Irritable bowel syndrome: an update on diagnosis and management

Dr Ko is a Gastroenterology Advanced Trainee at Campbelltown and Camden Hospital and PhD candidate in the School of Medicine, Western Sydney University, Sydney.
Dr Ho is a Senior Lecturer in Medicine and a Gastroenterologist at Western Sydney University, Sydney, NSW.
Irritable bowel syndrome
Digestive diseases
Irritable bowel syndrome (IBS) is a common chronic relapsing disorder. A positive diagnosis, in conjunction with a multimodal approach to management, which includes dietary and lifestyle modifications as first-line treatment, followed by pharmacological and psychological therapies, engages and supports patients with IBS.
- The diagnosis of irritable bowel syndrome (IBS) can be made using the ROME IV criteria and subtyped based on predominant symptoms.
- Clinicians should focus on providing a positive diagnosis of IBS rather than a diagnosis of exclusion. A positive diagnosis enables early introduction of therapy and rationalisation of investigations.
- Simple noninvasive testing for serum inflammatory markers, coeliac disease serology and faecal calprotectin level should be performed in patients with suspected IBS. Further tests are of low yield, with significant opportunity costs and economic burden.
- A multimodal treatment approach is preferred in patients with IBS, depending on the severity.
- Lifestyle and dietary modifications form the first-line treatment for IBS. Subsequent effective therapies include psychological and pharmacological options.
- Specialist referral should be considered if there is diagnostic uncertainty, lack of response to first-line therapies, or as per patient requests.
Irritable bowel syndrome (IBS) is a chronic, relapsing disorder that affects around one in nine people in Australia.1 Patients suffering from IBS have symptoms of abdominal pain related to defecation or a change in bowel habits. IBS can be a challenging gastrointestinal disorder to manage; pathophysiological mechanisms of gut-brain axis dysfunction, visceral hypersensitivity and exacerbations caused by psychological stress, gastrointestinal infections and the complex relationship between diet and gut microbiota have all been identified as having a role in the pathogenesis of IBS, thus necessitating multimodal management strategies in IBS treatment.2-5 This article summarises the latest recommendations from recently published updated guidelines from gastroenterological societies on diagnostic and management approaches to IBS.6,7
Diagnostic criteria for IBS and IBS subtypes
The ROME IV criteria provide diagnostic criteria for IBS, defined as recurrent abdominal pain at least one day a week with two or more of the following:
- related to defaecation
- associated with a change in stool frequency
- associated with a change in stool form (appearance).
These criteria must be present for three months, with symptom onset at least six months before diagnosis.7 However, it should be noted that functional bowel disorders can coexist, and thus a patient’s symptoms might overlap with other ROME IV criteria.
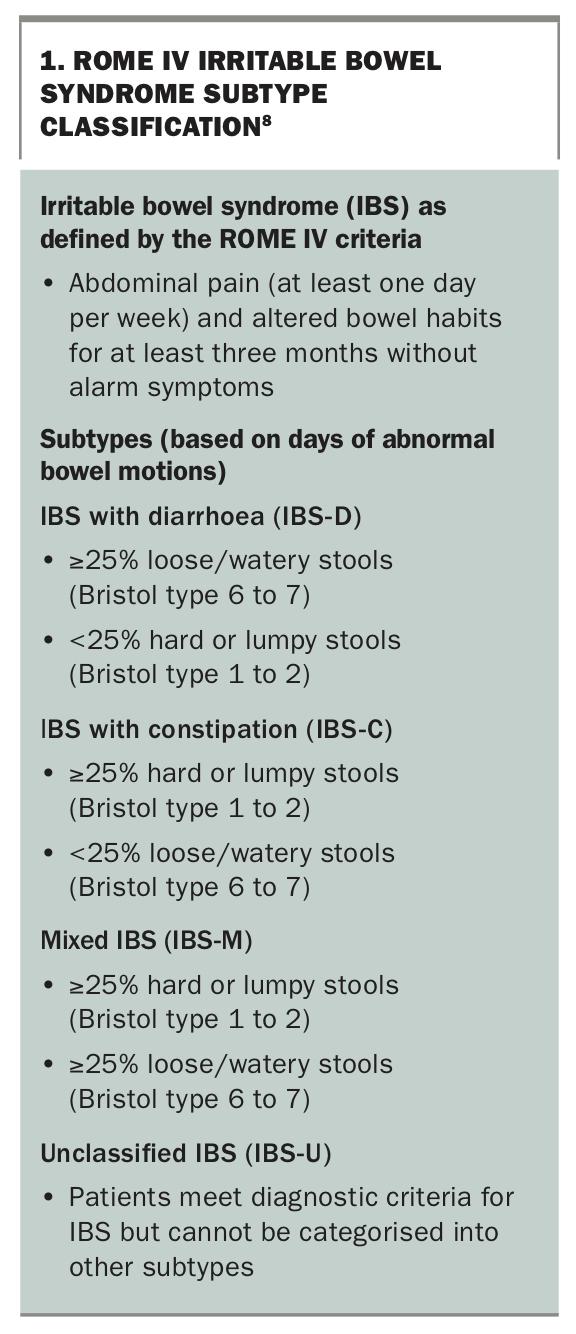
The ROME IV criteria further subtypes IBS into IBS with constipation (IBS-C), IBS with diarrhoea (IBS-D), mixed IBS (IBS-M) and unclassified IBS (IBS-U) (Box 1).8 A recent large international study on the prevalence of the different IBS subtypes found a similar prevalence for IBS-D, IBS-C and IBS-M at around 30% each and about 5% for IBS-U.8,9 It is important for clinicians to accurately classify patients with IBS into the appropriate subtype, as management of symptoms is influenced by the predominant IBS characteristic, while also empowering patients to identify their main troublesome IBS symptom to guide treatment goals.
{kind=link}
Additionally, it is important to consider a holistic approach to IBS management and address common associated disorders, which might worsen IBS symptoms. Patients with IBS frequently have associated conditions such as fibromyalgia chronic pelvic pain, chronic fatigue syndrome and temporomandibular joint disorder. They also have a higher prevalence of mental health disorders; up to half have depression, anxiety or self-identify as a hypochondriac.10,11
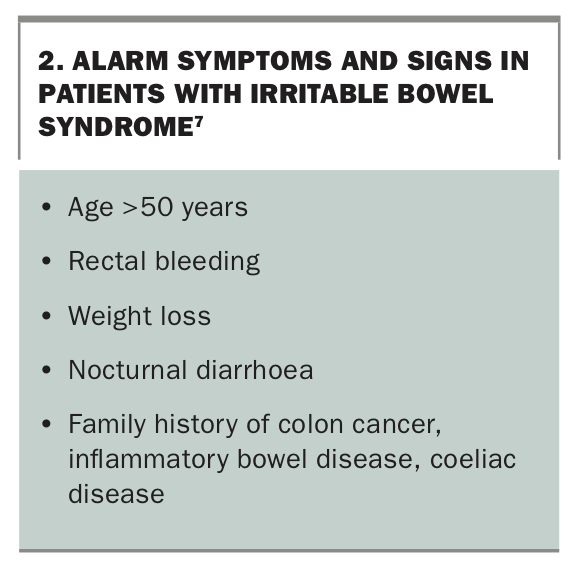
If patients fit the ROME IV criteria for IBS, careful history and examination to exclude the presence of alarm symptoms and signs (Box 2) should be undertaken. Patients with alarm symptoms and signs should be referred for specialist gastroenterologist review in a timely manner.
{kind=link}
Initial investigations
International guidelines and the Gastroenterological Society of Australia’s (GESA’s) IBS4GPs online treatment algorithm, recommend focusing on a positive diagnosis of IBS rather than treating IBS as a diagnosis of exclusion, as the latter approach can result in low diagnostic yield after extensive workup, with minimal impact on patient satisfaction.6,7,12 Investigations in a patient with suspected IBS should be rationalised and simple noninvasive tests used first. Younger patients with IBS (aged 16 to 45 years) tend to be overinvestigated, whereas older patients with a first presentation of IBS symptoms tend to be underinvestigated. The following outlines the recommended investigations in a patient fulfilling IBS criteria with no alarm symptoms.7,12
Initial blood and stool tests
Full blood count
All patients should have a full blood count performed. Evidence of anaemia or a raised white cell count should trigger consideration of alarm symptoms and other presentations.
Coeliac serology
Patients with coeliac disease may present with abdominal pain, bloating and/or changes in bowel habits, which is a similar clinical presentation to IBS. Patients with IBS symptoms should be screened for coeliac disease with antitissue transglutaminase IgG and IgA antibodies (sensitivity and specificity >90% in a patient without IgA deficiency).6,7,13,14
Inflammatory markers
C-reactive protein, a marker of inflammation, has good positive predictive value for inflammatory bowel disease (IBD) in patients with IBS symptoms, but poor negative predictive value.7 An abnormal C-reactive protein level should lead to consideration of referral for further investigations to exclude an inflammatory bowel aetiology for the patient’s presenting symptoms.7,14
Iron studies
Iron deficiency, particularly if associated with anaemia, should prompt referral to a gastroenterologist to exclude colorectal cancer and other gastrointestinal pathologies.6 GESA has published a helpful clinical update on assessment and management of iron deficiency.15
Stool testing – faecal calprotectin
A faecal calprotectin test is relatively simple and noninvasive, with excellent accuracy in excluding IBD. A normal faecal calprotectin level (<50 mcg/g) is associated with a less than 1% chance of a diagnosis of IBD in a patient with symptoms of IBS.7,13,16 This test is currently not Medicare rebatable, with an out-of-pocket cost for patients.
Low-yield investigations
Colonoscopy
A routine colonoscopy is not recommended as an initial investigation in patients younger than 45 years who have IBS symptoms without alarm features. It may be justified if alarm symptoms or signs are present, or in those with diarrhoea who have risk factors for microscopic colitis. If blood and stool test results are negative, the yield of identifying pathologies, such as IBD, microscopic colitis or colorectal malignancy, via colonoscopy is very low. Colonoscopies have significant patient morbidity (bowel preparation, time off work, anaesthetic risks, financial costs) and healthcare economic costs.17
Stool ova, cyst and parasite testing
Faecal testing for ova, cysts and parasites has a low yield in altering the diagnosis or management in patients with IBS, with the exception of patients who have risk factors for giardiasis, which includes exposure to water of poor quality, camping/hiking with exposure to unclean water, being in childcare settings, close contact with persons with giardiasis, swallowing water when in recreational water bodies, anal intercourse and traveling to endemic areas.7 There is no proven causative link between either Blastocystis or Dientamoeba fragilis infection and IBS pathogenesis. Therefore, routine testing for the presence of these gastrointestinal pathogens is not recommended due to uncertainty about the significance of the results in relation to patient symptoms.16,18
Food allergy testing
Routine testing for food allergies is not recommended. A true food allergy is diagnosed by a thorough medical history exploring symptoms of a reproducible reaction to food in conjunction with formal testing (e.g. skin prick test, IgE testing) by an immunologist. Overdiagnosing food allergy can adversely affect quality of life and nutrition, and studies have shown that between 50 and 90% of presumed food allergies are not true allergies.19
Thyroid function testing
Although commonly ordered in patients presenting with altered bowel habits, thyroid function tests rarely change the diagnostic or management outcomes of patients with IBS and, therefore, are not recommended as initial testing for IBS diagnosis.20
Breath testing
Hydrogen breath testing to exclude small intestinal bacterial overgrowth or lactose intolerance in patients with suspected IBS is not recommended due to previously reported high false-positive rates of this test in patients with IBS.6,21
Management of IBS
Approach
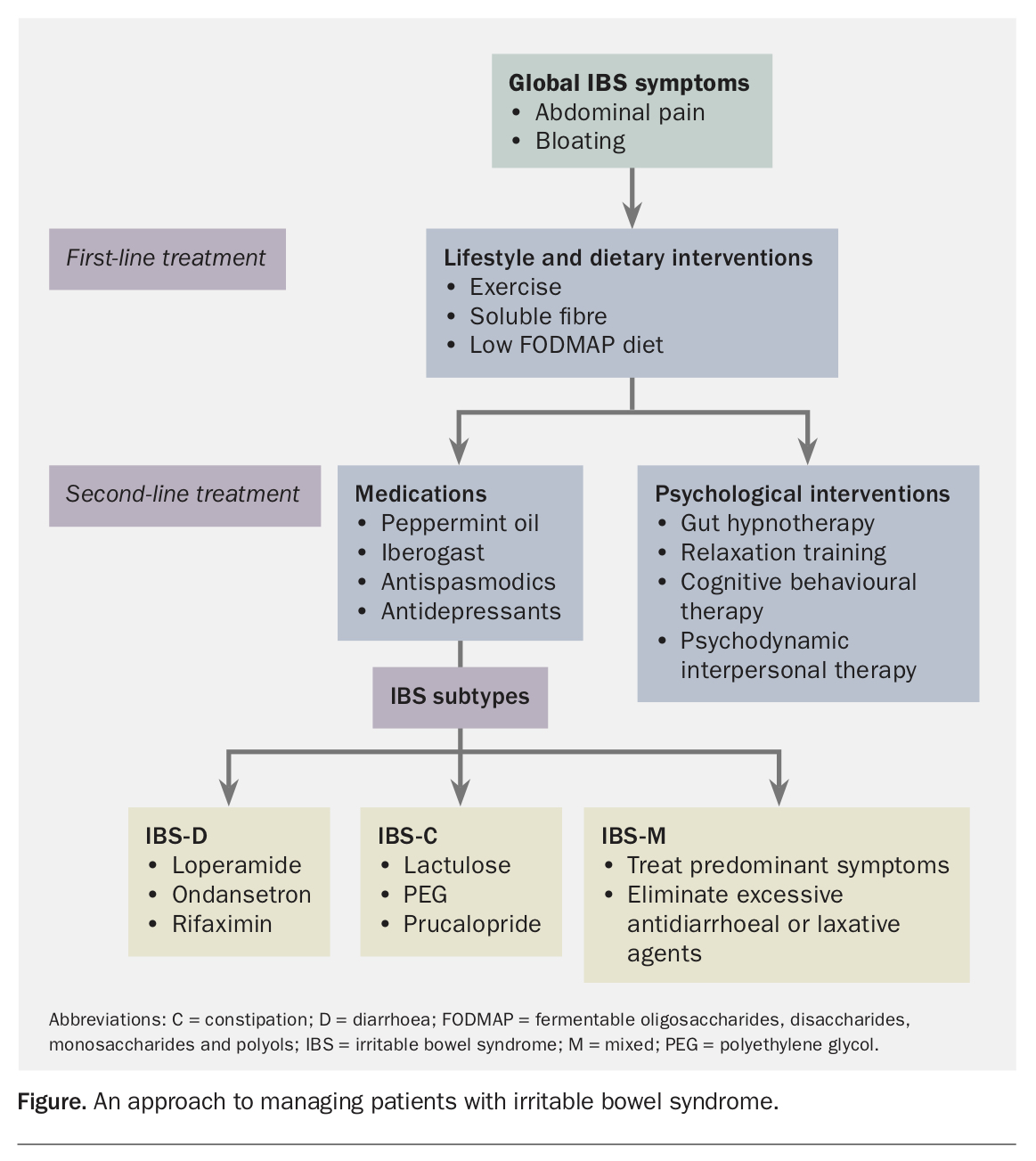
American and European gastroenterology guidelines advocate for the clinician to provide a confident, positive diagnosis of IBS with minimal investigations, as it reduces time to commence therapy and can better direct patients to explore therapeutic options rather than focus on pursing more investigations.7,22 This approach is also supported by GESA’s advice to GPs.12ch of ‘diagnosis by exclusion’) involves initially ensuring the ROME IV criteria are met, while limiting diagnostic tests and providing careful longitudinal follow up.22 Once a positive diagnosis is made, the IBS subtype should be determined by asking the patient to record stool consistency on days that they identify abnormal bowel habit. The Bristol Stool Form scale is used to accurately record stool consistency when the patient is not on any stool-altering medications.23 An approach to managing patients with IBS is summarised in the Figure.
{kind=link}
Dietary and lifestyle modifications
Dietary and lifestyle interventions treat global IBS symptoms regardless of the patient’s subtype, and should be the first-line treatment.22 Up to 80% of patients with IBS have food-related symptoms.24 Reducing the intake of foods that exacerbate IBS symptoms including spicy food, milk and dairy products, alcohol and caffeine has been shown to be efficacious in reducing IBS symptoms.25 Studies have found that psyllium husk, a soluble fibre supplement, is effective in improving IBS symptoms.26 Patients should be started on a low dose with gradual up-titration.24
Fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs) increase fermentation and gas production, which can cause symptoms of bloating and pain due to luminal distension. A diet low in FODMAPs is recommended for patients to improve global IBS symptoms, with supporting evidence from randomised controlled trials and a meta-analyses demonstrating the effectiveness in reducing IBS symptoms.27-30 Due to its complexity, providing guidance to patients on how to correctly follow a low FODMAP diet is important. The diet consists of three phases:31
- reduce total FODMAP consumption
- reintroduce single FODMAP food to gauge tolerance threshold to that FODMAP
- use information from phase 2 to create an individualised low FODMAP diet for the patient.
A dietitian with expertise in low FODMAP diets is best placed to direct the individual dietary plan.7 Regular exercise is also important as a first-line treatment for IBS patients, with benefits particularly evident in patients with IBS-C.6
Psychological treatment
There is strong evidence to suggest that the gut-brain axis influences the psychological comorbidities experienced by many patients with IBS. Therefore, early integration of psychological therapy can help patients manage symptoms of IBS.32
Simple and effective psychological management includes addressing any psychosocial stressors and providing reassurance and education on the pathogenesis and nature of IBS. Involving a psychologist, particularly one with a special interest in gut health, is important.
Psychological therapies that have been shown to be effective in managing symptoms of IBS include gastrointestinal cognitive behavioural therapy, gut-directed hypnotherapy, mindfulness-based stress reduction and psychodynamic interpersonal psychotherapy.24,31,33 These therapies can be conducted in individual or group sessions over several weeks, in multiple sessions and can be introduced to the patient at any point in the treatment course of IBS.31
Pharmacological therapies
Patients with mild IBS in whom symptoms do not significantly impact on daily activities can be managed by providing a positive diagnosis, education and dietary and lifestyle changes. For those who do not respond to these approaches, pharmacotherapy can be considered.
For global IBS symptoms of abdominal pain and bloating, Australian and international guidelines recommend treatments with peppermint oil, Iberogast, tricyclic antidepressants (TCAs; off-label use) and antispasmodics.7,33,34 Peppermint oil has calcium channel blockade effects and can reduce smooth muscle spasm. Clinical trials showed doses of 0.2 to 0.4 mL three times daily provided symptom relief to patients with IBS, but can cause reflux and nausea, as it can relax the lower oesophageal sphincter. If this occurs, enteric-coated tablets of peppermint oil can be used.35 Iberogast is a herbal medicinal preparation that has been shown in randomised controlled trials to be effective in relieving abdominal pain and other IBS symptoms at doses of 1mL three times daily compared with placebo.36 Antidepressants have gastrointestinal neuropathic-pain modulating effects and have symptomatic benefit in IBS treatment, independent of coexisting depression.22,37 Low-dose TCA (i.e. 5 to 10 mg amitriptyline equivalent dose) has been shown to reduce abdominal pain in patients with IBS.14
Antispasmodics and probiotics are currently recommended by GESA as treatment for global IBS symptoms.34 Hyoscine and mebeverine are smooth muscle relaxants and are considered safe over the counter medications that patients can trial, although there is increasing evidence that efficacy in improving global IBS is low.33 A trial of antispasmodics can be carried out after informing patients of possible side effects such as dry mouth and constipation.7 Although probiotics have been used extensively in the treatment of IBS and have minimal concerning side effects, the quality of evidence regarding their efficacy is low and positive trials are prone to a large placebo effect. The GESA IBS decision tool outlines minimal side effects from a trial of probiotics but the overall evidence is poor, and international guidelines have mixed recommendations regarding the usefulness of probiotics in the management of IBS.7,24 Patients should not be encouraged to purchase multiple courses of probiotics if they have been ineffective after a 12-week trial.16
IBS subtypes
Mixed opioid agonists/antagonists (e.g. loperamide), 5-HT3 antagonists (e.g. ondansetron) and rifaximin have been recommended by GESA as effective therapies for treating patients with IBS-D.38 Loperamide is an opioid analogue that reduces diarrhoea but has little effect on abdominal pain.33-39 In fact, side effects of loperamide include abdominal pain, as well as bloating and nausea. To reduce these side effects, it should be started at the lowest dose (2 mg once a day) and slowly titrated upwards.24 Ondansetron, which works by slowing colonic transit, should similarly be started at the lowest dose of 4 mg once daily.34
Rifaximin is proposed to restore the altered gut microbiome in patients with IBS, with clinical trials demonstrating its effectiveness in managing IBS symptoms compared with placebo.40 However, rifaximin is currently only indicated on the PBS for hepatic encephalopathy treatment. Although sometimes used, cholestyramine (a bile acid sequestrant) is not recommended for treatment of IBS-D by Australian and international gastroenterological societies unless there is a history of cholecystectomy.7,38
For patients with IBS-C, pharmacological therapies, including low-dose polyethylene glycol (PEG), low-dose lactulose and 5HT4 receptor agonist (prucalopride), have shown efficacy in symptom improvement and are recommended by GESA. PEG is an osmotic laxative that improves chronic constipation, although evidence is sparse on its efficacy in treating IBS-C.7 However, it is relatively safe withminimal side effects (bloating and flatulence) and thus can be trialled in patients with IBS-C. Similarly, low-dose lactulose can be used if there is no response to PEG, and is preferred over stimulant laxatives due to tolerance and the rare side-effect of an atonic colon with long-term stimulant laxative use.41,42 Prucalopride has been shown to be effective in treating constipation and can be taken at 1 to 2 mg daily if other therapies fail. Possible adverse effects include headaches, nausea and abdominal pain.43 Patients should be advised to stop treatment if there is no response at four weeks.
Treatment of patients with IBS-M should be tailored to predominant symptoms and is largely based on the treatments for IBS-D and IBS-C; however, ensuring patients do not experience ‘pseudo-IBS-M’ due to use of laxatives or antidiarrhoeal agents is important.22
Conclusion
The management of patients with IBS follows a longitudinal model of patient care, which takes into account the patient’s biopsychosocial context while addressing their gastrointestinal symptoms. As GPs have an established therapeutic relationship with their patients, they are uniquely placed to manage patients with IBS. Patients who present with alarm features, diagnostic uncertainty, or who have ongoing symptoms or concerns should be offered specialist referral. MT
References
Clinical%20Practice%20Resources/Iron%20Deficiency/Iron_Deficiency_2015.pdf (accessed July 2021).