When the smoke clears. Supporting communities after a disaster

There is an increased risk of short- and long-term mental health impairment following a disaster, such as the recent Australian bushfires. Timely and effective reconstruction and practical assistance have a key role in supporting mental health. GPs also have a central role in monitoring and providing long-term care for patients who have been exposed to bushfire trauma.
- Psychological distress is common after a disaster and does not always suggest a mental disorder or require treatment.
- Community mental health is best supported by practical reconstruction initiatives and support for individuals to return to pre-bushfire levels of personal and financial resources.
- Psychological First Aid provides a framework to combine practical and psychologically informed responses after a natural disaster.
- People with acute or pre-existing mental health conditions should be identified and provided with timely access to specialist care.
- People most severely exposed to critical incidents, those who have lost a family member or close friend, and those who have had their home or livelihood destroyed have a higher risk for developing mental health impairment.
- Conditions with increased frequency after a disaster include post-traumatic stress disorder (PTSD), depression, prolonged grief reactions and adjustment disorder, as well as harmful behavioural responses such as heavy drinking, family conflict and intimate partner violence.
- The real mental health burden is likely to emerge over the medium- and longer-term when many emergency services and additional resources have moved on.
- Trauma-focused psychological interventions are recommended as the first-line treatment for PTSD. Selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors may be helpful if other treatments are not available.
- Children exposed to bushfire risk or living with a parent with post-traumatic mental health difficulties are at risk of PTSD and heightened internalising and externalising disorders.
- Physical health comorbidities need to be actively monitored.
The magnitude and extent of the 2019-2020 bushfire season have affected multiple states and communities across Australia, with growing concern that this marks a significant turning point in climate change-enhanced bushfire risk and extreme climatic events. The prolonged nature of the crisis saw large numbers of volunteer firefighters and communities exposed to extended periods of risk, adversity, loss and tragedy. Over 2400 homes were destroyed, with the destruction of vast tracts of rural infrastructure, livestock and native animals. The bushfires resulted in the tragic deaths of 34 individuals, including volunteer firefighters working to protect homes and communities.
In the wake of the disaster, the Prime Minister announced a A$76 million funding package for the provision of mental health support and access to trauma-informed specialist services that can be immediately provided to firefighters, emergency personnel, and individuals and communities affected by the bushfires. The prioritisation of mental health as the disaster was unfolding highlights the extent to which concerns for mental health has risen to prominence in disaster response planning.
It is important that any mental health interventions are guided by the evidence around disaster management and intervention. There has been considerable controversy over how to appropriately meet mental health needs in the immediate aftermath of a natural disaster. A new provision under the Prime Minister’s funding announcement provides direct access to psychologists, social workers and occupational therapists, removing previous requirements for a primary care mental health plan.1 This is intended to improve access to direct care in rural regions funding telemental health, but may raise the possibility of fragmented and nonintegrated care. This article outlines some of the key issues and clinical conditions that are important to consider across the postdisaster recovery period. It remains a fundamental contention that the GP should remain at the centre of physical and mental health care.
Learning from past mistakes
There has been a long history of delivering mental health and psychosocial responses following critical incidents and disasters. Previous attempts to implement community-wide mental health programs have had mixed results. A key example of this is the use of critical incident stress debriefing (CISD), an approach to trauma counselling that attempts to help patients process distressing events after a crisis through discussing their experiences and emotional reactions. The theory behind CISD is that early identification and intervention may mitigate the impact of psychological trauma and support accelerated recovery. Unfortunately, the outcomes of repeated trials of CISD indicated that the procedure increased the risk of mental health impairment for some participants.2,3 The reasons for this remain unclear but may relate to the complex processes involved in the consolidation of fear memories, which become disrupted in some individuals by pre-emptive efforts at assisted trauma processing.4
Distress or mental disorder?
Emotions, psychological distress and mental health interact in complex ways during the acute phase of an unfolding emergency. Symptoms that would raise concern at a later stage of the emergency can be prevalent and part of a normal stress response during the acute postdisaster period. Mental health screening studies following acute disasters have identified individuals who will develop mental health impairment and false-positive individuals who have transient distress responses.5 Assistance or interventions that pathologise all distress reactions cause undue alarm and shift the focus away from the delivery of more important and helpful critical responses.
However, not all symptoms in the acute period after a disaster should be normalised. Severe acute post-traumatic symptoms have been shown to be predictive of longer-term impairment. Epidemiological data also suggest that one in five individuals in a disaster zone will have a pre-existing mental health disorder6 and will require access to ongoing care. There is a high risk that a disaster event could lead to clinical deterioration in an existing mental health condition or the onset of a new mental health condition. It is also important to recognise that individuals with pre-existing vulnerabilities and those in communities that have been most severely exposed are considered high risk for mental distress after a disaster event (Box 1).
{kind=link}
A guiding principle is that individuals who meet the criteria for a mental disorder following a disaster require timely access to mental health care. This should be combined with a wait-and-watch approach for individuals who experience heightened psychological distress. The greatest concern documented in past disaster settings is the low level of identification of enduring mental health conditions that emerge after the acute crisis has passed.7
The best mental health support involves practical assistance and limiting resource loss
The mental health of individuals who have suffered through a disaster is closely linked to the degree of resource loss within a community. Restoring individual resources is an important strategy for limiting mental health impairment in postdisaster studies.8 After the 2009 Black Saturday tragedy in rural Victoria, stressors in bushfire-affected communities, including loss of accommodation, financial strain and relationship breakdown, were major determinants of subsequent risk of post-traumatic stress disorder (PTSD), depression and heavy drinking.9 Five years after the disaster, people with reduced stressors no longer had an elevated mental health risk compared with those with continuing resource stress, who showed a continued increase in risk.10 Restoration of housing in economically vulnerable populations resulted in a shorter duration of mental health impairment with up to five times the remittance rate of PTSD compared with those without such help.11 In the context of the recent bushfires, loss of infrastructure and displacement, homelessness and financial stress of those affected may trigger prolonged spirals of resource loss that could lead to increased risk for individual and community-level mental health impairment.
The key message is that mental health care is not an alternative to timely, effective and targeted post-disaster reconstruction and financial support. Health professionals should be key advocates for prioritising practical solutions to these problems.
Early intervention to support community mental health
Psychological First Aid (PFA) has become the most widely used framework to support the delivery of psychosocial aid following a natural disaster or complex emergency.12 This approach should be distinguished from Mental Health First Aid, which is a training program addressing mental health literacy.13
PFA strives to combine material aid, service linkage and psychological support to guide first responders and para-professionals in providing assistance in disaster settings. Across most applications, PFA focuses on:14
- gathering information about the disaster setting and available services
- contacting disaster survivors
- maintaining and restoring safety
- providing practical assistance
- linking people to appropriate services
- reconnecting people to family, friends and support
- supporting helpful coping.
Detailed training modules have been developed by multiple agencies (World Health Organization, Red Cross USA and Australia).
PFA is distinguished from trauma therapy approaches by actively discouraging detailed trauma discussion or the use of trauma-processing strategies. There has been limited evaluation of the efficacy of PFA in supporting better long-term mental health outcomes.15,16 The few studies that have been undertaken provide support for the use of a structured approach that focuses on a case brokerage model to link people to resources and services.11,14 There is little evidence to support the counselling element of PFA, with commentators noting the potential dangers of providing immediate counselling in these settings.17
Recognising and treating acute stress disorders
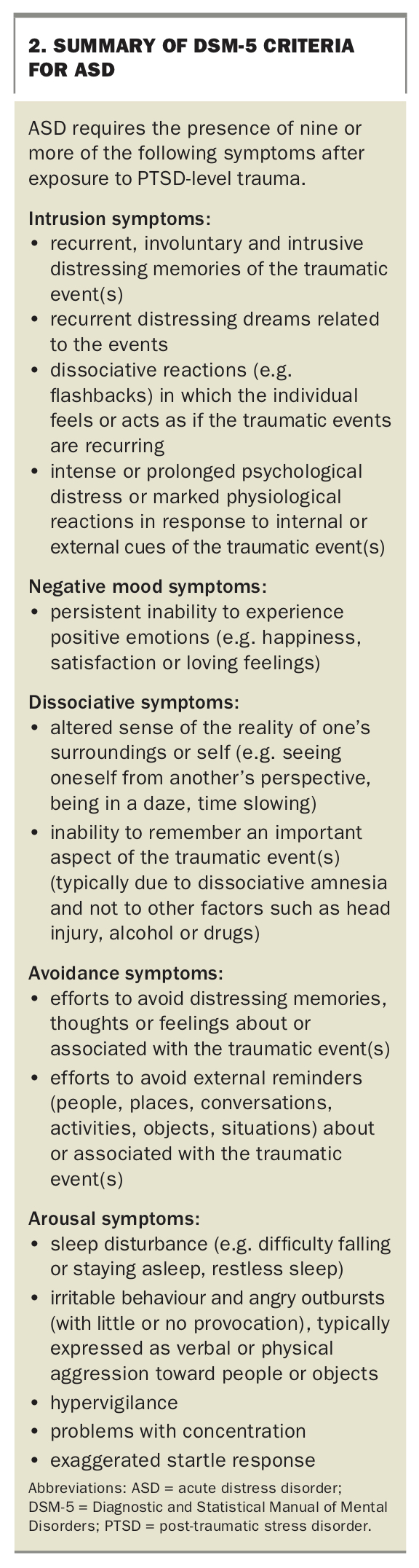
After a major disaster event, some individuals are likely to experience acute mental health reactions. Acute stress disorder (ASD) is a mental health condition that has been documented to occur in the first month after a critical incident or disaster event. Over 50% of those identified with ASD are likely to transition to a chronic mental health condition, most commonly PTSD and major depression.18 The Diagnostic and Statistical Manual of Mental Disorders (DSM5) criteria for diagnosing ASD (Box 2) requires the presence of a greater number of symptoms than PTSD, reflecting the high prevalence of these symptoms in the immediate post-traumatic period.
{kind=link}
Earlier conceptions of ASD diagnosis highlighted the importance of dissociative symptoms such as derealisation, numbing, detachment, memory impairment and absence of emotional responsiveness. Although these remain common, more recent research indicates that ASD presentations are marked by the overall severity of acute PTSD symptoms. The provision of psychological intervention for ASD has been shown to be effective, with the greatest evidence for trauma-focused cognitive behavioural therapy interventions.19
Post-traumatic stress disorder and other traumatic stress reactions
The Black Saturday Bushfires Study found that PTSD was one of the most common mental health outcomes for high fire- affected regions, with one in five of those surveyed identified as having PTSD three to four years after the disaster. The risk for PTSD is most directly linked to the ‘trauma dose’, which is characterised by the number and severity of lifetime trauma events. Seminal research undertaken among volunteer firefighters exposed to the 1983 Ash Wednesday tragedy in South Australia found a direct association between fire exposure severity and the number of PTSD symptoms,20 a relationship confirmed many times over since this study.
The provision of evidence-based trauma-focused psychological intervention for PTSD is recommended as a first-line treatment, with the strongest evidence supporting prolonged exposure therapy, cognitive processing therapy and eye movement desensitisation and reprocessing (EMDR).21 The Bushfire Medicare Benefits Schedule items1 allowing psychologists and social workers to provide telemental health services may assist GPs to link regional patients to trauma-focused mental health professionals in areas where these services are not available locally.
Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) may be helpful as a first-line intervention in managing comorbid conditions that present with PTSD, such as depression. SSRIs and SNRIs may have a small positive benefit on PTSD symptoms and can be used if other treatments are not available. Current evidence supports the use of fluoxetine, paroxetine, sertraline and venlafaxine.21-23 The reader’s attention is drawn to the Medicine Today article on recognising and managing PTSD, which provides more detailed information on assessment, management and treatment.24 Attention should also be drawn to the Australian guidelines for the treatment of ASD and PTSD, which include a medications prescribing algorithm for the treatment of PTSD.25
Recognising delayed onset and preventing delayed treatment
An important feature of PTSD is the capacity for the condition to be associated with a delayed onset, a common feature in first responders.26,27 PTSD is often associated with a chronic course with over 50% of cases found to persist at 14 years after onset.28 Only a minority of those with PTSD appear to get access to evidence-based trauma-focused psychological treatments.29 This highlights the critical role for the GP in undertaking long-term monitoring of patients and being aware of important times such as anniversary events or the impact of new threats that could trigger a delayed onset.
There have been two recent clinical developments that are important to be aware of in managing and understanding traumatic stress conditions: complex PTSD and moral injury.
Complex PTSD
A new diagnosis of complex PTSD (cPTSD) has been incorporated into the International Classification of Diseases 11th Revision (ICD-11) diagnostic system. This diagnosis includes all the standard PTSD symptoms but also includes additional symptoms associated with affect dysregulation, negative self-concept and disturbances in relationships. At this time there is no clear evidence that cPTSD requires a different approach to treatment, although recommendations have been made to support the value of combining traditional treatments for PTSD with other strategies to support the deficits associated with cPTSD in distress tolerance, self-concept and interpersonal effectiveness.30
Moral injury
Another development that may have some importance is the issue of moral injury. This is a notion that has emerged within veteran and military health settings but seems to have a strong resonance with the experience of many first responders. Moral injury refers to the impact that results from settings where an individual ‘perpetrates, fails to prevent, bears witness to, or learns about acts that transgress deeply held moral beliefs and expectations.31 In military veterans, exposure to morally injurious events is linked to the onset of PTSD and other post-traumatic reactions dominated by feelings of guilt, shame, anger or embitterment related to the nature of the moral injury encountered.32 The work of first responders in disaster zones, where difficult decisions have to be made that may have far-reaching consequences, places them at particular risk for moral injury.
Major depression
The multiple stressors and losses associated with natural disasters are also associated with elevated rates of depression. In the Beyond Bushfires study, rates of major depression three to four years after the event were found to be around one in eight in the high-fire-impact zones, which were twice that compared with low-impact zones. As with PTSD, depression onset and maintenance were closely linked to the number of post evidence-based trauma-focused psychological intervention disaster life stressors.10 Depression can also increase symptoms of PTSD prospectively in disaster settings, highlighting the importance of providing timely intervention where possible.33 Key strategies for assessing and managing depression, mood disorders in primary care and advice on managing treatment-resistant presentations are available in recently published articles.34-36
Adjustment disorder following disaster events
Although not as disabling as depression, it is important to be aware of the risk of adjustment disorder after exposure to multiple losses arising from a disaster. Adjustment disorder provides a diagnostic description to identify individuals whose exposure to a psychosocial stressor leads to prolonged impairment and disability. Although the population prevalence of adjustment disorders is low, at around 1 to 2%, adjustment disorders have been found to be particularly high following exposure to traumatic or high adversity events.37
Adjustment disorders after traumatic incidents can often be misdiagnosed as PTSD, leading to inappropriate treatment and referrals. There is growing evidence that adjustment disorder responds to low-intensity psychological interventions and is amenable to e-mental health application.38 The Skills for Life Adjustment and Resilience (SOLAR) program is one approach developed in Australia for survivors of disasters experiencing ongoing distress and adjustment difficulties.37
Prolonged grief reactions
Prolonged grief reactions following traumatic bereavement can occur with reasonable frequency. The description of prolonged grief disorder outlined in ICD-11 provides a useful evidence-based framework for identifying grief reactions. These are described as a "pervasive grief response characterised by longing for the deceased or persistent preoccupation with the deceased accompanied by intense emotional pain (e.g. sadness, guilt, anger, denial, blame, difficulty accepting the death, feeling one has lost a part of one’s self, an inability to experience positive mood, emotional numbness, difficulty in engaging with social or other activities). The grief response has persisted for an atypically long period of time following the loss (more than 6 months at a minimum) and clearly exceeds expected social, cultural or religious norms for the individual’s culture and context",39 noting that this disturbance should also be associated with significant personal, family, social, educational and occupational impairment. Approximately one in 10 bereaved individuals will experience a prolonged grief reaction, a rate that is higher for traumatic bereavements.40,41
Traditional bereavement services do not appear to result in significant improvement for prolonged grief disorders.42 There is growing evidence that targeted interventions designed specifically for prolonged grief are effective and associated with significant improvement.43 At present these are only available at specialist services.
Emergence of harmful behavioural patterns
Alcohol
Mental health monitoring of communities affected by the Black Saturday fire tragedy found a pattern of higher levels of heavy drinking among the highest affected regions.10 Although this was evident for both men and women, the highest levels of heavy drinking were among men, a pattern consistent with epidemiological data.44 Heavy drinking also showed one of the lowest levels of change at subsequent waves of assessment, underscoring the intractable nature of potentially harmful levels of alcohol consumption.
There is often high comorbidity among mental health and substance use disorders. Research that has sequenced the onset of drinking problems after traumatic exposure found problematic drinking patterns often follow the onset of post-traumatic symptoms.45 Many GPs may feel some reluctance to engage in discussions with patients over alcohol consumption levels. There are useful evidence-based strategies available to assist with this.46
Family conflict and intimate partner violence
The impact of disasters on interpersonal and family functioning should also be noted. Separation during a fire event is a common occurrence that is associated with longer-term psychological problems.
Although the family will be the main source of support, post-traumatic reactions and ongoing adversity can lead to increased levels of family conflict. High levels of irritable distress documented at eight and 26 months after the Ash Wednesday fires had a prolonged adverse effect on families.47 In the communities affected by the Black Saturday fire, anger reactions were documented as a major post-traumatic outcome and impacted on ongoing impairment levels.48
Increased risk for intimate partner violence as families come under enormous pressure has also been documented in the aftermath of disaster settings.49 Useful support guides are available to support the GP in identifying and responding to women and men presenting with exposure to intimate partner violence.50-52
Physical health outcomes
There is growing evidence across the spectrum of mental disorders of an increased association with poor physical health, risk of disease and reduced access to physical health care.53 The range of health disparities that people with a mental disorder face appear to largely be a consequence of the accumulation of modifiable health-related behaviours.53 GPs have a key role in maintaining a focus on the emergence of physical health impairments for patients affected by mental health disorders.
Working with patients to address key risk factors such as increased sedentary behaviour, reduction in psychical activity and poor diet, not only address health disparities, but have been shown to have positive benefits on a range of mental disorders.53 This can be greatly assisted by linking with allied health professionals such as exercise physiologists, physiotherapists and dietitians, many of whom increasingly have specialist experience working with individuals affected by mental disorder.
Older person needs
Demographic trends in Australia show an increased tendency for retirees to relocate from capital cities to regional areas. This, combined with an ageing population and lower immigration to rural settings, results in large numbers of older people living in high bushfire threat zones. Older adults have an increased risk of developing mental health difficulties following natural disasters than younger cohorts,54 and are more likely to have lower disaster preparedness, less likely to receive advance warnings, and are at greater risk of exposure, injury and fatality.55-58 Older people may also be more vulnerable to the longer-term impact of disasters including impacts on livelihood, reflecting a greater difficulty in re-establishing income and savings. This is combined with a higher level of chronic physical impairment and multimorbidity, resulting in higher levels of functional disability, social isolation, healthcare utilisation and reduced psychological wellbeing.59
Recommendations for disaster response initiatives for older Australians are broadly the same as for other populations, noting the needs of high-risk groups.60,61 Individuals with cognitive decline or physical-related impairment face particular difficulties during evacuation events, as do those involved in their care.58 The Seniors Without Families Triage tool (SWIFT) has been developed as a screening instrument during the acute phases of a disaster response to identify vulnerable older adults and structure the intensity of service required from high need, involving medical and/or social work support and placement, to case management and brokerage support, to referral to a community volunteers.62
Needs of children
There has been extensive research into the mental health impact of disasters on children and young people. As with adult populations, a dose-response relationship between the level of disaster exposure and the development of PTSD is clearly apparent. Factors that confer an increased risk to PTSD among children include:63,64
- female gender
- older age
- bereavement
- higher disaster fatalities
- greater proximity to the disaster
- perceived threat
- separation during the disaster event
- level of distress at the time of the disaster.
A broadly similar set of risk factors have been associated with postdisaster levels of depression in adolescents.65 Among younger children, disaster exposure is associated with increased internalising (worry, depression, anxiety) and externalising disorders (aggression, disruptive behaviour and conduct problems). Externalising disorders manifest more often after the first year following the disaster, a time when many of the major disaster response programs have ceased,66 and this response could be misunderstood as isolated behavioural issues by schools and parents. A strong association between children’s mental health and the severity of the parents’ mental health responses following disasters has been documented.67,68 It is therefore important that GPs consider the mental health of children when identifying mental health impairment among parents.
There is evidence of reduced academic outcomes for highly exposed children. Children aged 9 to 12 years attending primary school in high fire-affected areas two to four years after the 2009 Black Saturday tragedy had lower than expected gains in numeracy and literacy compared with children attending schools with lower levels of bushfire impact. A similar finding was documented by the Ash Wednesday Child Wellbeing study, with high-exposure children having poorer educational outcomes than a control group, a finding still evident 20 years following the disaster.69 These findings underscore the need for a public health response to address the needs of children affected by mass disasters.
A substantial body of research has demonstrated the effectiveness of mental health interventions for symptoms of PTSD, depression and distress in children.70-72 Access to specialist child psychological services for children affected by the bush fire is accessible through the recent government Mental Health Services for Bushfire Response.1 Referrals can also be made to Headspace centres for young people between aged 12 and 25 years including telemental health support services.73 Teacher-assisted interventions can have a positive impact on children’s mental health and academic performance.74
Caring for first responders
There has been concern regarding the impact of the bushfire crisis on the many thousands of volunteer firefighters who have been directly exposed to the fire event. As with other first responder groups, the risk associated with volunteer fire fighting relates to the cumulative impact of exposure to critical incidents and their severity.75-78 There is a clear ongoing need for the State Volunteer Fire Services to develop and maintain surveillance systems that link volunteers, professional firefighters and other first responders to care when needed.
A major challenge is the long delay between the onset of disabling symptoms and access to evidence-based care. Clinical experience indicates that many first responders do not recognise the development of PTSD symptoms and research suggests that they may attempt to manage the early onset of PTSD symptoms by increasing commitment to work and disengaging from other life activities.79 GPs should be aware that individuals who were directly involved in volunteering during the bushfire crisis may be at risk of developing PTSD and should be monitored. Detailed treatment recommendations are outlined within the Australian guidelines for diagnosis and treatment of PTSD in Emergency Service Workers.26
Conclusion
Bushfires and other natural disasters will continue to be a part of the Australian experience. This article has focused on the importance of responding to the mental health needs of communities and individuals affected by a disaster. It is important to note that this needs to be balanced against a body of research that also shows that times of adversity like this also forge many positive outcomes, including community connections and bonds following the event that are deeply protective. In supporting those affected, the most immediate need will be material and financial assistance in the acute phase with a small number of individuals requiring urgent mental health care. The real mental health burden emerges over the medium and longer-term when many of the emergency services and additional resources have moved on. GPs have an important role in identifying and managing the key mental health needs of the community in the longer-term. MT