in different lasers but the common feature of all tattoo-removing lasers is the ultrashort pulse duration, in the nanosecond to picosecond range, that selectively targets the minute tattoo granules. Blue and black pigments are the easiest to remove, followed by red; yellow and green pigments are the most difficult and often result in ‘ghosting’ or incomplete treatment.
In the 1980s, Q-switched (nanosecond) lasers were approved for use by the US Food and Drug Administration and have since become the gold standard for tattoo removal.12 They work by building up large amounts of energy behind an optical shutter. Once the shutter is opened, the energy is released and directed at the target tissue. This energy is absorbed by the target chromophore and converted to heat, causing expansion and contraction of the tissue and pigmented particles, resulting in their destruction. The destroyed pigment is removed as the cell membrane ruptures via the lymphatic system.16 Of note, most cosmetic inks contain iron or titanium oxide (such as some red lip tattoos).4 On irradiation, these may be reduced from ferric oxide to ferrous oxide, which is black and insoluble. This change may be permanent, and may require surgical or ablative laser removal.4
Hair removal
In 1996, the ruby laser was the first laser formally studied for hair removal.19 The target in hair removal is primarily the melanocytes in the bulge region and target melanin absorbs wavelengths between 600 and 1000 nm.16 Long-pulsed lasers including long-pulsed ruby, alexandrite, diode and Nd:YAG lasers are used for hair removal to cause damage to the whole follicular unit.12,16 The laser used depends on the skin phototype, with lighter skin phototypes (I-III) responding to alexandrite (755 nm) and diode (800 nm) lasers, whereas darker phototypes (IV-VI) respond better to the Nd:YAG (1064 nm) laser.6,16 Fairer hair colours (red, grey, white) are less effectively treated.20 The laser is compressed to the skin to allow for deeper delivery of the pulse and the epidermis is cooled with a sapphire plate on the laser handpiece for protection.12,16 The IPL device (discussed further below) is also used for hair removal and is regarded as one of the most effective methods of hair removal.20
Intense pulsed light devices and their uses
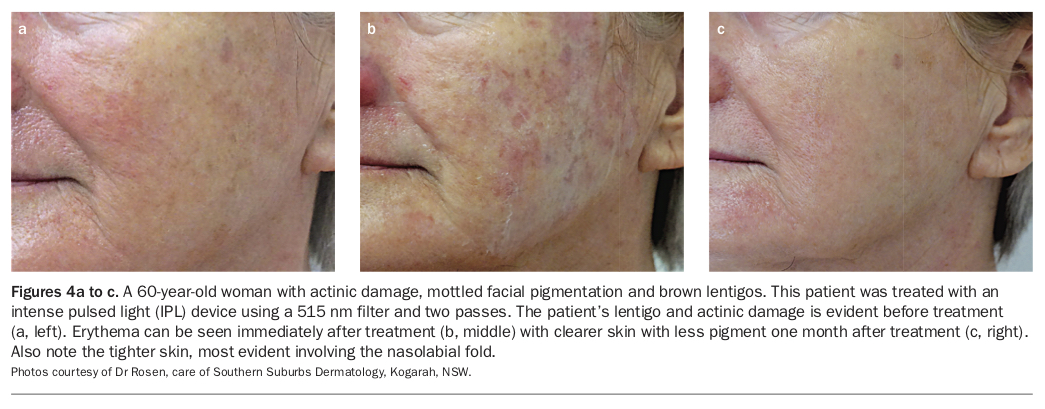
IPL differs from lasers because it produces polychromatic, noncoherent light that covers a broad spectrum of wavelengths.12,15 A typical wavelength range is from 400 to 1200 nm.6 Filters are used to select parts of the spectrum best suited to the target lesion6,12 (e.g. 515 nm for treating pigment lesions [Figure 4], 560 nm for treating vessels [Figure 5] and 540 nm for hair removal). The advantage of IPL is in its ability to target melanin as well as haemoglobin.14 It was initially introduced to treat vascular lesions and is also used to treat telangiectasias in active disease (Figure 6), telangiectatic rosacea (Box 2; Figure 7), melasma, lentigo and actinic damage, and hair removal.12 Modern IPL devices have improved outcomes as a result of improved wavelength filtration, shorter pulse durations and an enhanced ability to adjust epidermal temperatures.20 This results in less downtime and faster results.
{kind=link}
IPL has also been used in conjunction with aminolevulinic acid in photo-dynamic rejuvenation.14,21 This treatment combination is reported to remove actinic keratosis, erythema, dyspigmentation, fine rhytides, and skin texture.14,18 The most common side effect seen in IPL treatment is a routinely occurring transient erythema.22 It is worth noting that IPL devices are potent therapeutic devices and can result in the same side effects as lasers, including swelling, scarring and postinflammatory pigmentation changes.
Treatment providers
Regulation surrounding the provision of laser and IPL treatment is inconsistent across Australian states and territories: only Western Australia requires the operator of a laser to be a medical practitioner; only Tasmania has licensing requirements for IPL; the other states and territories have no regulation.23,24 In 2015, there were an estimated 4000 injuries related to the use of lasers and energy based devices, including hospital admissions for critical care for burns.25 Most of these complications were because of inadequate training for the treatment provided.25
Currently, the Australian Radiation Protection and Nuclear Safety Agency is developing advice for cosmetic treatments and beauty therapy. The need for such advice is clear, with reports of inappropriate treatment leading to missed diagnoses of melanoma, injuries relating to incorrectly applied treatments including burns and scarring (Figure 8), and implications for medical indemnity.23,24 GPs should advise patients to decide carefully where they wish to undertake treatment and ensure that providers are certified and experienced, and that there is a doctor on hand should any problems occur.
Conclusion
Lasers and laser-like energy devices are used more frequently for an ever-increasing number of indications. The evolution of laser devices has a seen a consumer- driven shift from ablative laser to nonablative laser use, where possible. Laser treatment for vascular and pigment lesions are less prevalent because IPL can sufficiently treat these problems.
All energy devices are powerful and can cause damage. Although there have been vast improvements in the quality of lasers and IPL devices, injuries result largely from provider inexperience and lack of training. In the absence of national regulations for the provision of laser and energy devices, we will continue to see complications and injuries as these types of treatments continue to increase. GPs can play an important role in advising patients on the treatment options available and guiding them to the best qualified practitioner to prevent unwanted side effects and injuries. MT