Managing obesity: focus on lifestyle approaches

Dr Gibson is a Research Fellow In the Boden Collaboration, Charles Perkins Centre, The University of Sydney.
Dr Franklin is a Senior Dietitian at Metabolism and Obesity Services, Royal Prince Alfred Hospital.
Dr Sim is a Senior Dietitian and Manager of Obesity Prevention and Management, Sydney Local Health District.
Dr Partridge is a Dietitian at the Westmead Applied Research Centre, The University of Sydney.
Professor Caterson is the Boden Professor of Human Nutrition and Director of the Boden Collaboration, The University of Sydney, Sydney, NSW.
Obesity

Most of us eat several times a day, most days of our lives. In our modern environment, food is plentiful, energy-dense, highly visible, convenient and a major part of our social lives. In contrast, being physically active is a choice and not a necessity for survival. It is therefore not surprising that it is hard for people to lose weight and keep that weight off.
- The majority of patients who have obesity are interested and motivated to lose weight; they want their healthcare practitioner to discuss it with them.
- The most important factor determining the success of any weight loss attempt is the ability to adhere in the long term to the new lifestyle changes.
- A quick and practical approach to offering dietary advice is to think quality (eating more for less kilojoules by choosing healthier whole-food options) and quantity (applying caution with portions).
- Simply telling patients they need to eat less and move more is unlikely to be effective. They need help to do this – it takes ‘skill power’ not just ‘will power’ to lose weight.
- Taking a detailed weight history and representing this visually is a useful starting point for providing individualised advice that is more likely to resonate with the patient.
Obesity is the result of a long-term positive energy balance and although an energy deficit must be created to achieve weight loss, attributing obesity to eating too much and not exercising enough is an oversimplification. It is evident in the real world and from scientific studies that people struggle to lose weight and keep it off. Unfortunately this failure is usually attributed to the individual, with the person often considered weak-willed, lazy and even stupid.
The factors contributing to obesity are complex due to an interaction between varying genetic and biological tendencies, and to environmental, cultural and socioeconomic drivers of weight gain. Factors may act alone or in combination to modulate energy intake and/or expenditure and hence determine the likelihood of an individual developing obesity. The current ‘obesogenic’ environment is propelling the epidemic by providing an unfavourable situation that overwhelms the sophisticated regulatory systems of the body controlling appetite and maintaining energy balance. In today’s world it can be argued that weight gain is a natural response for humans endowed with an ‘ancient metabolism’. Consuming excess energy was important in our evolutionary past to last us through the times of shortage, now it is a health hazard.
The primary care setting is the obvious choice for tackling the obesity epidemic because of the long-term nature of the clinician–patient relationship. However, due to a range of factors, including lack of time, perception the patient is not interested or motivated, that there are more important health issues to discuss, and the social and personal prejudices about the individual with obesity, many GPs find it challenging or feel ill equipped to tackle the problem.1
This article aims to help practitioners start a conversation with their patients regarding weight loss and better health using simple practical suggestions. It is in line with the current National Health and Medical Research Council (NHMRC) guidelines that recommend lifestyle change as the cornerstone of all interventions. The reader is also referred to the NHMRC Clinical Practice Guidelines for Managing Overweight and Obesity in Adults, Adolescents and Children for more information.2
Diagnosing obesity
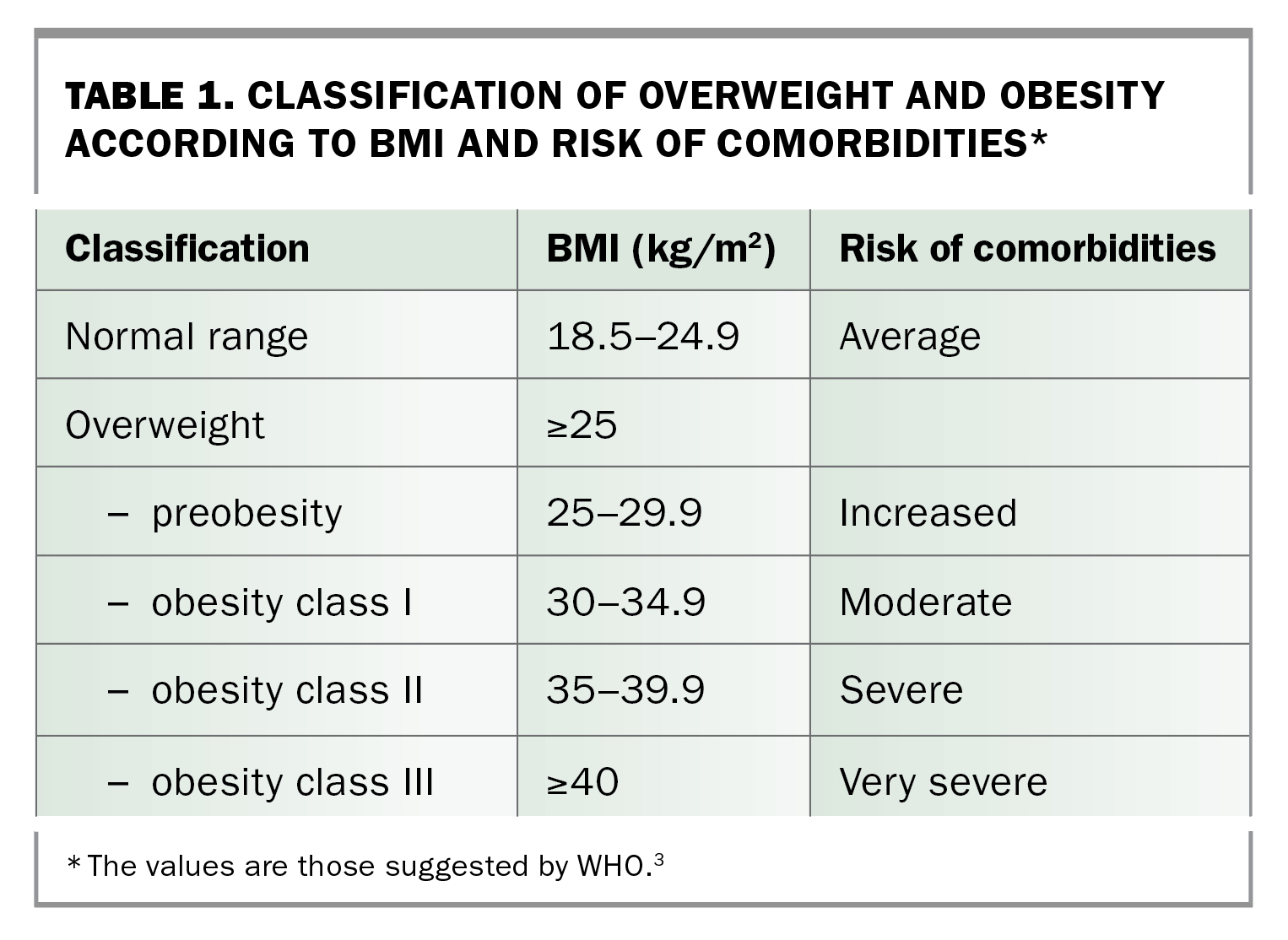
Obesity is defined as an abnormal or excessive accumulation of adipose tissue in the body, resulting in adverse effects on the health and wellbeing of the individual.3 In clinical practice, a useful measure of obesity is the body mass index (BMI). It gives a reasonable approximation of adiposity and indicator of health. BMI is derived by dividing an individual’s weight in kilograms by height in meters squared (kg/m2). Adults with a BMI between 25 and 29.9 kg/m2 are categorised as having overweight or preobesity, and those with a BMI of 30 kg/m2 or over are categorised as having obesity (Table 1).3 The BMI cut-off points are, however, not applicable to all ethnic groups, people at extremes of age and those with excess muscularity and height.
{kind=link}
Diagnosing someone as having obesity can have psychological consequences. The word obesity is loaded with stigma, blame and shame. Weight stigma arises from the misunderstanding of obesity drivers. Weight stigma can trigger physiological and behavioural changes linked to poor metabolic health, increased weight gain and exercise avoidance.4-6 Using compassionate terms and discussing weight from a health perspective can help alleviate these negative effects. Using words like ‘being well above a healthy weight’ is preferred rather than ‘extremely obese’ or ‘fat’. However, not discussing weight has equally detrimental outcomes.
Obesity as a disease and risk factor
Obesity is regarded as a disease in its own right. It is also a risk factor for a large number of chronic, metabolic and mechanically induced disorders, the risk of which increases on a continuum with increasing adiposity. It is not only the amount but also the distribution of adipose tissue that underlies the health risks and diseases associated with obesity. Waist circumference, a surrogate marker of visceral fat, has been shown to be a more sensitive measure of long-term health risks (Table 2).3 Waist circumference (really an abdominal circumference at a defined level) should be measured mid-way between the lowest rib and the upper border of the iliac crest. This position can sometimes be difficult to find in an individual with obesity. Always look from the side, make sure the tape measure is level and have it directly on the skin to get the most accurate and repeatable results.
{kind=link}
Goals of obesity management
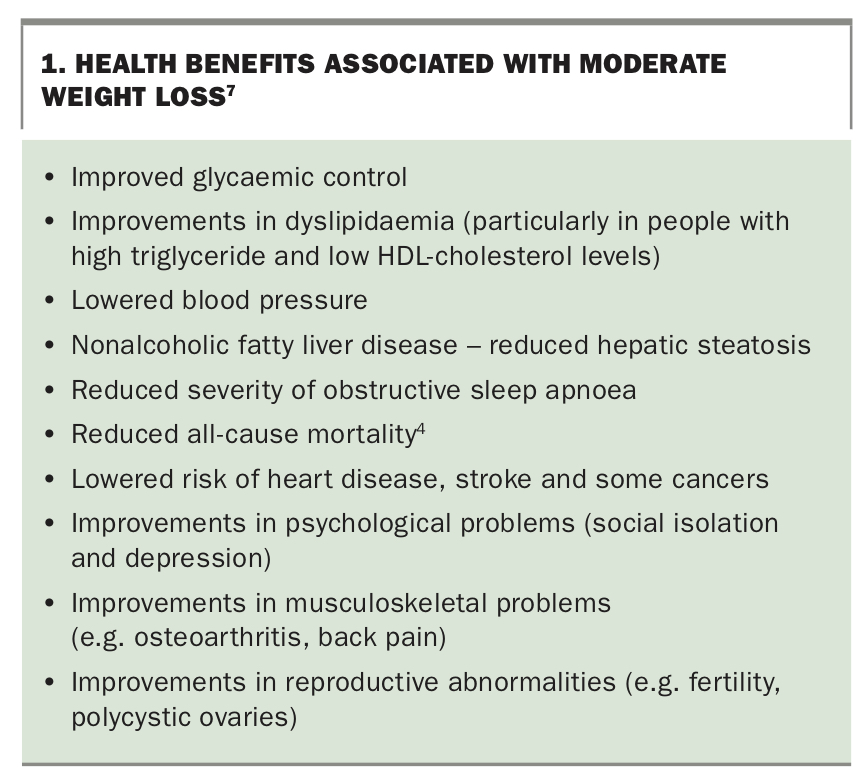
Any obesity management plan should be structured to include both an active weight loss phase and a weight maintenance phase. Lifestyle modification – dietary change, alterations in physical activity and behaviour modification – should be the main therapeutic approaches in the management of obesity. Effective weight management is defined as a weight loss of 5 to 10% of body weight that is maintained for at least two years. Health benefits associated with moderate weight loss are outlined in Box 1.7
{kind=link}
Not all patients will be ready or willing to lose weight despite their weight putting them at risk of medical disorders. However, a recent international study investigating perceptions, attitudes, behaviours and barriers to effective care in adults with obesity and healthcare professionals identified a dichotomy between patients and healthcare professionals.1 More than two-thirds (65%) of patients wanted their healthcare professional to talk about their weight. However, on average, they had to wait six years between starting to struggle with their weight and having such a conversation. The top reason (71%) given by healthcare providers why weight was not discussed was the perception that the patient was not interested in losing weight. In contrast, only 7% of patients reported not being interested. Most patients are interested and want their healthcare professional to discuss their weight, and the sooner this conversation takes place, the better.
Dietary approaches
Healthy eating, not dieting
The word ‘diet’ comes from the Latin word ‘diaeta’ meaning ‘way of life’. This is in sharp contrast to the way the word is used in today’s society, where it carries connotations of short-term adherence and negative associations with restrictive eating. As such, it is better to prescribe an ‘healthy eating plan’ as opposed to a ‘diet’. If patients embrace an ‘eating for health’ approach to dietary change and do not just view it as a way to lose weight then they may be less likely to ‘give up’ on their diet and start again the next day or week.
Any dietary advice for weight loss should not compromise the person’s micronutrient nutritional status. The types of foods that patients should be eating to lose weight are the same as those that are recommended for the general healthy population. The recommended number of serves in the Australian Guide to Healthy Eating are also based on those with the lowest energy requirements within each age and gender group (i.e. smaller and less active); following the guidelines should inevitably result in an energy deficit for larger persons. These recommendations, developed by the NHMRC, were released in 2015 as part of Eat For Health program (www.eatforhealth.gov.au).
No one-size-fits-all approach
A negative energy balance is essential for weight loss; how such an energy deficit is achieved is dependent on the individual. Weight loss is dynamic and needs to be reviewed on a regular basis. There are dynamic physiological adaptations that manifest with weight loss; namely a reduced resting metabolic rate, increased appetite and decreased energy cost of physical activity.8 Dynamic models that allow prediction of how changes of diet or physical activity will translate into weight changes over time have been developed and are available online (http://bwsimulator.niddk.nih.gov and www.pbrc.edu/research and faculty/ wcalculators/weight-loss-predictor).8,9 These models may be useful in clinical practice to establish a target energy intake for a patient based on the desired weight loss outcome and duration. They can also provide guidance on the energy intake necessary to maintain the new weight once reached.
Temporary changes equal temporary weight loss
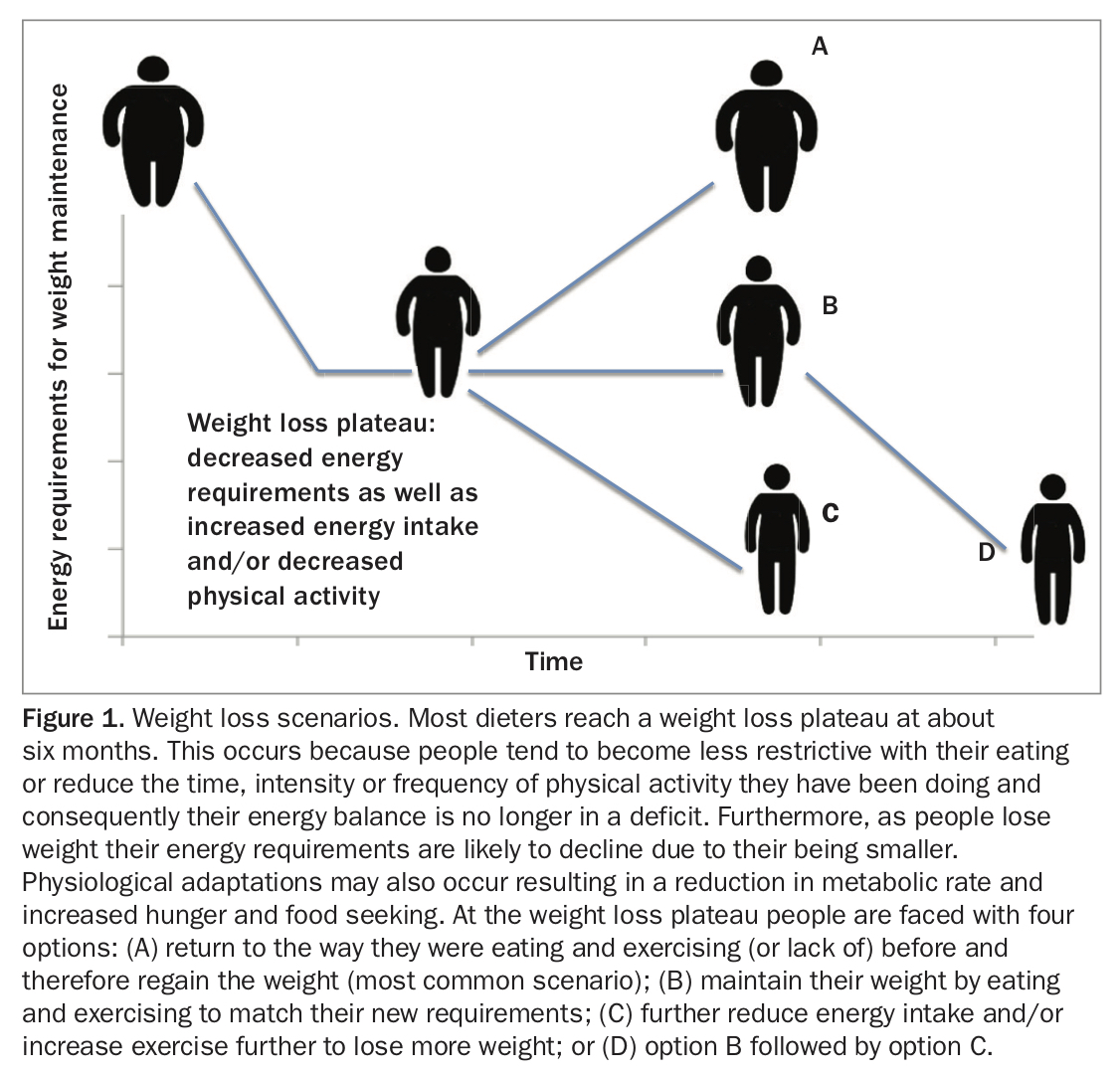
Most people who diet reach a weight loss plateau at about six months and this occurs for several reasons. First, people may become less restrictive with their eating, or reduce the time, intensity or frequency of their physical activity and consequently their energy balance is no longer in a deficit. Second, as people lose weight their energy requirements decline. Third, physiological adaptations may occur resulting in a reduction in metabolic rate and increased hunger and food seeking.10-13 At the weight loss plateau people are faced with the following four options (Figure 1):
{kind=link}
- return to the way they were eating and exercising (or lack of) before weight loss and therefore regain the weight (the most common scenario)
- maintain their weight by eating and exercising to match their new requirements
- further reduce energy intake and/or increase exercise further to lose more weight
- period of weight maintenance followed by further weight loss (i.e. second option followed by the third).
This introduces several common misconceptions among individuals who have lost weight or are losing weight. First, that they will be able to maintain a lower weight as easily as when they were at a higher weight. Second, that weight plateauing is bad and there is no point in trying if not achieving weight loss. And third, that if you just have a strong enough will power you will be able to decrease your energy intake further and lose more weight.
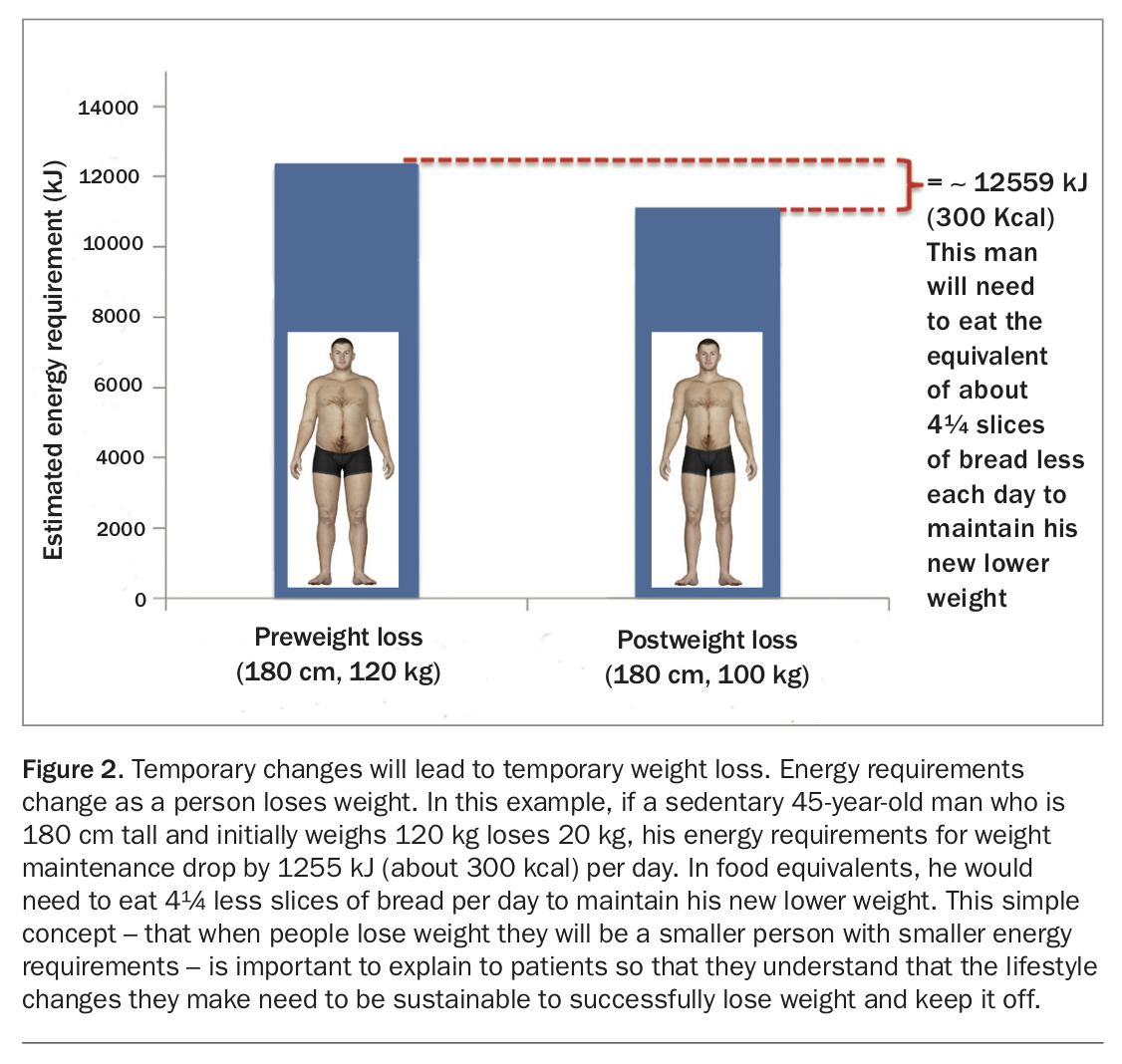
Patients often think that because they were able to maintain their original weight with little or no effort, then this should also be the case after weight loss. To maintain their new lower weight they need to be eating less or doing more exercise than they were at their original weight. This is why the most important factor determining the success of any weight loss attempt is the ability to maintain long-term adherence to new lifestyle changes. Temporary changes will lead to temporary weight loss; if the predisposing factors remain, so too does the propensity for weight regain (Figure 2).14 Therefore patients should be encouraged to make lifestyle changes that are sustainable.
{kind=link}
Patients often become frustrated and give up on lifestyle changes when their weight starts to plateau. The WHO recognises that no weight gain is a good outcome in weight loss interventions, particularly in patients who have previously been gaining weight. Helping patients identify benefits of their new lower weight or of not gaining weight may help them to feel less frustrated when their weight plateaus. Many dieters believe that if they restrict their intake further then they will lose weight no matter what their bodies are trying to do. The physiological adaptations to losing weight will make people feel more hungry and seek higher energy food more often.10-13 Therefore this can be a good time to introduce another strategy such as meal replacement products in particularly very low energy diets (VLED), which can control hunger while reducing weight, use of pharmacotherapy or bariatric surgery.15
The National Weight Control Registry in the USA (www.nwcr.ws), which is following more than 10,000 people who had lost 13.6 kg or more using any method and kept it off for at least a year, has shown that successful people had the following characteristics: they ate a low-energy and low-fat diet; consistently self-monitored their weight; ate breakfast regularly; engaged in 60 minutes of physical activity each day; watched very little television (screen time) and had minimal variation to diet on weekends or when on holidays.16
A practical approach
There are numerous dietary approaches for weight management. A simple starting point can be discussing vegetable consumption and discretionary food intake.
Increase vegetable consumption
Only 8% of Australian adults meet the guidelines of serves of vegetables per day. This is even less (5%) for both vegetables and fruit.17 A possible goal is to encourage patients to ensure that half of what they eat is vegetables for at least two meals each day.
Decrease discretionary food items: discuss alcohol and ultra-processed food intake
Discretionary foods make up more than one-third (36%) of Australian adults’ total daily intake. Of this, for adults aged 51 to 70 years, alcoholic beverages account for over one-fifth (22%) of discretionary food intake.18
Ultra-processed foods are those that undergo a multitude of processes including many that could not be recreated in the home. They have been found to have a detrimental effect on health particularly weight regulation. It has been reported, eating ad libitum only ultra-processed food for two weeks can lead to a 0.9 kilogram increase compared with a 0.9 kg weight loss after eating unprocessed food under the same circumstances.19
A possible goal is to encourage patients to swap discretionary foods for other (unprocessed) foods and/or minimise the amount consumed. It is not essential to eliminate a particular food.
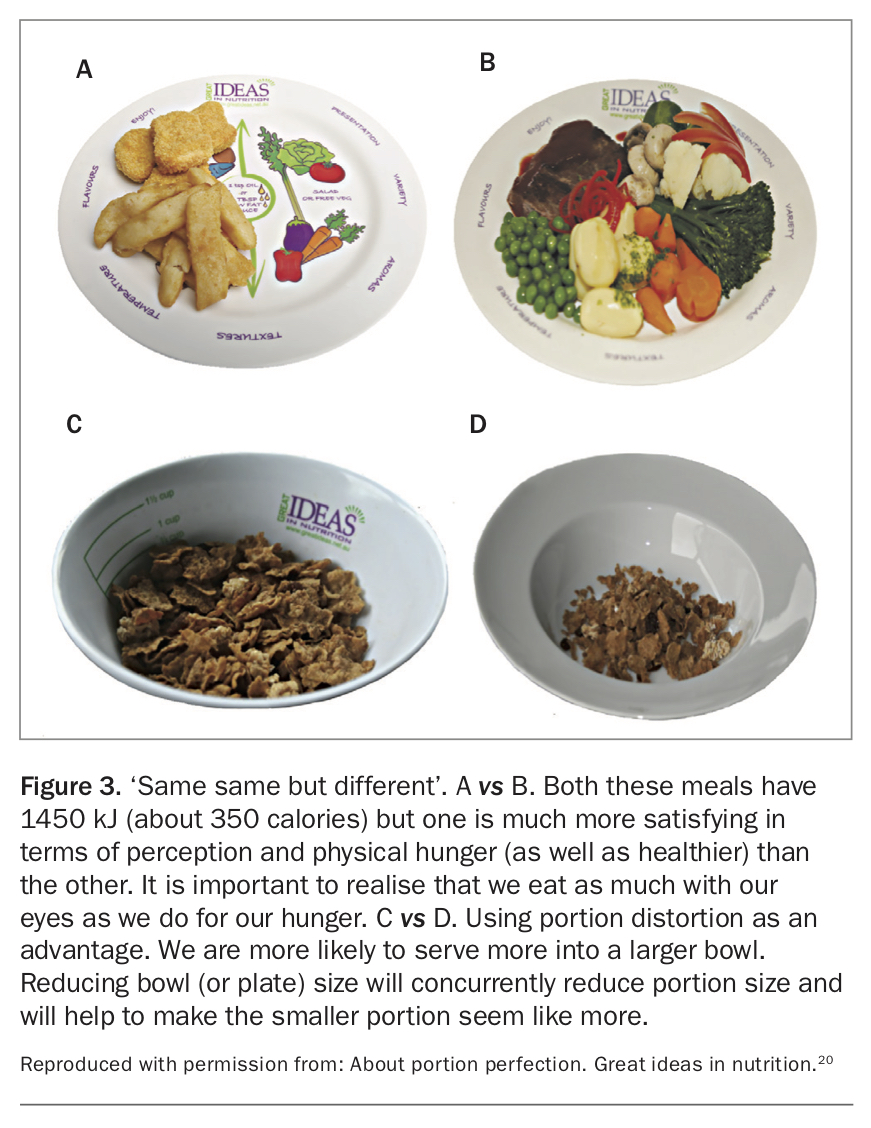
Quality – eating more for less
Simply put, when losing weight a ‘kilojoule is a kilojoule’. However, a person would have to eat a lot more carrots than potato chips to consume 1000 kJ. An important aspect for sustainability of an eating plan is feeling satisfied. A useful approach is to encourage patients to think about kilojoules as if it were money – that is, to feel satisfied on an ‘energy budget’ they need to ‘spend’ their kilojoules wisely. By choosing healthier, less energy-dense foods such as vegetables, fruit, wholegrains, reduced fat dairy products and lean protein foods, patients can eat more for less kilojoules (Figure 3).20 This will also help to establish long-term healthy eating habits for optimal health.
{kind=link}
Quantity – portion caution
Many patients may already have good nutritional knowledge and be eating a reasonably healthy diet. It is still possible to overeat, even on nutritious foods. The fact that larger portions have more energy may seem intuitive; however, most people tend to eat whatever they are served. In today’s society we have become accustomed to larger portions. To accommodate our larger portions, our bowls, plates and cups have also increased in size. A ‘normal’ portion is often much more than we actually need to eat.
Environmental factors impacting portion sizes are ubiquitous and can strongly influence the amount we eat or drink.21 Larger packaging and serve ware have been shown to unknowingly increase the amount served.22,23 As most people eat more when there is more in front of them, overserving leads to overeating. It is also not simply a matter of telling people that the bias exist, even nutrition experts – after being lectured extensively on the topic – still served themselves 56.8% more ice cream when given a larger bowl and larger spoon compared with those who were given a smaller bowl and smaller spoon.24 Reducing the size of serve ware will concurrently reduce portion size without necessitating vigilance and portion distortion can be used as an advantage (Figure 3).20
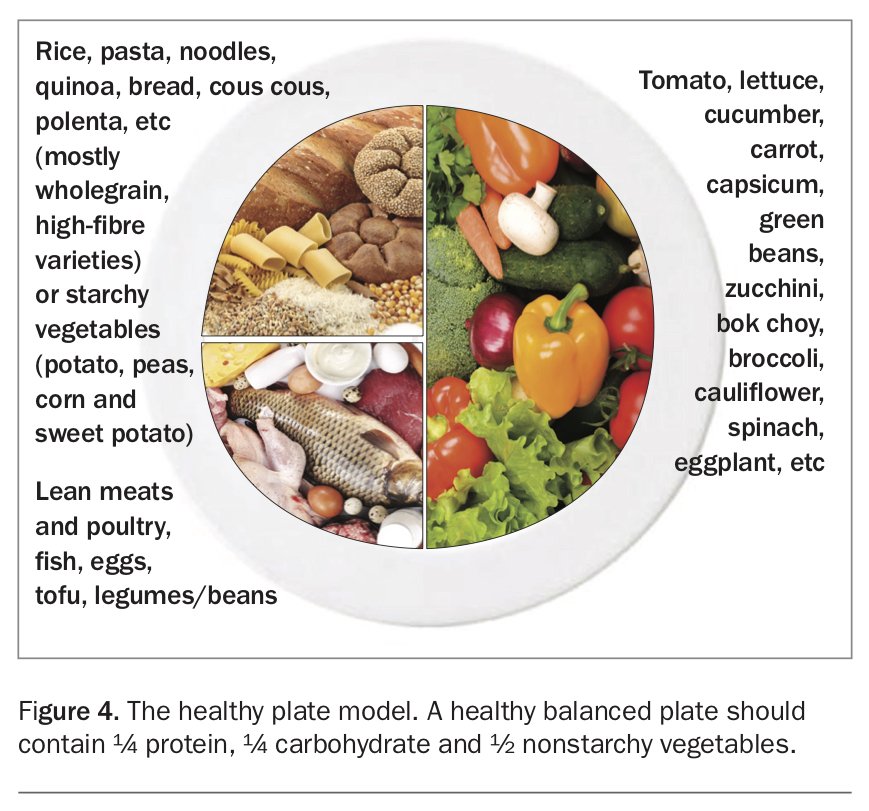
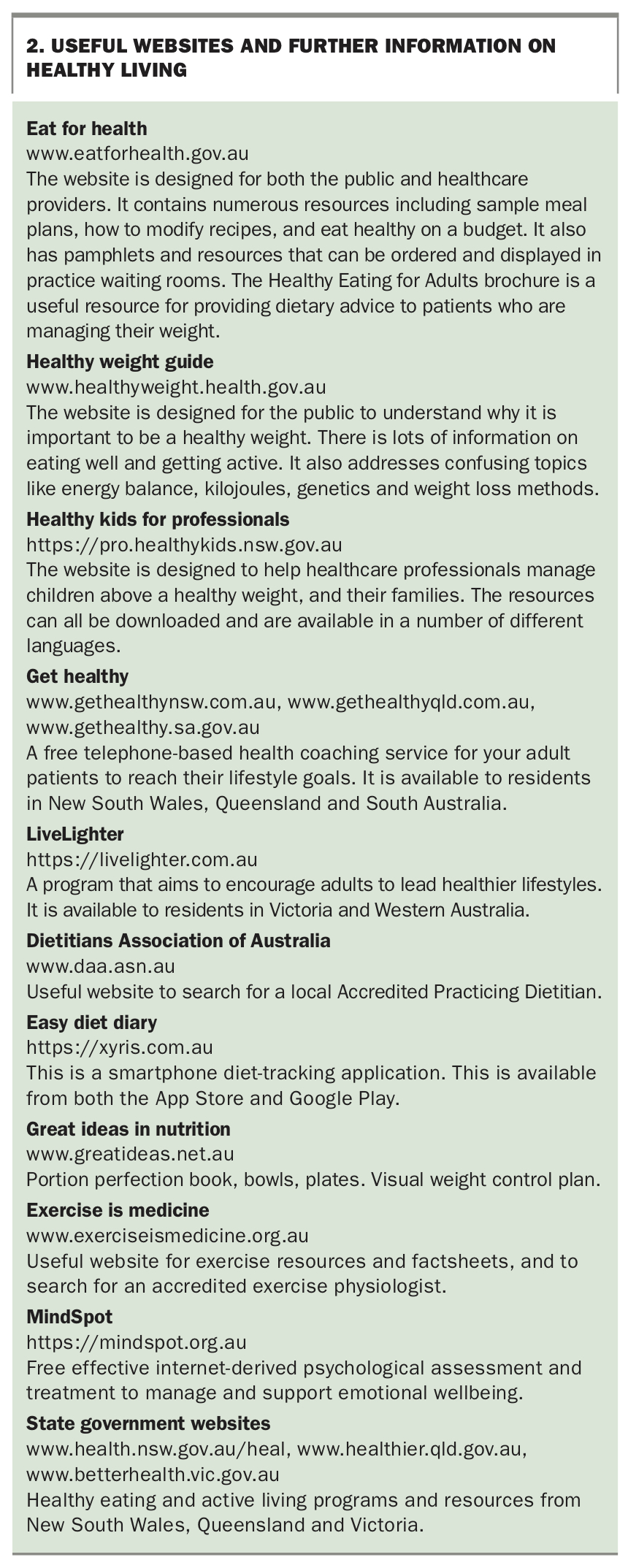
A healthy plate model using the Healthy Eating for Adults brochure can be a simple way to educate patients on appropriate types and proportions of foods to consume for main meals (see Figure 4 and Box 2 listing useful websites and online resources).
{kind=link}
{kind=link}
Physical activity
Patients should be encouraged to increase their daily physical activity. The goal is to achieve at least 150 to 300 minutes of moderate or 75 to 150 minutes of vigorous activity per week. Moderate activity is to a level that increases breath and heart rate above normal. Vigorous activity leads to harder breathing (i.e. puffing and panting) and substantially raised heart rate, depending on the level of fitness. People should find the activity somewhat hard or harder. It is also important to encourage patients to reduce their ‘inactivity’, in particular their sitting time, and to stand more. Research suggests that sedentary behaviour that is detrimental to a person is not just the lack of physical activity but also prolonged uninterrupted periods of sedentary time, which is associated with metabolic risk variables (including waist circumference, BMI, triglyceride level and two-hour plasma glucose level).25,26 Pedometers or smart phone applications may be useful to self-monitor activity and to set daily or weekly targets; these can be gradually increased. Patients should aim for 10,000 to 14,000 steps (depending on stride length) per day (or 10 km). Any increase in physical activity is good and should be encouraged, even if targets are not met immediately. A dose response occurs with greater activity, leading to increased health benefits, regardless of whether weight loss is achieved.27,28 Hydrotherapy and/or aqua aerobics are useful alternatives for people with osteoarthritis or those who experience pain on exercise. Referring the patient to an exercise physiologist may also be helpful. The most important factor is finding an activity that the patient enjoys and is likely to maintain in the longer term.
Behaviour change – skill power not just will power
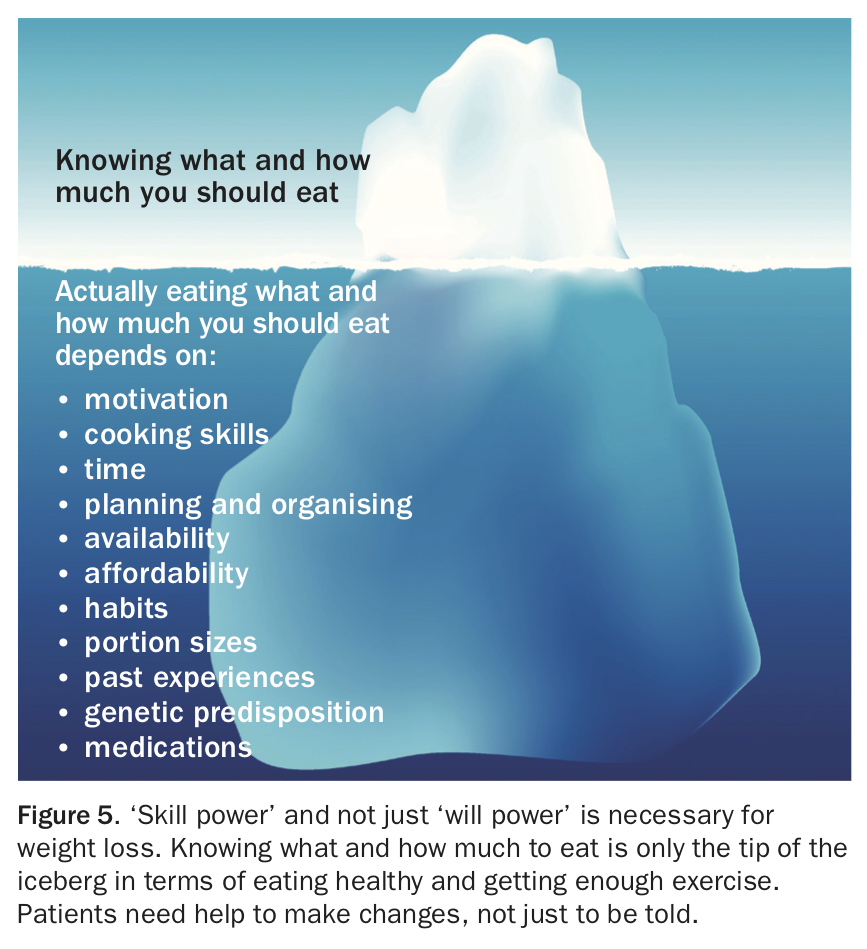
Most people who are of an unhealthy weight do not want to be unhealthy or have excess weight.1 The problem is that we live in an environment in which it is extremely difficult to not gain weight. Knowing what and how much to eat, and being motivated to do so is only the tip of the iceberg (Figure 5). When people commit to losing weight they often assume that it is simply a matter of deciding to do so. In reality, life (work, family commitments, etc) do not stop when people are losing weight; there are many barriers that can get in the way. This is why simply telling patients they need to ‘eat less and move more’ is unlikely to result in successful weight loss. They need help to do it by, for example, identifying barriers before they arise and devising strategies and providing support to overcome or minimise them.
{kind=link}
Self-monitoring by recording food intake and/or exercise can help patients to gain insight into their own eating habits and provide a useful starting point to developing a plan of action. Numerous smart phone applications have been developed for this purpose and can be a useful alternative to traditional pen and paper recording. The key to successful behaviour change is frequent contact and support to ensure that lifestyle changes are sustained. Sometimes simple interventions may not be enough and a referral to other healthcare professionals (including psychologists, dietitians and exercise physiologists) may be required for a more intensive intervention or approach. Ongoing involvement of the clinician in the patient’s efforts to initiate and maintain a healthy weight and lifestyle is integral.
Putting it into practice
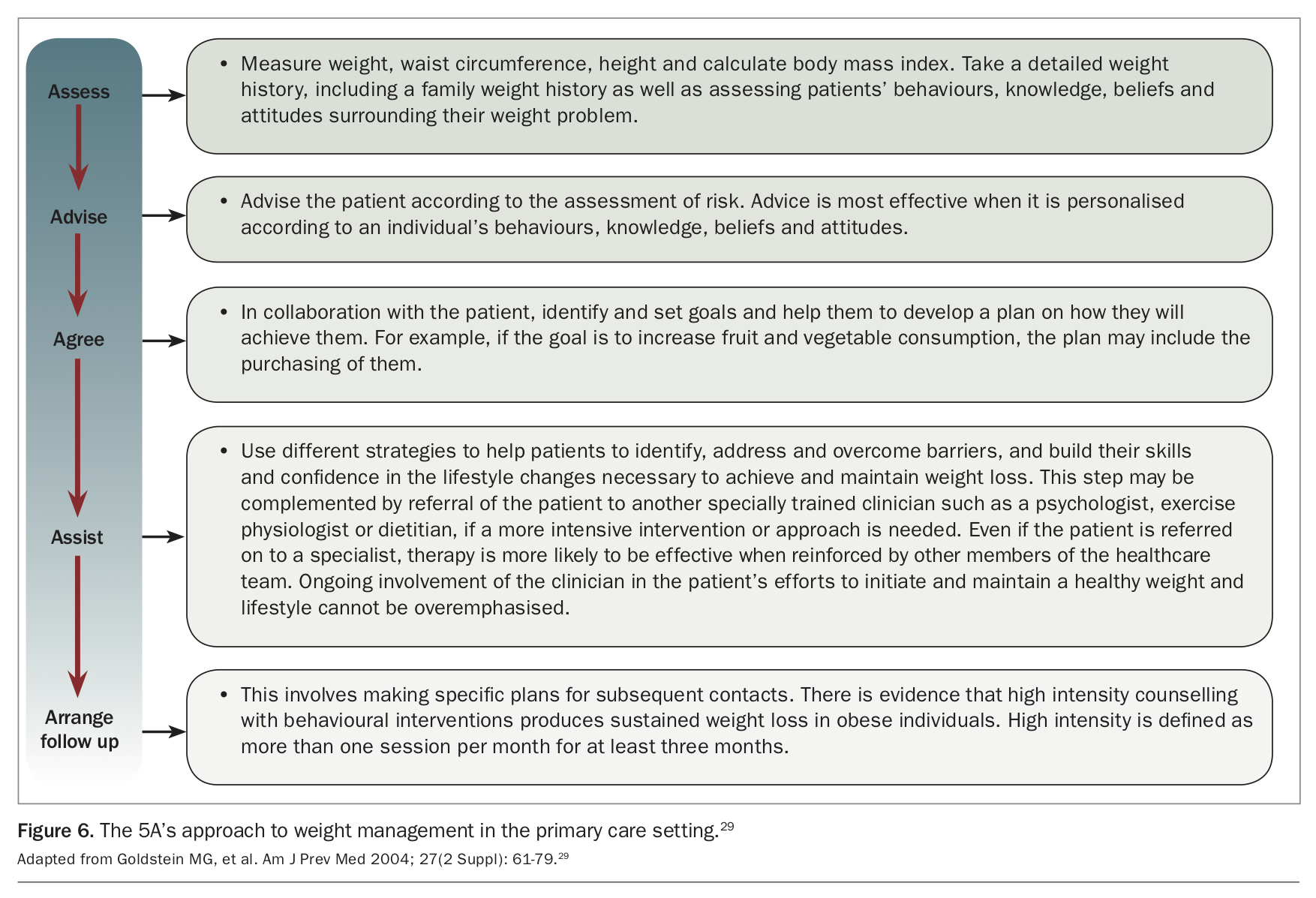
Using the 5A’s approach
The 5A’s approach (Assess, Advise, Agree, Assist, Arrange) can be used as a guide to structure weight management counselling. It does not necessarily have to be done all in the one session (Figure 6).29 This approach is adopted in the NHMRC guidelines.2
{kind=link}
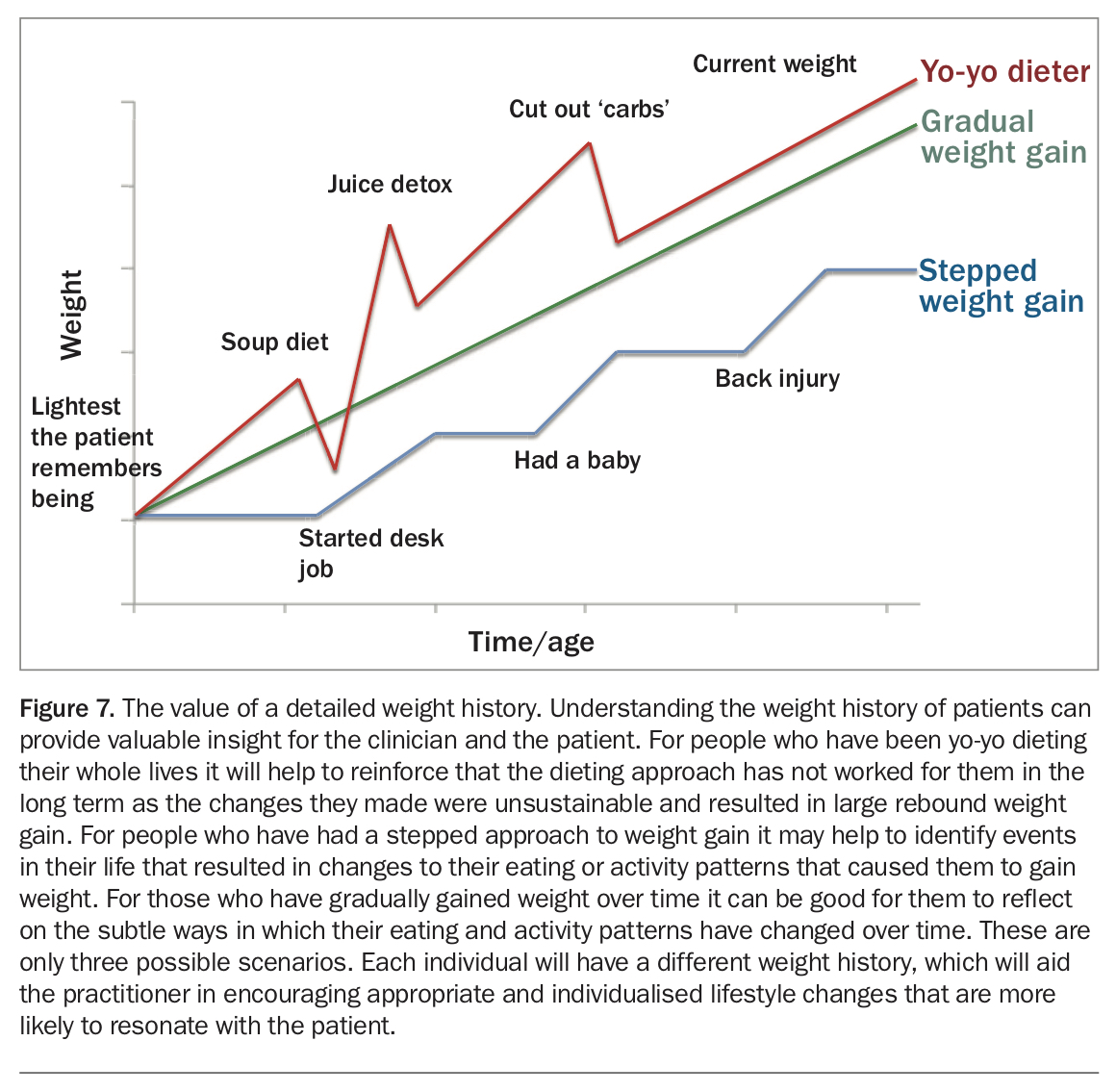
A starting point
A useful starting activity when commencing any weight management program is to take a detailed weight history. If possible, represent it visually back to the patient, as shown in Figure 7. Discussing or displaying a patient’s weight history will help them to think about, understand and identify the reasons for their weight gain or weight regain over time. It will also aid the practitioner in encouraging appropriate and individualised lifestyle changes that will resonate with the patient.
{kind=link}
Conclusion
Obesity has extensive medical implications. Most patients do want to lose weight and are motivated to do so. Identifying individual and personal reasons will aid motivation. Focusing on healthy eating, controlled portion sizes, increased movement and reduced sedentary time will all help with weight loss. Obtaining an extensive weight history will make treatment easier and will help patients understand their own weight status. MT