Is weight loss the best treatment for type 2 diabetes?


Weight control
Diabetes type 2
Obesity is the main driver of type 2 diabetes and weight loss has been shown to improve blood glucose levels. This article describes the author’s own approach to weight loss in people with diabetes – the use of a very low energy diet followed by long-term weight maintenance (lifestyle changes and appetite-suppressing medication).
- Obesity is the main driver of type 2 diabetes, commonly interacting with chronological ageing and ethnic susceptibility.
- Weight loss improves blood glucose levels in people with diabetes, and those with a short history of the condition may go into temporary remission.
- Weight loss is not maintained long term in most individuals because body weight is vigorously defended.
- Very low energy diets (VLEDs) allow rapid weight loss with maintenance of micronutrient levels.
- Appetite-suppressing medication may be necessary as well as lifestyle changes after losing weight medically (VLED, bariatric surgery).
- Many people can cease some or all diabetes medications after substantial weight loss.
Australia is in the midst of an obesity epidemic that is driving an epidemic of type 2 diabetes. This is already a major health problem in developed Western countries but its greatest impact will be in Asian countries, due to the greater risk of developing type 2 diabetes in Asian populations.1
How does obesity lead to diabetes? When there is excess fat in the body some of it is deposited ectopically causing damage. Excess fat in muscle and adipose tissue leads to insulin resistance,2 and excess fat ingestion stimulates gluconeogenesis and is a major cause of hepatic insulin resistance.3 Finally, saturated fatty acids are a major toxin to beta cells.4
It follows that losing weight both reverses insulin resistance and improves insulin secretion. Several studies have shown that substantial weight loss, either with a very low energy diet (VLED) or bariatric surgery, can greatly improve blood glucose levels.5,6 This is especially true if weight loss is achieved when diabetes is first diagnosed.
Weight loss with lifestyle advice
The fact that weight loss is the best treatment for people with type 2 diabetes has been acknowledged in most national and international guidelines in which weight loss is advised as first-line therapy. When people are first diagnosed with type 2 diabetes, they are usually given advice to change their diet and to increase their level of physical activity. However, multiple studies have demonstrated that lifestyle advice leads to only modest weight loss of between 3 and 8 kg, which is not maintained for any length of time by most people.7 Blood glucose levels initially decrease with this approach but within a short time some or all of the weight lost is regained and the glucose levels increase again. At this point, pharmacotherapy (usually metformin) is initiated. The natural history of type 2 diabetes is that eventually the single agent no longer controls the patient’s blood glucose level and a second-line treatment such as a sulfonylurea or a dipeptidyl peptidase-4 inhibitor is prescribed. With time, a third-line drug such as a sodium-glucose cotransporter-2 inhibitor, glucagon-like peptide-1 analogue or insulin is added.
Why is the weight loss with lifestyle advice modest and why do most people regain weight? The reason is that body weight is strongly defended. To fully appreciate what this means it is necessary to consider the physiological regulation of body weight. Weight is controlled by the hypothalamus. There are two types of neurons in the arcuate nucleus of the hypothalamus. One type expresses both neuropeptide Y (NPY) and agouti-related protein (AgRP), both of which powerfully stimulate hunger. The other type expresses pro-opiomelanocortin (POMC; from which alpha melanocyte-stimulating hormone [αMSH] is cleaved) and cocaine- and amphetamine-regulated transcript (CART); both αMSH and CART powerfully inhibit hunger. At any particular time, it is the activity of these neurons that determines whether we want to eat or not.
Eleven circulating hormones produced by the gut, the pancreas and adipocytes influence the activity of these particular neurons and therefore regulate hunger (Table 1). Only two of these hormones stimulate hunger, with the remaining nine inhibiting it.
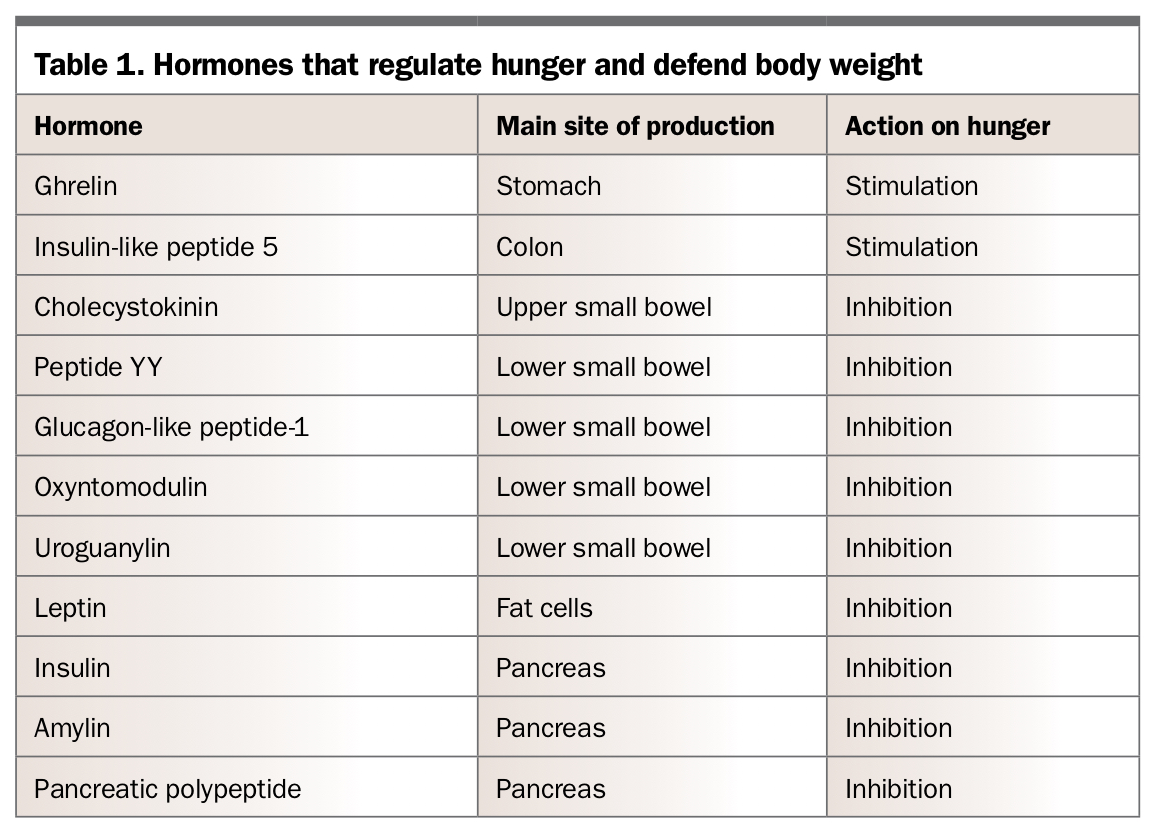{kind=link}
Although most people gain weight when taking insulin, there is good evidence that insulin inhibits hunger when it enters the brain. Insulin detemir is the only insulin that is weight neutral. This insulin has been made long-acting by the addition of a fatty acid molecule. Its increased lipophilicity means that it can enter the brain more easily than other insulins, and thus have a greater hunger inhibition effect to counter its peripheral weight-gaining effects.
Soon after the discovery of leptin in 1994, it was found that levels of this hunger-inhibiting hormone decrease dramatically after diet-induced weight loss.8 In contrast, levels of the hunger-stimulating hormone ghrelin were found to increase after weight loss.9 It was then shown that levels of cholecystokinin, another hunger-inhibiting hormone, also decrease after weight loss.10 These changes lead to increased hunger. In 2011, it was demonstrated that other hormones also change to increase hunger and that these changes are long lasting.11 These feedback loops explain why it is difficult to maintain weight loss in the long term and why lifestyle advice only leads to modest weight loss.
Management of people with obesity and type 2 diabetes
The strategy described below is the author’s own approach to weight loss in people with type 2 diabetes and can be used in those at any stage of the condition from prediabetes to long-established diabetes.
If the person is taking insulin it is wise to check endogenous insulin production by measuring C-peptide levels; glucose levels should be measured at the same time to help interpret the C-peptide measurement. In those with adequate C-peptide levels for the prevailing glucose level, insulin injections may possibly be stopped if there is adequate weight loss.
Very low energy diets
The best way for a patient to lose weight is to follow a VLED of only 3200 kJ/day.12 These diets allow rapid weight loss and control hunger while maintaining micronutrient levels. The patient replaces breakfast and lunch with a VLED product (e.g. a shake, bar or soup) and has a proper meal for dinner. This meal consists of protein (the size of the hand), three nonstarchy vegetables and a salad. It is important to also advise the patient to eat a small amount of fat (olive oil, margarine, butter) each day to maintain gall bladder emptying and thereby help prevent gallstone formation.
VLEDs are low in carbohydrate so patients will become ketotic from day three and will not be hungry. Ketones suppress hunger by providing an alternative energy source to the brain and preventing the change in hunger hormones described above.13 For the first two days, patients can eat a protein source such as roast chicken at anytime to help control hunger.
The patient continues the VLED until the target weight is reached. If the patient is taking insulin or sulfonylureas it is essential to halve the dose of medication and ask them to monitor their glucose levels more closely because a VLED reduces blood glucose levels dramatically.
Modern VLEDs are well formulated and are safe to use for a prolonged period of time.14 It is often stated that 5% weight loss is very beneficial; however, although a modest weight loss is beneficial, a large weight loss is even better. It has been shown that patients who have type 2 diabetes respond well to a VLED especially if they are not taking medications that increase insulin levels.15
When the target weight is reached
Once the target weight is reached, the patient should be weaned off the VLED over two months. Firstly, the lunchtime VLED is stopped and replaced with a salad and protein. After one month, the VLED is stopped completely and the patient is advised to eat ordinary meals. During this phase it is important to refer the patient to a dietitian who can prescribe an energy-reduced balanced diet that is nutritionally complete.
The introduction of carbohydrates will clear the ketones and the patient may experience hunger. At this time, the patient should be reviewed frequently to allow intervention before too much weight is regained.
Hunger control
Several medications may be used to control hunger. Three of these agents, phentermine, bupropion/naltraxone combination and liraglutide, are approved by the TGA for weight management (Table 2); others are used off label, and include topiramate and exenatide. In the author’s opinion it is best to use submaximal doses of several medications rather than a high dose of a single medication (e.g. start with liraglutide 0.6 mg subcutaneous injection plus phentermine 15 mg and topiramate 12.5 mg [half a 25 mg tablet] in the morning). This limits side effects and increases efficacy. Do not combine phentermine and bupropion together as this has the theoretical risk of increasing circulating serotonin levels which may cause sclerosis of heart valves.
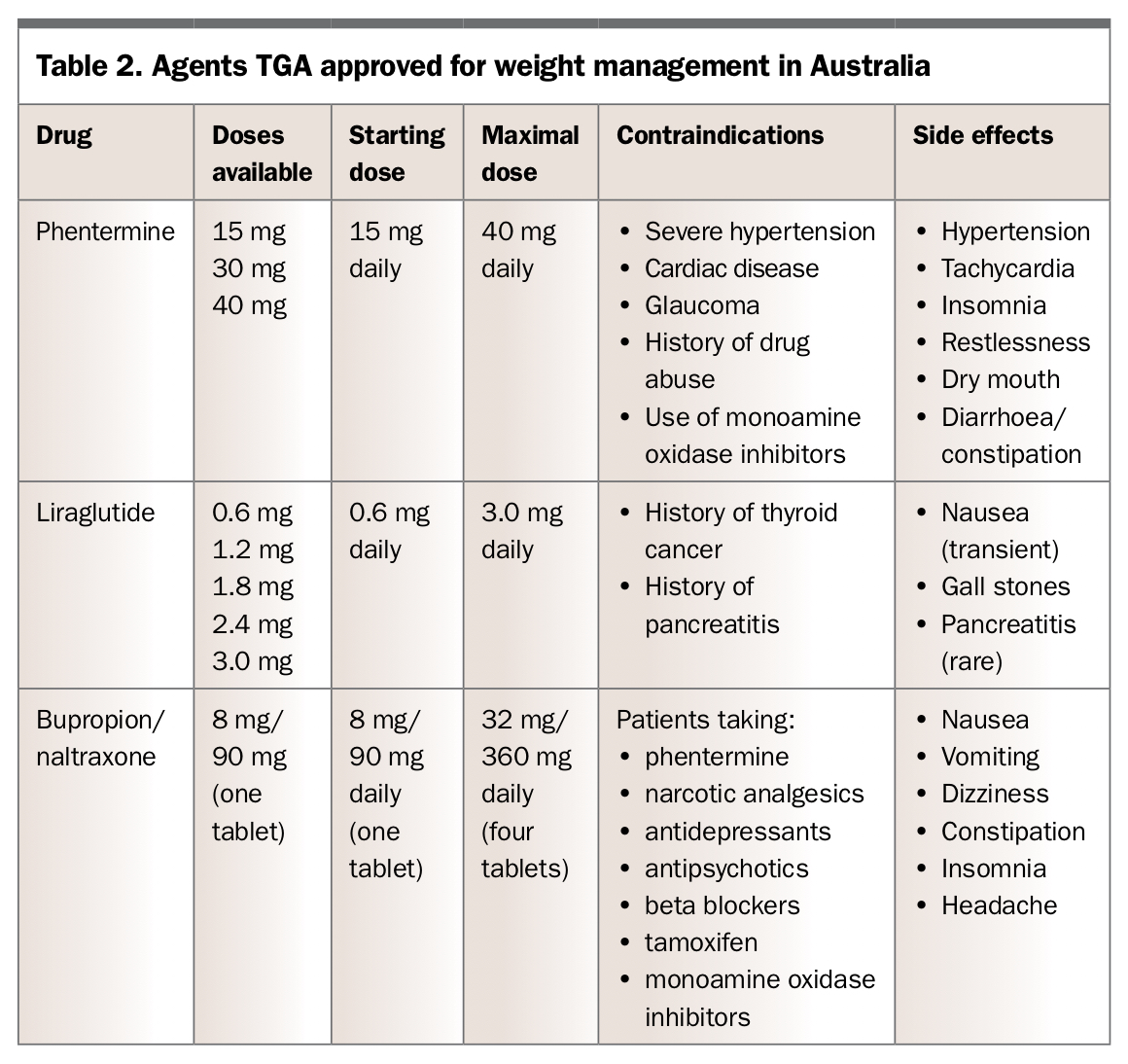{kind=link}
Bariatric surgery
If the patient fails diet therapy or cannot take hunger-suppressing medication, either because of cost or other contraindications, bariatric surgery should be considered. Adjustable gastric banding, sleeve gastrectomy and roux-en-Y bypass are the three bariatric surgery operations currently used in Australia. The type of operation used will depend on discussions between the patient and the surgeon. Most bariatric surgery operations are performed in private hospitals.
Following substantial weight loss, many (but not all) people taking insulin can come off insulin and some with pre- or early diabetes can come off all medication. How long this remission lasts is unclear. If glucose levels start to increase again, medications that do not cause weight gain should be used (Box).
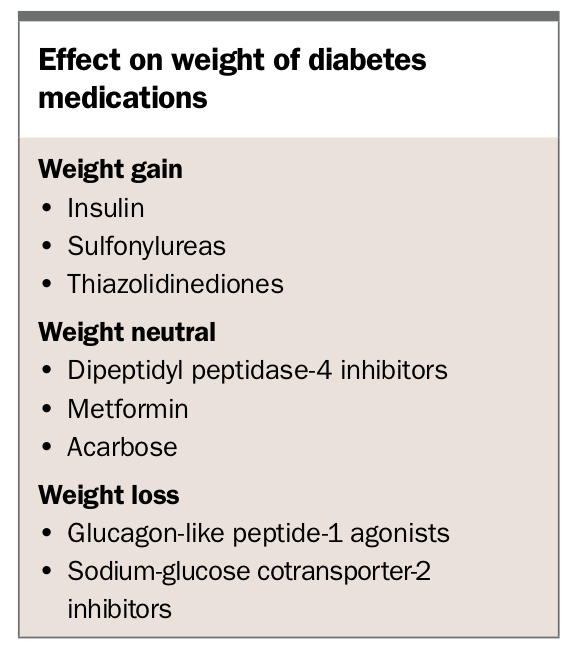{kind=link}
Conclusion
Obesity, by causing insulin resistance and impairing beta cell function, is the main driver of type 2 diabetes. It follows that weight loss is a powerful strategy to lower blood glucose levels. Weight loss is best achieved with a VLED but must be followed by an indefinite weight-maintenance phase. This includes lifestyle changes but often also appetite-suppressing medication. MT