Asthma in adolescents: often overlooked, not to be forgotten

Dr Palit is a Fellow in Paediatric Respiratory Medicine and Adolescent Health at the Sydney Children’s Hospital Network, Sydney; and a Senior Lecturer in Health Services Management, School of Public Health and Community Medicine, UNSW Sydney, Sydney.
Dr Jayasuriya is a Consultant Paediatrician in the Department of Respiratory Medicine and an Honorary Consultant in the Department of Adolescent Medicine, The Children’s Hospital at Westmead, Sydney; and a Clinical Lecturer in the Discipline of Paediatrics and Child Health, Faculty of Medicine, The University of Sydney, Sydney.
Associate Professor Towns is Head of Adolescent Medicine for The Sydney Children’s Hospitals Network; a Consultant Paediatrician in the Department of Respiratory Medicine, The Children’s Hospital at Westmead, Sydney; and Clinical Associate Professor in the Discipline of Paediatrics and Child Health, Faculty of Medicine, The University of Sydney, Sydney, NSW.
Asthma
Asthma in children

The management of adolescents and young people with asthma can be challenging and requires clinicians to consider life stage, development and psychosocial factors to ensure treatment is both appropriate and effective.
- Confirm the diagnosis of asthma with objective tests and monitor regularly to avoid over- or undertreatment.
- Review the young person alone for at least part of your consultation and provide reassurance regarding confidentiality.
- Develop, discuss and update an asthma action plan at every visit.
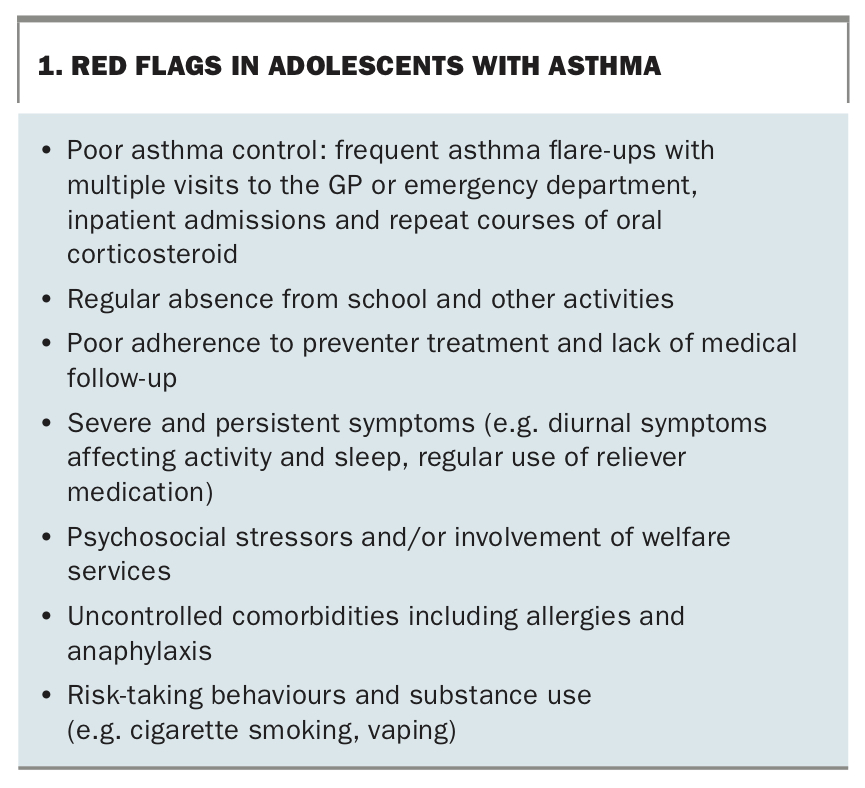
- Red flags for patients at high-risk of asthma include poor asthma control, nonadherence, under-recognition of symptoms, psychosocial stressors, risk-taking behaviours and communication barriers.
- Embrace digital health technologies in your clinical practice as they have been shown to improve adherence and symptom control.
Adolescents with asthma present a unique set of challenges for the discerning clinician due to their developmental stage, physiological changes and the emergence of psychosocial factors that can impact management. Adolescents may modify their behaviours due to poor asthma control or under-recognise their symptoms leading to poor adherence to treatment. Nonadherence to asthma medications is a well-known problem in the adolescent age group, further complicated by risk-taking behaviours such as smoking, vaping and other substance use, which can lead to unexpected exacerbations and complications.
Parents are often surprised when their teenage child has an asthma episode, having been told they would outgrow their childhood asthma. Although some children with asthma do seem to recover, adolescents with childhood asthma should continue to be actively screened for symptoms of wheeze, chest tightness and shortness of breath. Recent data from the Australian Institute of Health and Welfare National Health Survey 2017–18, shows that the prevalence of asthma in young people aged 15 to 24 years is about 10% in both sexes, similar to the 0 to 14-year-old age group (12% boys and 8% girls, respectively).1 Puberty does not predict remission of asthma and almost two-thirds of children with chronic asthma have persistent symptoms throughout puberty.2 Additionally, it is relatively common for asthma to first present during adolescence and this occurs more commonly in girls than boys.3
GPs play a key role in the assessment and management of adolescents and young people with asthma. Most primary care providers are well versed in the use of National Asthma Action Plans (AAPs) such as those available via the National Asthma Council Australia.4 Written and digital AAPs are one of most effective clinical interventions we have and should be revisited at every consultation. Regularly updated AAPs have been shown to:
- improve adherence
- reduce school absenteeism
- reduce GP presentations
- reduce visits to the emergency department and hospital inpatient admissions.
As GPs rightly continue to provide the bulk of care for adolescents with asthma, it is important to consider the following during clinic visits:
- identify adolescents who are vulnerable or at high risk (Box 1)
- address poor adherence and comorbid psychosocial issues
- promote ongoing self-management and emerging independence
- refer patients early for further assessment when the diagnosis is uncertain, there is treatment failure or red flags emerge (Box 1).
{kind=link}
Diagnosis
Asthma is characterised by episodes of wheeze with shortness of breath, often precipitated by triggers such as viral infections or environmental factors. The recently updated Australian Asthma Handbook version 2.1 is an online evidence-based clinical guideline for asthma management and has a section specifically for asthma management in adolescents.5
As primary care providers, it is important to be clear about what constitutes asthma and what may otherwise be masquerading as variable airflow limitation. A detailed history and physical examination, use of objective measures of airway function and assessment of atopic status are needed to confirm a diagnosis of asthma. Investigations to consider that may require specialist referral include:
- spirometry including postbronchodilator response (withhold inhaled bronchodilators for a minimum of four hours before testing)
- fractional exhaled nitric oxide measurement – is helpful in identifying asthma phenotype (often associated with eosinophilic airway inflammation) and informing treatment decisions5,6
- allergen skin testing for common environmental and food allergens
- bronchial provocation (challenge) testing or exercise testing to establish evidence of airway hyper-responsiveness or reveal the cause of exercise-related symptoms. Challenge tests are useful for excluding a diagnosis of asthma as the cause of current symptoms. They are performed at accredited lung function laboratories and are indicated when asthma is suspected but initial spirometry does not demonstrate reversible airflow limitation7,8
- peak expiratory flow monitoring, although not routinely recommended, can be helpful in some circumstances to establish evidence of airflow variability and motivate adherence to treatment.
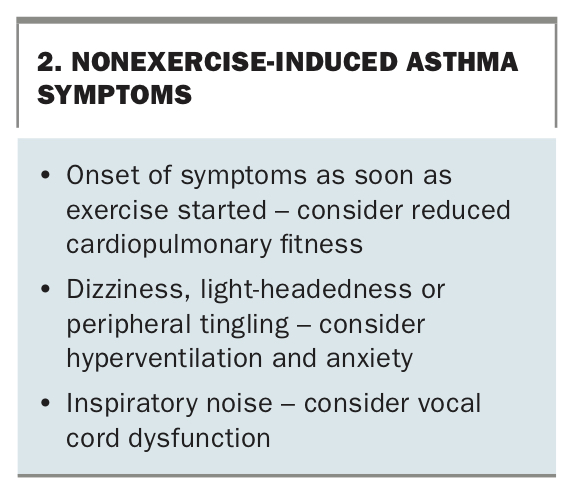
Exercise-related symptoms are common in the adolescent age group and may be caused by a variety of underlying factors not related to asthma. Adolescents may avoid exercise because of unrecognised asthma symptoms and therefore underappreciate the extent of their exercise limitations. Patients with exercise-related symptoms require accurate assessment to differentiate exercise-induced asthma from poor cardiopulmonary fitness, vocal cord dysfunction, hyperventilation, dysfunctional breathing and anxiety (Box 2).6,9
{kind=link}
Recurrent cough as the predominant or only symptom can be misleading. Somatic cough disorder (previously known as psychogenic cough or habit cough) is often misdiagnosed as asthma and patients treated inappropriately with inhaled corticosteroids.10 Anxiety and psychosocial factors may mimic or trigger acute asthma; however, these symptoms are associated with normal auscultation findings, lung function testing and oximetry. History is key here and will often reveal a rapid improvement of symptoms once the psychosocial trigger has been addressed.
Assessment
Alongside your respiratory review, think about other issues that may be contributing to the clinical presentation. Often the cause of poor adherence, escalating symptoms or ‘treatment failure’ in the adolescent may be due to the following factors.
Allergies
Allergic rhinitis is an independent risk factor for developing asthma and frequently coexists with asthma.11 As many as 75% of patients with asthma also have allergic and nonallergic rhinitis, although estimates vary widely.12 The unified airway disease concept of a single inflammation affecting both the upper and lower airways has become increasingly recognised in the literature as contributing to comorbid allergic rhinosinusitis and asthma.13 Studies have shown that children and adolescents aged 5 to 18 years with comorbid allergic rhinitis had worse asthma control and therefore stand to benefit from simultaneous treatment of both interrelated conditions.14,15
Sleep
Chronic sleep deprivation and sleep disorders are common in adolescents, made worse by poor asthma control with night-time awakening and daytime sleepiness negatively impacting healthcare outcomes and academic achievement.16,17 Obstructive sleep apnoea and sleep disordered breathing are both independent risk factors for severe asthma, and treating these conditions will improve asthma control.16,18 Night-time symptoms with awakening suggest uncontrolled asthma and possibly hypoxia. Consider referral to a specialist and performing overnight oximetry and/or polysomnography if night-time symptoms persist despite treatment.
Obesity
Being overweight can affect lung mechanics with reduced functional residual capacity, expiratory reserve volume and, to a lesser extent, total lung capacity. Additionally, obesity is thought to be a risk factor for asthma due to the mechanisms of underlying inflammation and genetics, and is currently an area of active research.19,20 Social prescribing with goal setting for your adolescent patient with asthma to increase activity levels (join a gym, enrol in an extracurricular activity or sport) and eat healthily can be a feature of every consultation. Exercise-induced asthma need not be a barrier to exercise, and optimal use of reliever medications 10 to 20 minutes before activity can be part of adolescent patients’ AAPs and communicated to all caregivers.
Hormonal changes
Early puberty, often associated with obesity, is an independent risk factor for the persistence and severity of asthma into adolescence and thereafter. Although the mechanisms are unclear, hormonal fluctuation during puberty affect asthma control and preventer treatment may need to be adjusted accordingly.21 Exacerbations of asthma symptoms may worsen during the premenstrual phase in 40% of females and, if poorly controlled, hormonal management should be considered.22
Mental health
Anxiety, depression and other mood disorders often emerge during adolescence, and early recognition, assessment and support is important to achieve optimal asthma outcomes. Poor adherence to treatment may be an early indicator of family problems, psychological distress and stressful life events.23 Anxiety may either mimic asthma symptoms or trigger them, and exercises to help control breathing, meditation, mindfulness and cognitive behavioural therapy and distraction strategies to reduce environmental stressors can help with self-management and improve outcomes for adolescents with asthma.24,25
Environment
Exposure to smoke and increased air pollution from bushfires can adversely affect lung health, leading to increased asthma exacerbations, hospital admissions and, in some cases, death. The 2019–20 ‘Black Summer’ bushfires caused multiple fatalities and significant respiratory morbidity, particularly across the eastern seaboard of Australia.26 In this context, population exposure to atmospheric particulate matter with a diameter less than 2.5 micrometres can cause widespread respiratory disease through oxidative stress and inflammation, and is a major public health concern.27
Thunderstorm asthma, seen not uncommonly during the spring and summer months in Australia, is triggered by massive loads of pollen allergen particles being released into the air. On days of high pollen count, fast-changing wind, temperatures and humidity can cause allergen particles to enter the bronchioles causing airway inflammation. The Melbourne thunderstorm asthma event in November 2016 led to 10 deaths and a 672% increase above the three-year average of respiratory-related presentations to emergency departments across Victoria.28
Substance use
Ask adolescents routinely about their substance use including smoking, vaping and other recreational drugs. Among those aged 12 to 17 years, cannabis is the most used illicit substance.29 Tobacco smoking has generally decreased among young people in Australia, with 5% of students aged 12 to 17 years reporting current use in the Australian Secondary Students’ Alcohol and Drug survey in 2017.29
More young Australians, about 5% of 18- to 24-year-olds, are experimenting with vaping and this growing trend, particularly among first-time smokers, should ring alarm bells. Smoking and vaping marijuana regularly confer considerable risk to pulmonary health (as seen in the increasing incidence of vaping-associated lung injury in North America), may trigger or exacerbate asthma symptoms and should be discussed with young people so they are aware of the risks.30,31
An approach to management
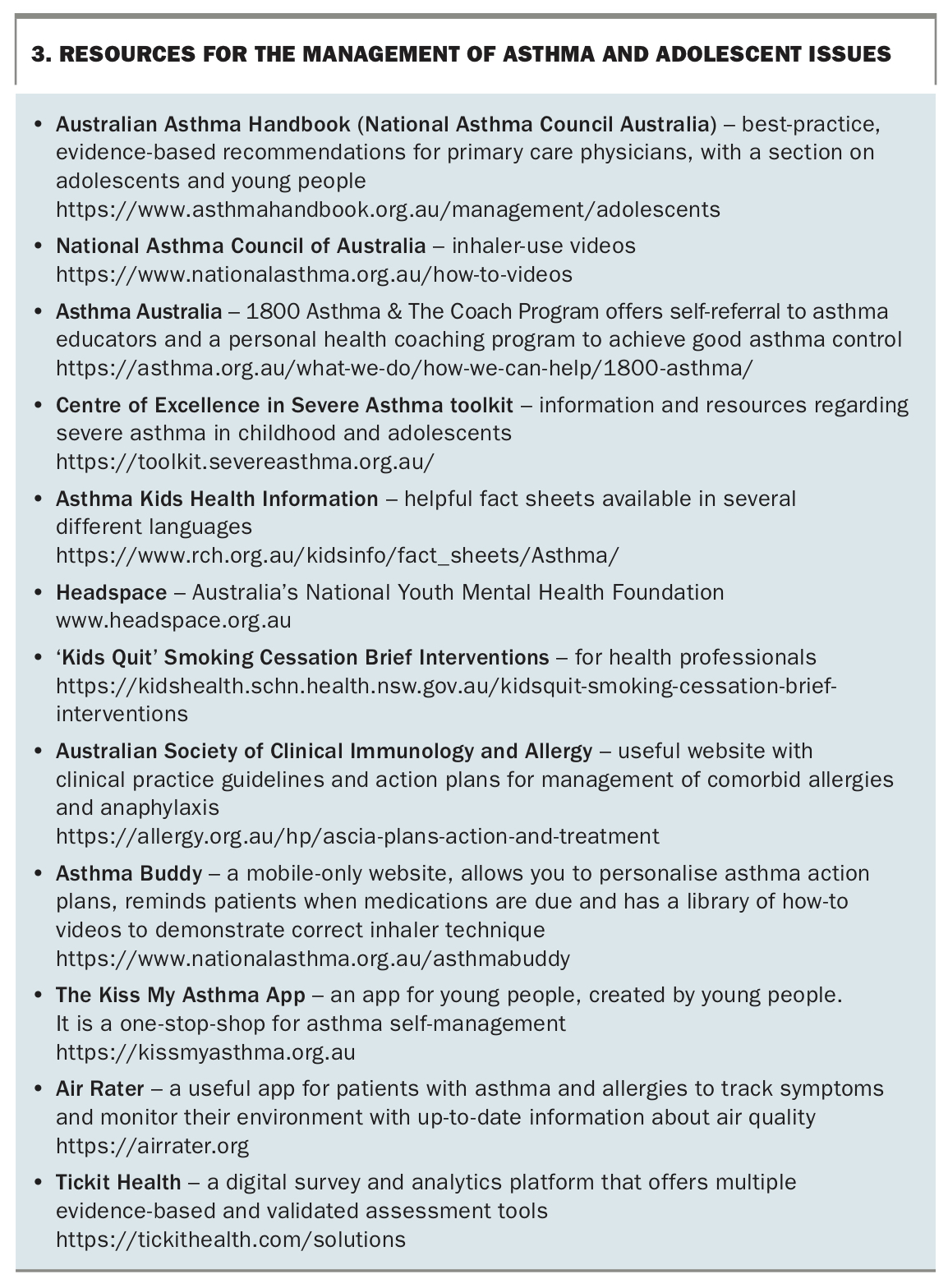
Clear, evidence-based, stepwise treatment recommendations are easily accessible in the Australian Asthma Handbook.6 When seeing an adolescent or young person with asthma, we recommend using the following approach and resources to maximise clinical effectiveness and engagement alongside online resources outlined in Box 3.
{kind=link}
Set the scene
- See the young person alone for at least part of the consultation and provide reassurance regarding privacy and confidentiality
- Consider cultural perspectives and health beliefs that may potentially impact the patient and their family
- Engage the family in the adolescent’s care and, for patients from non-English-speaking backgrounds, directly address parents and carers with the help of health interpreters
Educate
- Explore and encourage the adolescent’s self-management capacity by helping them to set goals and expectations around therapy
- Assess their understanding and provide re-education about medications, side effects and concerns
- Routinely check and reinforce correct inhaler technique
- Ask, in confidence, about smoking, vaping and other substance use and educate the young person (and their family) about potential harms
Adherence
- Ask open-ended questions to determine the degree to which the adolescent is participating with the agreed treatment plan. Find out what is working well and what is challenging for them to follow
- Negotiate the treatment plan to engage the young person and provide an opportunity for shared decision-making
- Promote regular routines and link taking medications to existing activities or set times of the day (e.g. before brushing teeth)
- Simplify treatment plans by choosing medications that need to be taken less frequently, for instance, a once-daily inhaled corticosteroid such as ciclesonide or fluticasone furoate, or combination therapy such as fluticasone furoate and vilanterol trifenatate
- Giving the patient a choice of preventer or reliever device, of which there is a dizzying number available, can help to empower and promote self-management (e.g. terbutaline sulfate turbuhaler is a useful reliever for patients unwilling to use a spacer, and easier to carry in a pocket or bag)
- Offer strategies to improve adherence and motivation including the use of digital apps, phone reminders and notifications (Box 3)
Identify risk factors
- Red flags for adolescents with asthma are outlined in Box 1. This cohort of patients will benefit from more regular GP review, engagement of the practice nurse and, if there are persisting issues, referral for specialist assessment
- HEEADSSS 3.0 (home environment, education and employment, eating, peer-related activities, drugs, sexuality, suicide/depression, sleep and safety from injury and violence) is a helpful psychosocial screening instrument (available electronically; Box 3) to identify areas of concern for adolescents32
- A home visit, particularly if the asthma is severe, is usually very informative in identifying triggers (e.g. animal allergens, house dust mites, mould, smoke)
- Changing school, moving homes or family disruptions can disrupt treatment plans and mask symptoms, leading to poor control
{kind=link}
Treatment
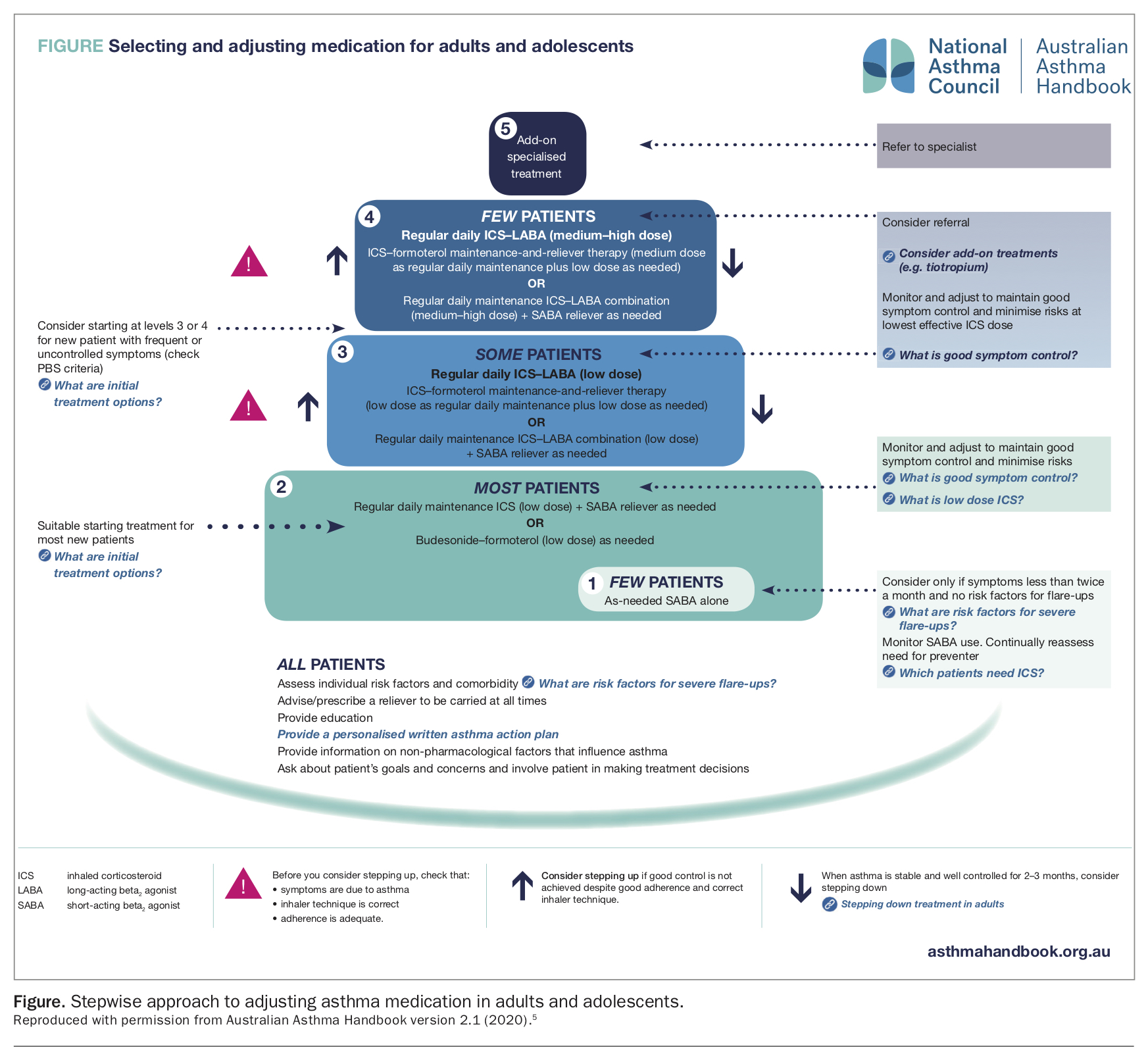
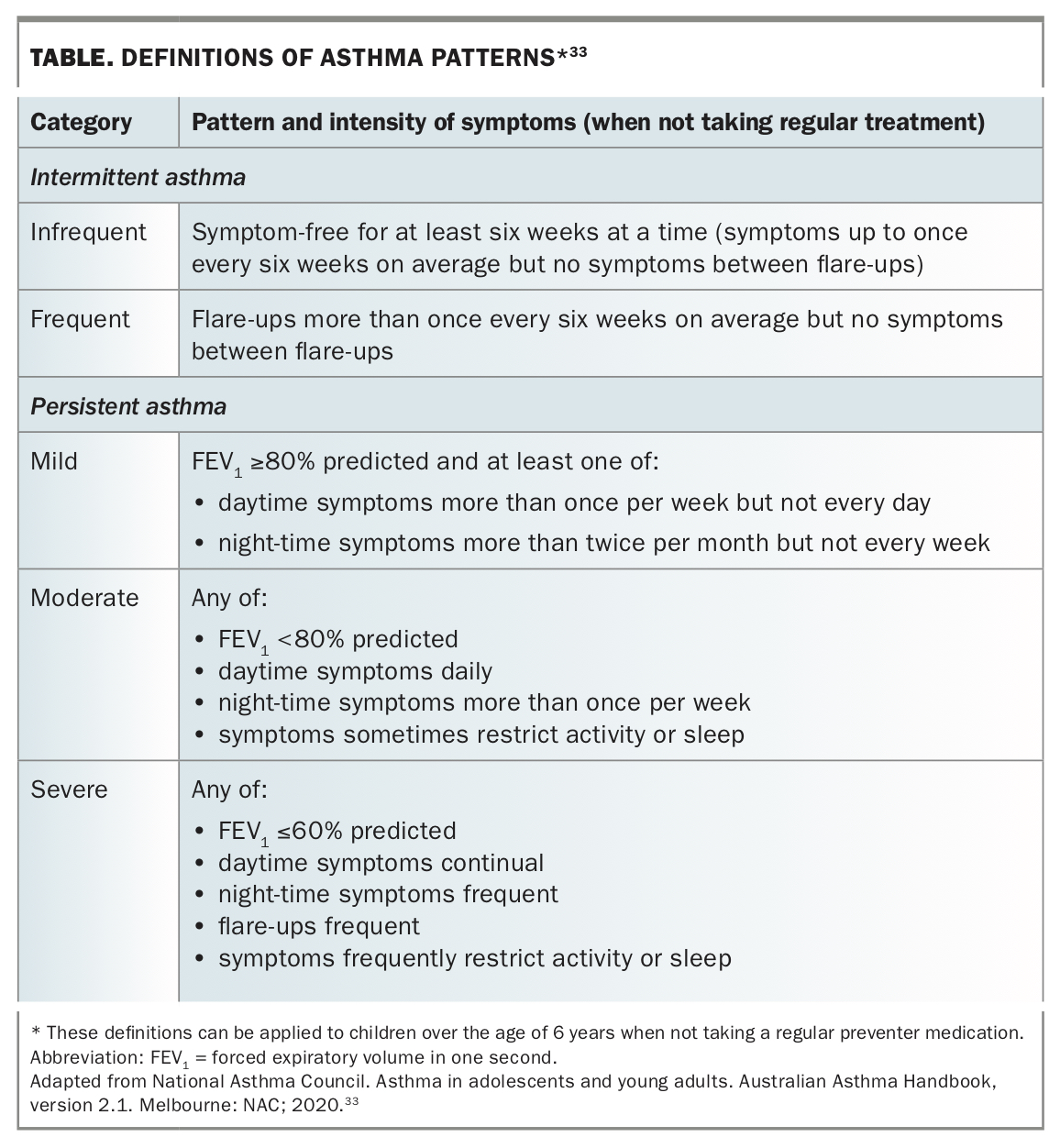
- Asthma is classified according to frequency and persistence of symptoms. When selecting initial and subsequent preventer medications consider the young person’s pattern of asthma, risk factors and comorbidities (Figure)5
- Before stepping up therapy, revisit the diagnosis, check symptoms are due to asthma, inhaler technique is correct and adherence is adequate
- Monitor and adjust therapy to maintain good control at the lowest effective dose of preventer medications. When asthma is stable and well controlled for at least three months, consider stepping down the dose
- Combination therapy medications (inhaled corticosteroids plus long-acting beta agonists [ICS/LABA]) have been proposed as an option for some adolescents when starting treatment (Figure);5 however, data in this age group is limited
- Low-dose budesonide/eformoterol combination can be prescribed at a fixed maintenance dose with a short-acting beta agonist (SABA) as reliever therapy or as single maintenance and reliever therapy (SMART regimen) for adolescents aged 12 years and over. SMART therapy AAPs give adolescents with good symptom perception the option to titrate medication when they feel their asthma is worsening (Table)33
- The pharmacological approach to treating allergic rhinitis usually consists of treatment with antihistamines, oral leukotriene antagonists (advise the family about potential adverse neuropsychiatric effects of montelukast in young people) and intranasal corticosteroids, the last being the most efficacious. Intranasal corticosteroids, often first-line treatment, are effective in reducing congestion, itching, rhinorrhoea, sneezing and ocular symptoms for adolescents with allergic rhinitis12
- During bushfire season and periods of heavy air pollution, advise young people at high risk to stay indoors with windows and doors closed and reduce strenuous physical exercise.26 Consider stepping up preventer therapy (e.g. corticosteroid dose) early if symptoms or exacerbations increase and if living in bushfire-prone areas. Update AAPs, reinforce adherence and emphasise the importance of always carrying their reliever inhaler
{kind=link}
{kind=link}
Support
- Refer adolescents (and parents and carers) early for smoking cessation and provide opportunistic brief interventions at every episode
- Offer concurrent psychological support for adolescents who express feelings of hopelessness, anxiety or depression
- Recommend patients to peer-led programs in which adolescents are trained to teach their peers about asthma self-management. Peer-led programs have consistently been shown to improve health-related quality of life measures34,35
- Family support and education is needed to help parents and carers look after their adolescent with a chronic condition. This is important not only to reinforce treatment routines but also to facilitate school, social and peer interactions36
- Community asthma educators provide invaluable self-management support, education and training and can be accessed directly through Asthma Australia (Box 3)
Digital health technologies37
- Adolescents and young people are tech savvy and expect us to be too. A variety of digital health apps and resources are listed in Box 3
- Multiple randomised controlled trials have demonstrated that web-based interventions (e.g. e-learning modules, AAP generators, medication lists, symptom diaries, online videos) are particularly effective in improving asthma scores and symptom-free days
- Digital health apps have also been shown to improve both asthma control and adherence to treatment in adolescents
- Text messaging and phone call reminders are effective in improving follow-up rates and appointment attendance
Transition
Transition to adult care is an important consideration, especially for young people with complex asthma who are engaged with specialist paediatric services. GPs play an important role in transition planning, which incorporates re-education, self-management promotion and self-advocacy. Later in adolescence, it is helpful to establish an individual transition plan with early referrals made to appropriate adult services to ensure that the young person does not fall through the gaps.
Conclusion
All asthma deaths are preventable and although the overall number has dropped considerably over the past several years in Australia, there has been little change in the rate of mortality due to asthma in the 5- to 34-year-old age group.1 Consequently, adolescence offers an important opportunity for intervention with early referral to specialist multidisciplinary services indicated when the diagnosis of asthma remains uncertain, symptoms are inconsistent or uncontrolled, significant comorbidities exist and lung function testing does not demonstrate variable airflow limitation.
Our understanding and treatment options of ‘difficult’ or ‘therapy-resistant’ asthma have made considerable advances recently and a new era of immunotherapy and biologics (e.g. omalizumab, benralizumab) offers hope for a subset of adolescents with complex asthma. However, for the most part, early recognition, regular monitoring and psychosocial support offer the greatest opportunity to give our young people the best start in life.
Adolescence is a critical period in development, maturation and identity formation when opportunistic interventions and therapy planning may be especially beneficial.
For adolescents with asthma, as with other chronic conditions, the role of the GP is crucial in maintaining good physical health, identifying risk factors that may contribute to poor control and recognising the developmental and psychosocial factors that affect their long-term outcomes. MT