New targeted therapies for rheumatoid arthritis

Better understanding of the pathophysiology of rheumatoid arthritis has led to the development of targeted biologic and small molecule (synthetic) disease-modifying antirheumatic drugs (DMARDs), including the janus kinase inhibitors.
Rheumatoid arthritis (RA) is the most common form of inflammatory arthritis, affecting around 1.9% of Australians.1 RA is characterised by polyarthritis, causing pain, irreversible joint damage and disability if left untreated. Treatment aims not just to improve symptoms but to induce remission or control inflammation to prevent joint injury and disability.
The aetiology of RA is unknown; however, tumour necrosis factor (TNF), interleukin-1 (IL-1) and interleukin-6 (IL-6) appear to be the most abundant cytokines involved. This knowledge has led to the development of targeted therapies that have revolutionised the management of RA.
The early use of disease-modifying antirheumatic drugs (DMARDs) results in better outcomes and a lower risk of refractory disease.2-6 The mainstay of treatment continues to be the conventional synthetic DMARDs (csDMARDs), which include methotrexate, leflunomide and sulfasalazine. However, since the late 1990s, the addition of targeted biological agents, such as the TNF inhibitors, to csDMARDs has provided treatment options for patients with demonstrated inadequate disease control. More recently, targeted small molecule (synthetic) agents, the janus kinase (JAK) inhibitors, have provided further benefit for the up to 30% of patients who continue to have inadequate disease control with targeted biological agents.7 All these agents have also been found useful in patients with other inflammatory diseases, including different inflammatory arthritides.
Targeted therapies require specialist provision, but it is important that all clinicians have some understanding of their increasing role in the management of patients with RA. Here we summarise the role of targeted biologic and small molecule (synthetic) DMARDs in RA.
When is targeted therapy considered?
Targeted DMARD therapy needs to be considered if a patient with RA fails to achieve disease control or remission within three to six months of treatment with csDMARDs. All targeted therapy has greater efficacy when combined with csDMARDs, and treatment guidelines therefore recommend combination therapy.8-11 Methotrexate is often used as the ‘anchor’ drug, following trials demonstrating a faster onset of action, comparable or greater efficacy, better long-term tolerance and improved survival compared with other conventional DMARDs.12,13 Methotrexate also inhibits the development of antibodies directed at biologic agents that reduce their efficacy, thereby strengthening the case for methotrexate to be used in combination with targeted DMARDs.
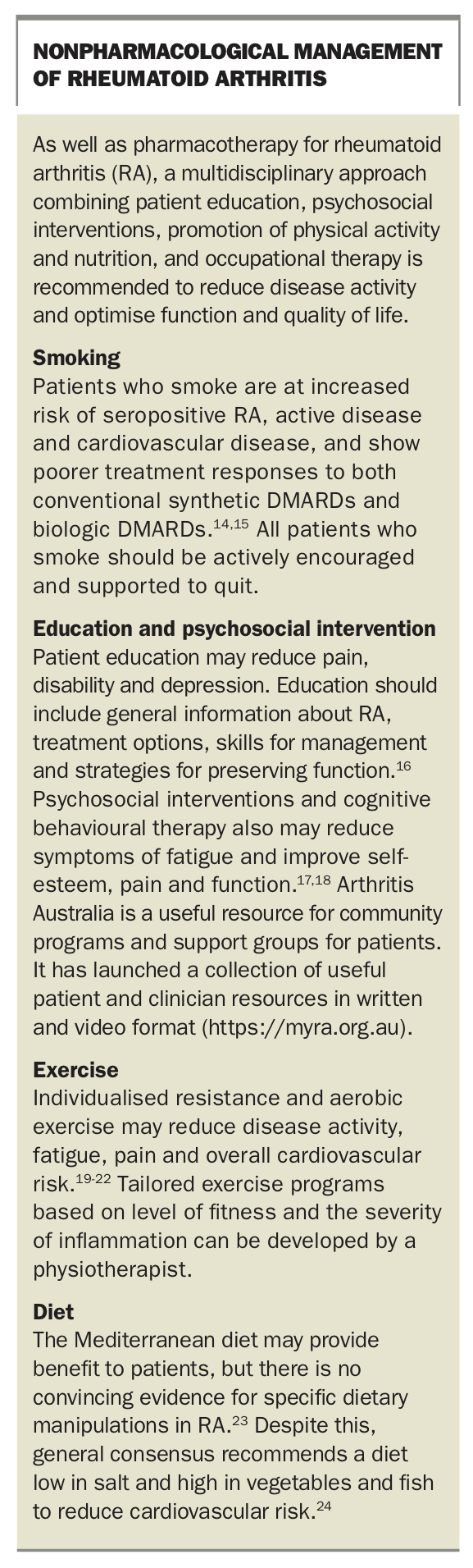
Nonpharmacological management is also important in reducing disease activity and optimising function and quality of life in patients with RA, including those receiving DMARDs. A multidisciplinary approach focusing on patient education, psychosocial interventions, physical activity, nutrition and occupational therapy is recommended (Box).14-24
{kind=link}
Biologic DMARDs
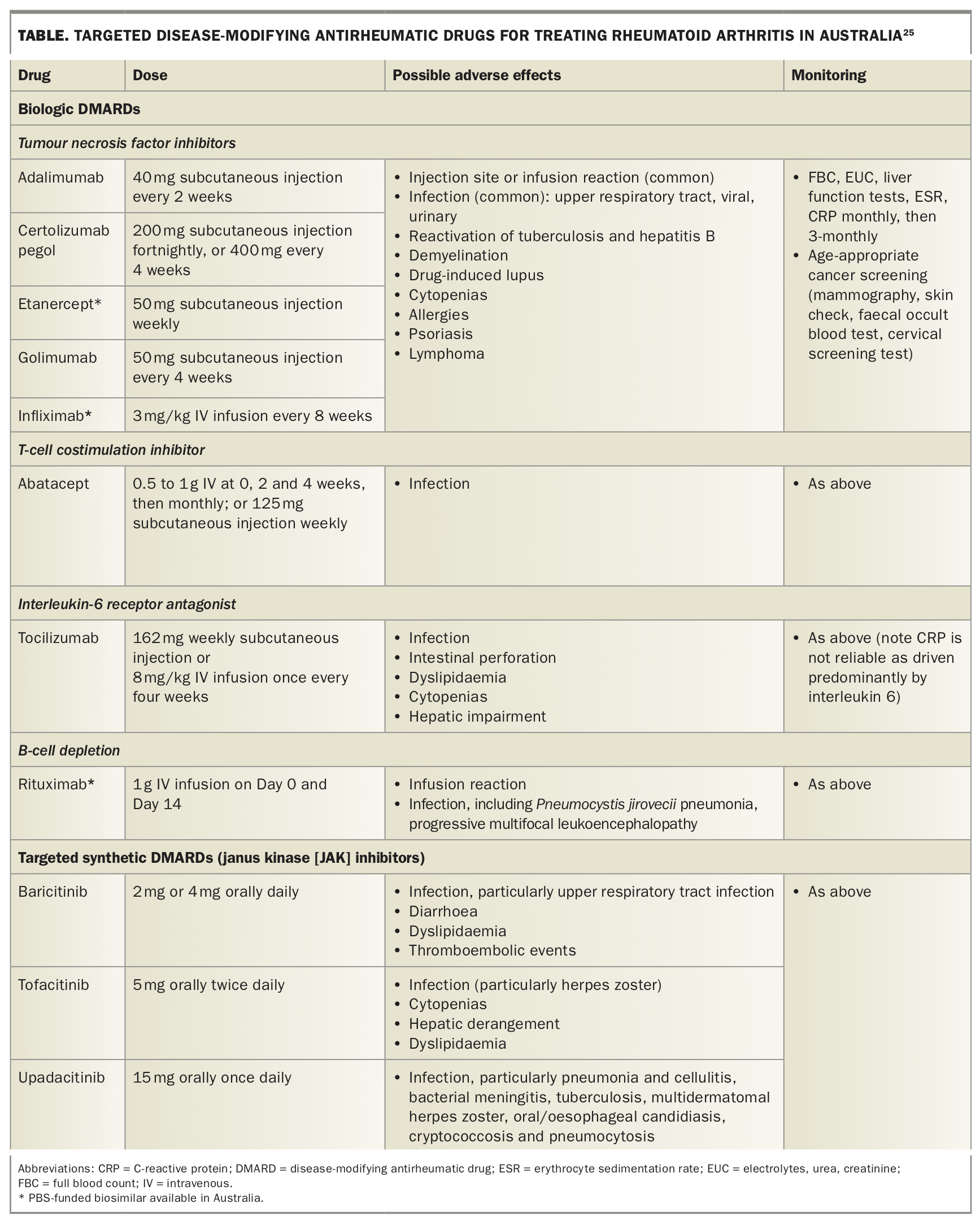
Biologic DMARDs are antibodies that target inflammatory pathways involved in the pathophysiology of RA. Eight biologic DMARDs are currently subsidised by the PBS for the treatment of RA (Table).25 They target TNF, IL-1, IL-6, B-lymphocyte CD20 receptors and T cells. All biologics are injectables, administered either subcutaneously or by infusion.
{kind=link}
Biosimilars
In 2015-16, the cost of RA to the Australian healthcare system was about $1.2 billion, representing 1% of total disease expenditure.26 Targeted DMARDs have contributed to a large proportion of this cost. Now with patents expiring, biosimilars are emerging and have the potential to reduce treatment costs significantly. Unlike small synthetic agents, biologic agents are large complex molecules and cannot be copied identically to create generics. A biosimilar is a biologic that is highly similar, but not identical, to a reference biologic drug. Despite a theoretical risk of increased immunogenicity, the overall consensus is that biosimilars are sufficiently equivalent in efficacy and safety to their reference biologic as to allow for a single switch from the reference biologic to a biosimilar, although the safety of multiple switches is less certain.27 PBS-funded biosimilars are currently available in Australia for several TNF inhibitors and for rituximab.
Targeted synthetic DMARDs
The most recent advance in RA treatment has been the development of the JAK inhibitors. The first of these agents, tofacitinib, was listed on the PBS in 2015. Since then, two other JAK inhibitors, baricitinib and upadacitinib, have become available (Table).25 Others are in the later stages of development.
JAK inhibitors are small synthetic agents that block intracellular signalling of inflammatory cytokines, activation of lymphocytes, and ultimately inflammatory pathways that normally result in joint destruction. In contrast to biologic agents, JAK inhibitors are administered orally and lack the potential to generate antidrug antibodies.
Similarly to biologic DMARDs, contraindications to JAK inhibitors include severe infections, active tuberculosis, neutropenia (neutrophil count less than 1.0 x 109 cells/L) and severe liver impairment. The safety of the targeted synthetic DMARDs during pregnancy is unclear, and thus patients who are pregnant or planning pregnancy need ongoing specialist input.
Which targeted therapy?
With the rapid evolution of treatment options for RA, choosing the ‘correct’ agent to optimise treatment success has become more challenging. Research has failed to identify clinical or biological markers that would enable individual responsiveness to a particular targeted therapy to be predicted. There is some evidence that the JAK inhibitors may be effective as monotherapy, although they have higher efficacy when prescribed in combination with methotrexate.28,29 There is even some suggestion that they have potential superior efficacy over biologics in some contexts.30-32
Therapy choice depends mostly on PBS criteria, specialist experience and acceptability of the route of administration to the individual patient. However, some disease characteristics and comorbidities help direct treatment choice.
- Rituximab and abatacept may be more efficacious in patients who are seropositive (i.e. with antibodies to rheumatoid factor and/or anticyclic citrullinated peptides [anti-CCP]).33-35
- For patients who show an inadequate initial response to anti-TNF therapy, meta-analyses suggest that agents with alternative mechanisms of action are more likely to be efficacious, although other anti-TNF agents may still lead to benefit.36
- Comorbid interstitial lung disease and chronic obstructive lung disease are not uncommon. TNF inhibitors have been reported to have possible pulmonary complications, and may best be avoided in the first instance in patients with severe lung disease.37
- Rituximab, also previously avoided in patients with severe lung disease, has now been shown to stabilise symptoms and lung function in patients with interstitial lung disease.38
Despite these differences, the likelihood of efficacy is largely indistinguishable between targeted agents. Individual biologic and targeted synthetic DMARDs remain of equal standing in treatment guidelines as options in patients with inadequate disease control on conventional DMARDs.
Pretreatment evaluation
Before initiating therapy, all patients should have baseline blood tests, including a full blood examination and measurement of serum creatinine and liver enzyme levels. Patients should also be screened for latent or chronic infections such as hepatitis B, hepatitis C, HIV infection and tuberculosis. Pregnancy, lactation, malignancy and other medical comorbidities are further important considerations before the initiation of therapy. Notably, certolizumab has been shown to lack placental transfer, and biologic DMARDs are not effectively absorbed by breastfeeding children, although targeted synthetic DMARDs may be absorbed.39,40
Adverse effects and management concerns
Infection
Cytokines involved in inflammation play an important role in protecting against infection. All targeted therapies increase the risk of infection. Symptoms and signs are often absent, emphasising the need for medical practitioners to remain alert to the possibility of both common and opportunistic infections in patients receiving targeted therapies.
Rates of serious infection are comparable between biologic and targeted synthetic DMARDs, with the exception of herpes zoster, which occurs more often with targeted synthetic DMARDS.4,5 The rates of serious infection are increased in patients with lymphopenia, emphasising the importance of monitoring lymphocyte counts.41
Rates of reactivation of latent tuberculosis and other opportunistic infections appear higher in patients receiving targeted therapies compared with the general population.41 The risk of tuberculosis reactivation appears greatest with monoclonal antibody TNF inhibitors (e.g. infliximab and adalimumab, but not etanercept).42-45 It remains unclear whether the JAK inhibitors carry a similar risk.
Vaccination
Patients with RA are recommended to have annual influenza vaccination, as they are at increased risk of complications, and to be up to date with pneumococcal vaccination. Although live vaccines such as the zoster, measles, mumps and rubella, and yellow fever vaccines are strictly contraindicated in patients receiving biologic or targeted synthetic DMARDs, inadvertent dosing has not shown any infective complications.46,47
Malignancy
Patients with RA are at increased risk of lung and lymphoma malignancies compared with the general population.48 Aside from an increased risk of nonmelanoma skin cancers, particularly with TNF inhibitors, biologic and targeted synthetic DMARDs do not appear to increase the risk of malignancy.49 Regular six to 12-monthly skin checks and age-appropriate malignancy screening are recommended. Ongoing longer term data are required to further evaluate malignancy risk.
Thrombotic complications
Patients with RA have an increased background risk of thromboembolic complications. JAK inhibitors may contribute to a small increase in this risk, but further confirmation and quantification are required.50,51
The future of targeted therapy
The future role of targeted therapies, especially JAK inhibitors, in Australia as initial or monotherapy in RA is unclear. With longer term data, greater clinical experience, the availability of biosimilar drugs and the development of precision medicine, this will likely change. Nevertheless, around 20% of patients with RA continue to have refractory disease despite targeted therapies, and further therapeutic developments are needed.52,53
Conclusion
RA is a chronic, inflammatory disease capable of causing joint destruction, pain and disability. Early diagnosis and treatment are essential to avoid complications. Optimal management involves a multidisciplinary approach, with nonpharmacological as well as pharmacological therapies. Over the past three decades, better understanding of the pathophysiology of RA has led to improved targeted therapies, including biologic DMARDs and, more recently, the JAK inhibitors. Knowledge of their relative benefits will facilitate their best use. MT