COVID-19 in the gut and liver

Infectious diseases

Coronavirus disease 2019 (COVID-19) is known to result in gastrointestinal symptoms and liver damage. Consideration needs to be given to COVID-19 as a potential cause of new-onset gastrointestinal symptoms. Awareness of special issues affecting patients with chronic gastrointestinal and liver diseases in a pandemic is important.
Respiratory symptoms are the classic symptoms of coronavirus disease 2019 (COVID-19), but some people with COVID-19 can experience gastrointestinal symptoms such as diarrhoea, nausea and vomiting without any respiratory symptoms.1 Faecal swab and intestinal biopsy specimens from patients with COVID-19 have tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) nucleic acid, confirming active viral replication in the gastrointestinal tract.2 SARS-CoV-2 has been isolated from the stool samples of patients with COVID-19, indicating the possibility of faecal-oral transmission.3
The liver can be affected in COVID-19. It is recognised that abnormal liver enzyme levels are common in patients with COVID-19 and correlate with the severity of illness.4
The Gastroenterological Society of Australia (GESA) COVID-19 guidelines on inflammatory bowel disease (IBD), liver diseases and endoscopy were published in 2020 and made appropriate recommendations for management during the pandemic.5-7 This review of COVID-19 in the gut and liver emphasises issues relevant to primary care.
Mechanism of SARS-COV-2 infection and the gut
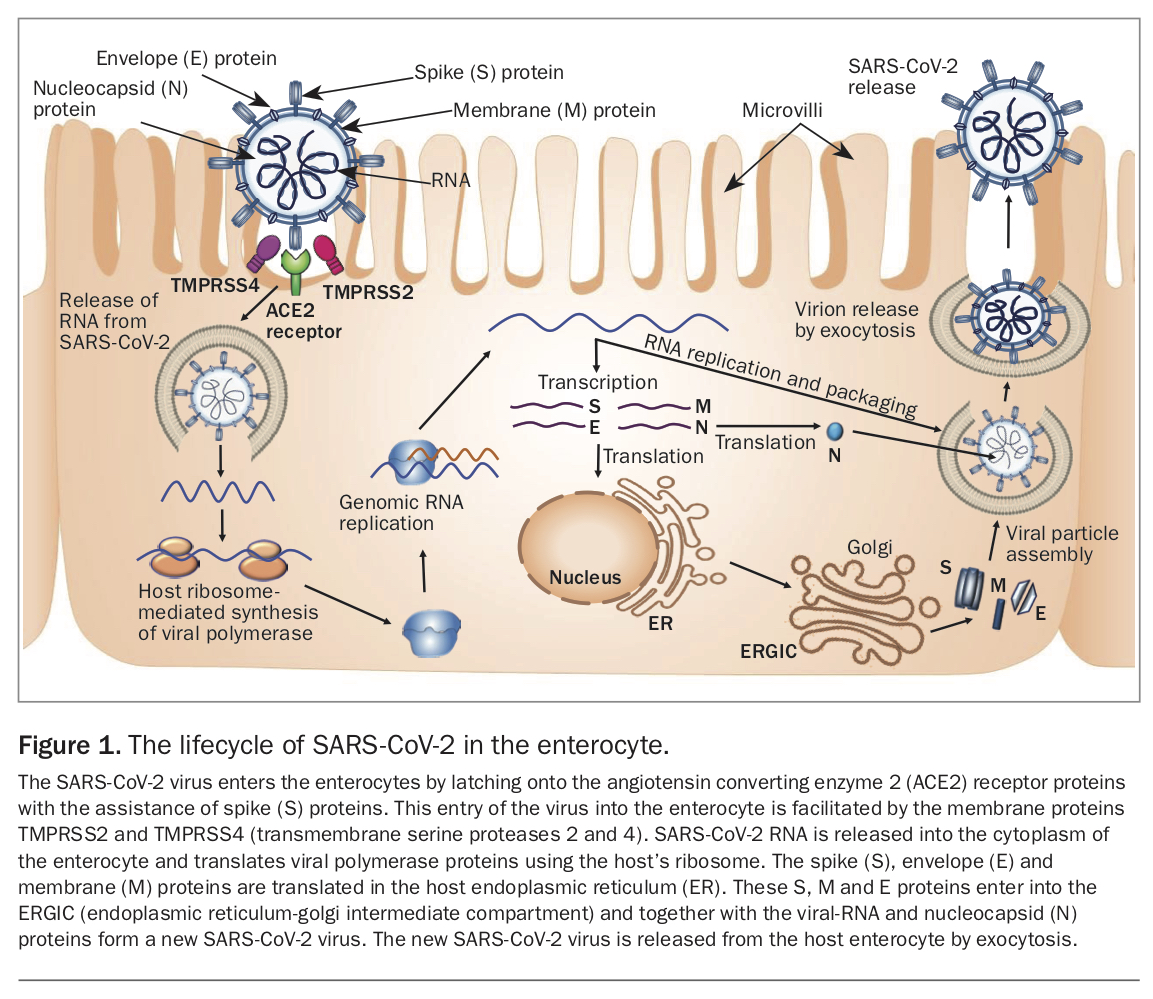
SARS-CoV-2, the virus that causes COVID-19, enters cells by latching onto protein receptors called angiotensin converting enzyme 2 (ACE2) receptors (Figure 1). These receptors are found in respiratory cells but are also highly expressed in the cells lining the oesophagus and the enterocytes of the ileum and colon.8 Two other proteins found in the membranes of cells, transmembrane serine proteases 2 and 4 (TMPRSS2 and TMPRSS4), help to promote SARS-CoV-2 infection of enterocytes.9 The mechanism by which SARS-CoV-2 does damage to the gastrointestinal tract is not fully understood.
{kind=link}
Gastrointestinal implications of COVID-19
What is clear is that COVID-19 can result in gastrointestinal symptoms. One in six people hospitalised with COVID-19 may show only gastrointestinal symptoms at presentation.10 Gastrointestinal symptoms appear to be common, with one review of more than 25,000 patients with COVID-19 finding that about 18% had gastrointestinal symptoms before or at the same time as onset of respiratory symptoms.11 The most common symptom was diarrhoea, the next nausea, and vomiting was the third most common. Abdominal pain is considered rare. In some studies, diarrhoea affected one in three people hospitalised with COVID-19.12,13
Critically ill patients with COVID-19 have a higher rate of gastrointestinal symptoms than critically ill patients without COVID-19, but it does not appear that there is an increased mortality from COVID-19 for patients with gastrointestinal symptoms.14-16
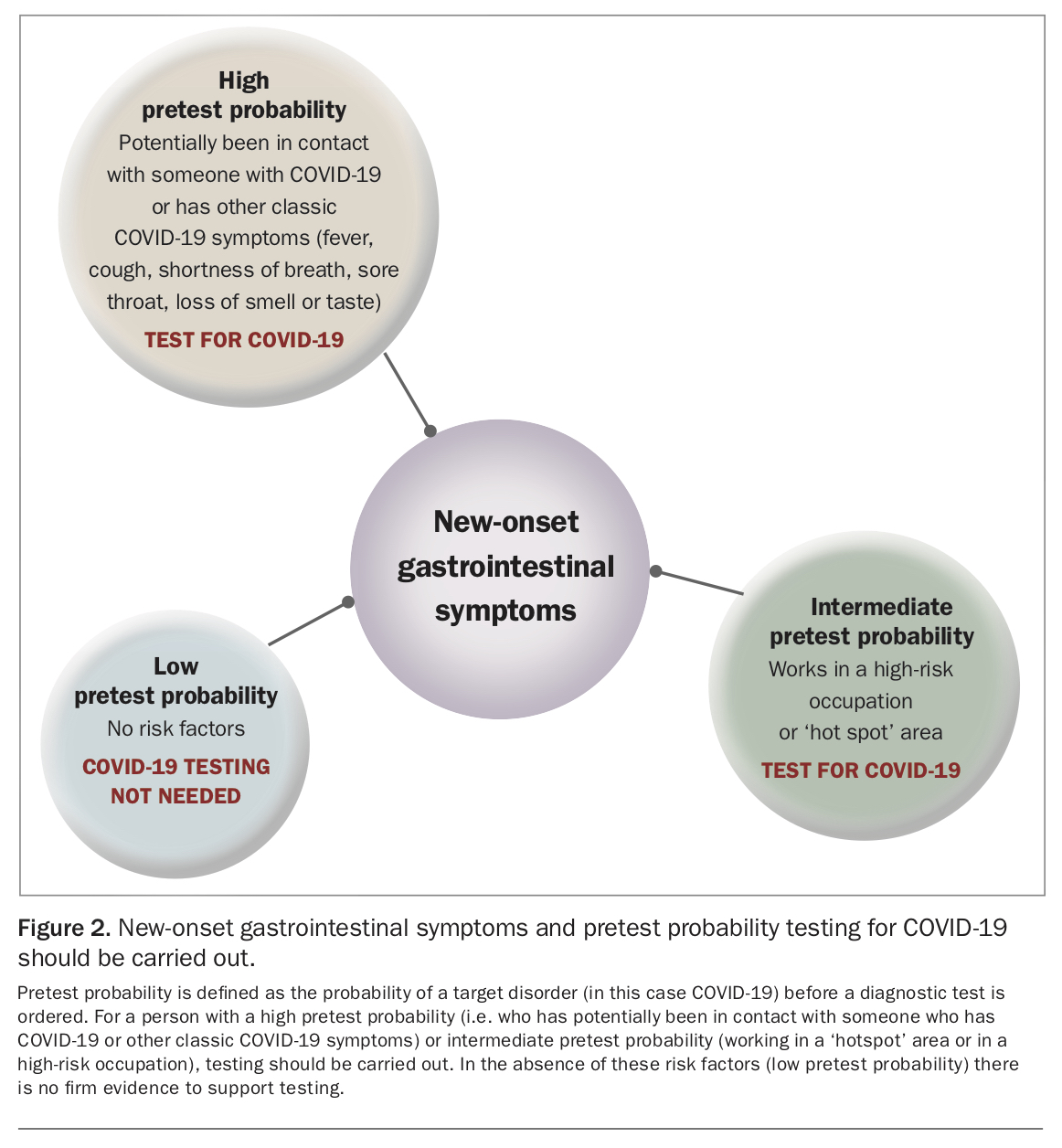
Gastrointestinal symptoms such as diarrhoea can occur earlier than classic respiratory symptoms and fever in patients with COVID-19. In a single-centre Chinese cohort of 138 patients with COVID-19, just over 10% had diarrhoea and nausea symptoms one to two days before developing fever and dyspnoea.17 Given that patients with COVID-19 can present with gastrointestinal symptoms earlier than classic respiratory symptoms or with gastrointestinal symptoms alone, the pretest probability needs to be canvassed before deciding on testing for COVID-19 for new-onset gastrointestinal symptoms.
COVID-19 testing in Australia is free of charge and covered under Medicare. Testing is strongly encouraged in anyone with new-onset respiratory symptoms, unexplained fever or loss of smell or taste that may reflect COVID-19 infection. In addition, a diagnosis of COVID-19 should be considered in a person with new-onset unexplained gastrointestinal symptoms, and there should be a low threshold for testing (Figure 2).
{kind=link}
Persistent viral faecal shedding has been reported for COVID-19. One study in China followed 74 patients hospitalised with COVID-19 by taking throat swabs and faecal samples daily or every second day.18 The researchers found that in over half of these patients faecal samples remained positive for SARS-CoV-2 viral RNA for an average of just over 11 days after their throat swabs tested negative. Viral RNA was still detected in one patient’s faeces 33 days after their throat swab test result had turned negative.
This suggests the virus still actively replicates in the patient’s gastrointestinal tract long after the virus has cleared from the respiratory tract. This active shedding of virus into faeces does not mean, however, that the person is necessarily contagious. The detection of SARS-CoV-2 nucleic acid in sewage is useful as an alert for the possibility of a community outbreak, and sewage surveillance programmes are important in the public health response to the pandemic. It must be noted that the presence of nucleic acid in sewage indicates that virus at some point has been shed in stool and does not confirm the presence of live virus.19
The presence of viral RNA in stool does raise the possibility of faecal-oral transmission. This prospect is strengthened by the finding of live virus in faecal culture.3,20 However, even if this mode of transmission does exist, the likelihood of SARS-CoV-2 being transmitted by faeces from one person to another is considered to be very low.21 Faecal-oral transmission therefore is not currently considered a major route in the spread of COVID-19.
Pre-existing gastrointestinal diseases and COVID-19
There are some special considerations for existing gastrointestinal conditions in the context of the COVID pandemic.5,7,22-28
- There is no evidence that gastrointestinal disease or IBD increase the risk of SARS-CoV-2 infection.
- The clinical presentation of some chronic gastrointestinal diseases such as IBD can mimic a gastrointestinal presentation of COVID-19 and therefore clinicians will need to assess whether symptoms are related to a diseases flare or COVID-19. As COVID-19 testing is readily available in Australia, there should be a low threshold for recommending a test.
- In patients with IBD who are exposed to COVID-19, immunomodulatory and biologic medications should generally not be ceased without careful consideration of the risk of disease flare. Patients on corticosteroids for IBD may be at increased risk of severe COVID-19 and should follow all guidelines to limit their risk of exposure.
- If a patient with IBD develops COVID-19, the severity of COVID-19 and the severity of the IBD need to be taken into account in making decisions about continuing or ceasing medications. In general, if a patient with quiescent IBD develops COVID-19, IBD medications can be temporarily withheld for at least two weeks and recommenced with the timing of recommencement contingent on the severity of COVID-19 and baseline IBD disease.
- Triaging guidelines for endoscopy (GESA) should be followed if restrictions to nonurgent procedures are reintroduced because of increasing numbers of COVID-19 cases.
- Bowel cancer screening should not be delayed because of the COVID-19 pandemic.
- SARS-CoV-2 is completely inactivated and incapable of infecting cells in a low pH environment (pH 1 to 2). Taking an acid suppressing medication such as a proton pump inhibitor (PPI) for a long period of time can increase a person’s risk of severe clinical outcomes from COVID-19 but does not increase their susceptibility to SARS-CoV-2 infection. People taking histamine-2 receptor antagonists have not been shown to be at increased risk of severe clinical outcomes from COVID-19. PPIs should be used judiciously in accordance with national guidance on appropriate prescribing and, ideally, substituted with histamine-2 receptor antagonists when possible. It is appropriate to continue with a PPI if there is a strong medical indication, such as for healing of a bleeding peptic ulcer.
- The risks of SARS-CoV-2 vaccination in patients with gastrointestinal diseases are anticipated to be very low, and vaccination is strongly recommended.
- The precise timing of vaccination should be decided by discussing with the patient the risks and benefits of any proposed delay. For example, a short course of high-dose corticosteroids for an IBD flare can impact on vaccine efficacy, and it may be reasonable to delay vaccination until patients have tapered down or stopped taking their corticosteroids.
Mechanisms of SARS-COV-2 infection and the liver
The precise mechanism for liver injury during SARS-CoV-2 infection has not been determined. Current evidence indicates COVID-19-associated liver injury results from a multifactorial attack including drug-induced liver injury, systemic inflammatory reaction and hypoxia-ischaemia reperfusion liver injury in addition to possible direct injury to the liver by SARS-CoV-2.
ACE2 receptors are specifically expressed in the cells lining the bile duct and are 20 times more prevalent there than in hepatocytes.29 One proposed reason for liver injury with SARS-CoV-2 is that there may be upregulation of ACE2 receptors in liver tissue caused by the proliferation of liver cells derived from bile duct cells, making entry of the virus into the liver more likely and subsequently causing damage.
A postmortem examination of the liver of a 50-year-old man with COVID-19 found moderate microvesicular steatosis and mild lobular activity, which are considered nonspecific changes.30 It is uncertain, though, whether the effects were due to the virus or to the effects of drugs that the patient was taking. Some of the latest drug treatments for COVID-19 can result in liver injury. Raised liver enzyme levels were measured in 10 to 13% of a remdesivir-treated group in a recent randomised controlled trial.31
Implications of COVID-19 for the liver
When people are infected with SARS-CoV-2, typically they have mild to moderately elevated alanine aminotransferase (ALT) and/or aspartate aminotransferase (AST) levels in the early stages of the disease, accompanied by a slight increase in bilirubin levels.32 In a US cohort study of 5700 patients hospitalised with COVID-19, abnormal ALT levels were shown in 39.0% of patients and abnormal AST levels in 58.4%.33 These elevated liver enzymes largely resolve as the patient recovers from COVID-19.4
In another study, liver enzyme derangement was significantly higher in critically ill patients and was associated with poor outcomes.34 In these patients the liver dysfunction may be predominantly due to drug-induced or sepsis/shock-related liver injury.
Pre-existing liver diseases and COVID-19
There are some special considerations for existing liver conditions in the context of the COVID pandemic.6,22,35-39
- Patients with liver disease are not at increased risk of infection with COVID-19.
- Patients with cirrhosis are at increased risk of developing severe COVID-19 and subsequent complications, including mortality. Mortality of 30 to 32% in patients with cirrhosis and COVID-19 infection has been reported. Mortality was no higher among patients hospitalised with cirrhosis and COVID-19 than it was among those hospitalised with cirrhosis complications without COVID-19.
- Intensive telehealth surveillance has been shown to be a feasible option for providing care to patients with chronic liver disease during a pandemic and reducing their risk of contracting COVID-19.
- Patients with chronic liver diseases including hepatitis B, hepatitis C and autoimmune hepatitis need to continue their usual outpatient medication regimen. The risk of disease flare from ceasing medications outweighs the risk of contracting COVID-19.
- There is increased concern regarding relapse into alcohol use among patients with alcohol-related liver disease during a period of isolation, and vigilance is required.
- Patients with hepatocellular cancer should continue with their treatment uninterrupted, as any disruption can worsen outcomes.
- The risks of SARS-CoV-2 vaccination in patients with liver diseases are anticipated to be very low, and vaccination is strongly recommended.
- The precise timing of vaccination should be decided by discussing with the patient the risks and benefits of any proposed delay. For example, a short course of high-dose corticosteroids for an autoimmune hepatitis flare can impact on vaccine efficacy, and it may be reasonable to delay vaccination until patients have tapered down or stopped taking their corticosteroids.
Conclusion
Australia has performed better at managing the COVID-19 pandemic than many other countries with comparable populations and geographies. That being said, COVID-19 is likely to be with us for several years notwithstanding the success of vaccines. As such, it is important to be cognisant of the nature of multiorgan involvement with COVID-19 and the ensuing sequelae for patients. The gastrointestinal tract and liver are known to be affected in COVID-19. Gastrointestinal symptoms such as diarrhoea, nausea and vomiting are common and may be the only clinical manifestation of COVID-19. A high index of suspicion should be maintained for new-onset gastrointestinal symptoms as attributable to COVID-19 if there is high to intermediate pretest probability. As COVID-19 testing is readily available in Australia, there should be a low threshold for recommending a test.
Liver enzyme abnormality is very likely to be multifactorial, and mildly elevated transaminase levels are common. Liver enzyme abnormalities resolve in most cases. However, people with cirrhosis who contract COVID-19 are at a markedly increased risk of death and all reasonable efforts should be made to reduce their exposure to COVID-19.
During a pandemic, patients with gastrointestinal and liver diseases generally should not have their medications discontinued without careful consideration of the risk of a disease flare. Special consideration applies to patients on corticosteroids (e.g. for IBD) as they may be at increased risk of severe COVID-19. These patients should be advised to follow all guidelines to limit their risk of exposure, acknowledging that this is still an evolving area where more data are emerging.
Real world data are also being collected on vaccine responses in immunocompromised patients. It is recommended that all patients with gastrointestinal and liver disease receive SARS-CoV-2 vaccination regardless of comorbidity, as the benefits are considered to greatly outweigh the risks. MT