Aural discharge. Types, causes and treatment

Most patients with an aural discharge can be effectively treated with ear toileting and antibiotic ear drops, although some require specialist referral. Care is needed with the use of potentially ototoxic ear drops, particularly in patients with otitis media with perforation of the eardrum or grommets.
- An ear discharge is usually caused by a bacterial or fungal infection of the external ear canal or otitis media discharging through a perforation in the tympanic membrane.
- Simple ear toileting techniques and local application of antibiotic drops and ointments in conjunction with waterproofing of the skin of the ear canal resolve most infections promptly.
- Most available antibiotic ear drops are ototoxic and can only be used in a discharging ear with perforation for a few days.
- Ear swab cultures may be useful if treatment fails, and in patients who have diabetes or are immunocompromised.
- Patients with increasing pain or bleeding and those who fail to respond to simple treatment or who are at risk due to diabetes, immunocompromise or previous radiotherapy require referral for specialist assessment.
- Cancer of the ear canal is rare but has similar symptoms to otitis externa that has responded poorly to treatment, and a high degree of awareness is required.
Discharge from the ear canal (otorrhoea) is a common clinical problem that is most often related to infection of the external ear canal skin (otitis externa). However, it can also be due to infection of the middle ear if the eardrum is perforated (otitis media with perforation). This article describes the various causes of an ear discharge, their features and treatments. The differential diagnosis of an ear discharge is summarised in Box 1.
{kind=link}
The normal ear
The external ear canal is supported by bone in its medial part and by cartilage in its outer parts and is closed at the medial end by the tympanic membrane. It is lined by tightly bound squamous epithelium that is thicker in the cartilaginous part than in the bony part. This skin contains hair follicles and specialised sebaceous glands responsible for wax secretion (ceruminous glands) and has a unique migratory property that is responsible for the self-cleansing nature of the external ear. Over a period of months, the epithelium migrates radially off the drum and along the external canal surfaces, becoming mixed with the secretions from the ceruminous glands and any impacted debris, forming ear wax (cerumen). This oily secretion contains immunoglobulins and lysozymes and forms an acidic waterproofing layer that, together with the migrating surface epithelium, forms the primary defence against infections of the ear canal.
Otitis externa
Mechanisms of infection
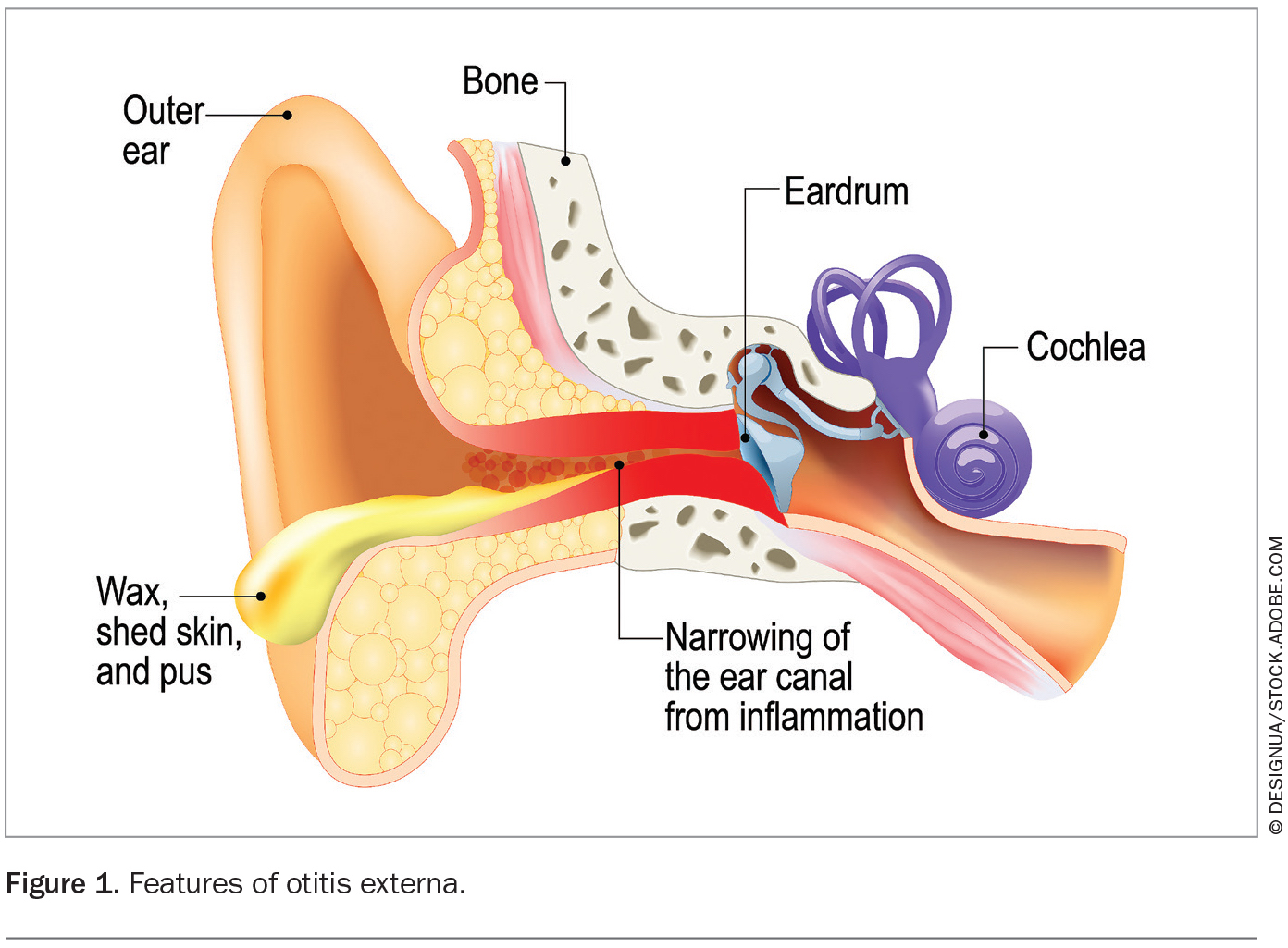
Otitis externa is usually caused by a combination of factors that impair the normal protective mechanisms of the external ear canal, allowing the entry of micro-organisms to the underlying tissues, leading to infection and inflammation (Figure 1). These factors include:
{kind=link}
- water exposure
- humidity
- mild trauma
- chemical irritation
- dermatitis.
Patients who have diabetes or are immunocompromised are at greater risk. Chronic skin diseases such as eczema, psoriasis or contact sensitisation can involve the skin of the ear canal and also impair the protective mechanisms.
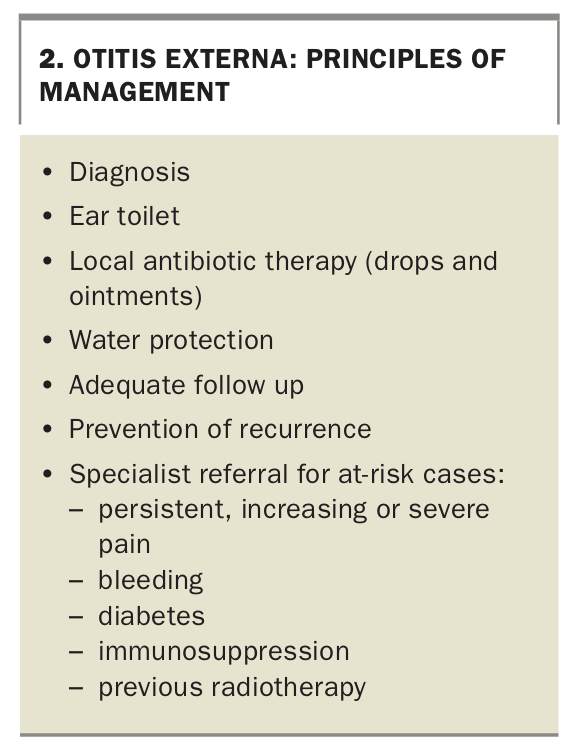
Principles of treatment
Treatment of ear canal infections aims to restore the protective mechanisms to their normal state by removing accumulated debris, treating the underlying infective agent with local antibiotic applications and promoting waterproofing of the ear canal skin (Box 2).
{kind=link}
Resolution of all symptoms and the return to the normal self-cleansing properties of the canal skin (as signified by the production of wax) often takes two to three weeks. Symptom resolution generally occurs before return of wax production and it may be tempting to stop treatment at this point. Treatment should, however, continue during this asymptomatic period to prevent recurrence of the infection. Persisting or worsening symptoms are often due to failure to follow the principles of therapy; a return to these seemingly simple basic steps usually produces rapid and satisfying results.
Diffuse otitis externa
Acute diffuse otitis externa
Acute diffuse inflammatory change involving the external ear canal skin (acute otitis externa) is by far the most common form of otitis externa encountered in clinical practice. Most infections result from water exposure and waterlogging causing a loss of waterproofing (swimmer’s ear), excessive humidity causing keratin maceration (tropical ear) or underlying skin diseases such as dermatitis, psoriasis or contact sensitivity removing the waterproofing layer. The infection is often triggered by mild trauma, for example, ear cleaning with a cotton bud, hair clip or towel after swimming.
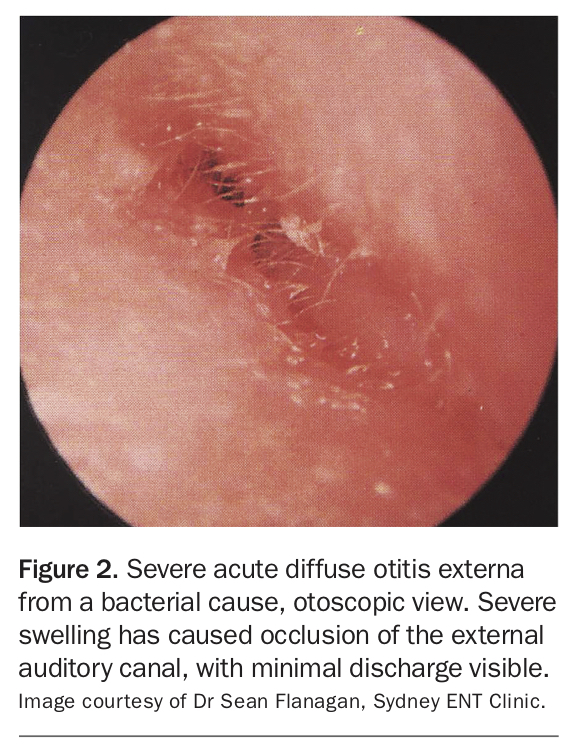
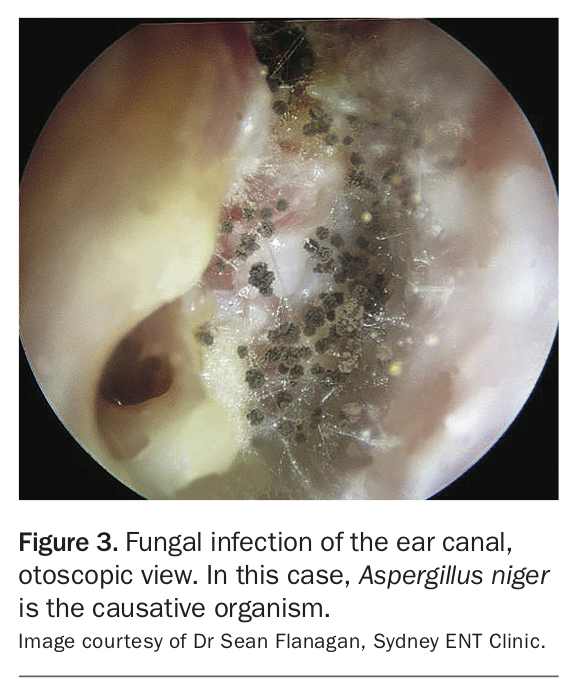
In the early stages of infection, a sparse watery discharge and irritation are the only symptoms. The ear canal skin appears mildly inflamed and waterlogged but the canal lumen remains patent. As the inflammation progresses, the ear canal lumen becomes occluded, resulting in loss of hearing, and there is a dramatic increase in pain (Figure 2). The ear canal appearance is of macerated ‘wet blotting paper’ keratin and oedema. Fungal hyphae may be visible, with the colour giving a clue as to the underlying causative organism (black is most likely Aspergillus niger; yellow is most likely Aspergillus flavus; Figure 3).
{kind=link}
{kind=link}
At the extreme stages of infection, there is intense pain and total occlusion of the ear canal, trismus, cellulitis of the periauricular soft tissues and local lymphadenopathy. Examination of the ear at this stage is difficult, particularly in children, because any manipulation of the pinna or ear canal produces extreme pain. This pain is due to the tight binding of the epithelial lining to the underlying cartilaginous and bony canal, so that even slight oedema causes a large increase in local tissue tension. Analgesia is helpful in the most acute stages of the infection, but it is not until the inflammation begins to resolve that extreme pain subsides.
Although therapy in the painful stages of otitis externa is often difficult, with patience and the appropriate equipment it is possible to toilet the ear canal and apply topical antibiotic. A head light, a fine dental broach probe loaded with cotton and an otowick are useful tools that are readily available and inexpensive. The co-operation of the patient is essential to prevent any more discomfort than is necessary during the procedure, and a brief general anaesthetic may be required for children. The toileting process often has to be repeated a few times (such as on alternate days) until the oedema and canal occlusion resolve and the tympanic membrane can be seen.
Antibiotic drops and ointments
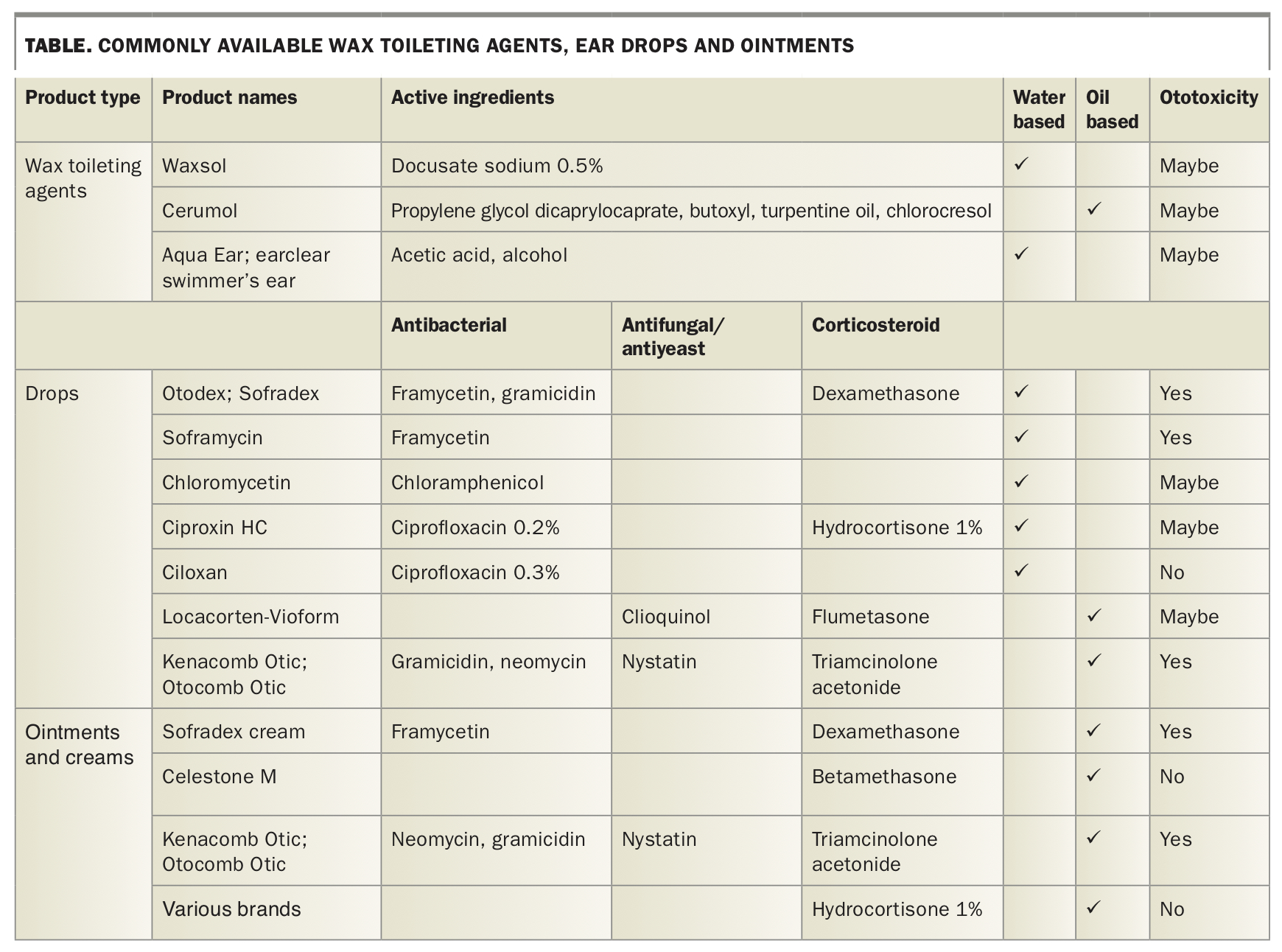
Some preparations available for treating a discharging ear are listed in the Table. Most consist of antibacterial or antifungal agents in combination with a corticosteroid, and they are formulated as either water-based drops and creams or oil-based drops and ointments.
{kind=link}
The choice between an oily or water-based treatment is important. Although treatment with water-based drops is easier, prolonged treatment tends to further waterlog the already oedematous and macerated canal skin, promoting fungal overgrowth and treatment failure. My preference is to commence therapy with a water-based drop (such as framycetin alone or in combination with dexamethasone and gramicidin) applied with an otowick for a few days. Once the acute pain has subsided and the canal has been thoroughly toileted, then a change to an oil-based drop (combined antifungal and corticosteroid with or without an antibiotic) is indicated. The oily treatment can be instilled as a drop (warming renders the solution soothing and less viscous) or painted on with a cotton-loaded broach probe. Filling the canal with ointment using a 2 mL syringe and a blunt 16 gauge plastic catheter is a useful technique, as the ointment lingers for a week or two and the patient does not have to apply further medication.
Ear swabs
A wide variety of commensal bacteria and some fungi occupy the healthy ear canal. The most common infecting organisms are Gram-negative bacilli such as Pseudomonas aeruginosa and Proteus spp. Less common infecting organisms are Gram-positive cocci such as Staphylococcus aureus and streptococci, and sometimes yeasts such as Candida and other fungi such as Aspergillus niger.
Knowing the microbiology of the discharging ear seems of little practical relevance in treatment. Cultures often produce a mixed result or a commensal organism, and my experience has been that following the general principles of therapy is more important in producing rapid resolution of infection than the specific choice of antimicrobial agent. However, swab cultures may be useful in cases of treatment failure, or in patients who have diabetes or are immunocompromised, and often show a fungal cause.
Water protection
Protection of the external ear canal from water during swimming and showering remains the main preventive treatment for otitis externa. A simple, inexpensive and effective way of achieving this is to place in the conchal bowl a cotton wool ball (about the size of a small fingertip) that has been heavily impregnated with petroleum jelly. Using a new plug each time reduces the risk of contamination and reinfection. This method is suitable for both adults and children.
Commercial silicon ear plugs can be used, but often need to be smeared with petroleum jelly to make them watertight and may abrade the ear canal or transfer infection. Drying agents such as acetic acid plus isopropyl alcohol drops or a hair drier on a low setting are also useful preventive measures. A sensation of stinging indicates the onset of infection, and a change to more intensive antibiotic ear drops and protection against water exposure is required.
Ear wax removal
Removal of excessive wax from the ear canal may be necessary in some patients with otitis externa. Gentle mechanical ear toileting, using a head light and cotton-loaded broach probe, is the preferred technique. Syringing, although useful for patients with excessive wax build-up, is best avoided in patients with otitis externa with active discharge. Wax dissolving drops are also useful for wax clearance, but when used for more than two or three days they can cause chemical irritation of the canal skin.
Dermatitis
Psoriasis and eczema are common predisposing factors for acute diffuse otitis externa. Dermatitis is often responsible for the annoying itch that patients experience after an acute infection has been successfully treated. Patients find it almost irresistible to scratch the canal with a hair pin or cotton bud, causing mild trauma and starting the whole cycle again.
In acute dermatitis, the conchal bowl is inflamed, fissured and weeping. The pinna, periauricular areas and other parts of the body may be affected, often bilaterally. The itch and irritation can be treated with intermittent corticosteroid ear drops and ointments (such as prednisolone or 1% hydrocortisone ointment), or simply warm vegetable oil, with the aims of preventing dehydration and promoting the normal protective mechanisms.
Contact sensitivity
Contact sensitivity to hair sprays, hair or skin care products, soaps or detergents is relatively common. Continual exposure of the ear canal skin to these products can result in sensitisation reactions that present as chronic otitis externa. The diagnosis is suggested by the history of chemical contact and improvement when use of a product is discontinued. Formal patch testing can help identify a causative product if several are suspected.
Sensitisation to therapeutic ear drops, particularly those containing antibiotics (especially neomycin), also occurs and often causes symptoms to persist despite what seems adequate treatment for acute otitis externa. Once this is recognised, using an alternative preparation usually results in rapid symptom resolution.
Localised forms of otitis externa
Localised forms of otitis externa can involve the hair-bearing cartilaginous canal skin (furunculosis), the cartilaginous pinna (perichondritis) or the external surface of the ear drum (myringitis). Discharge, irritation and pain are the common presenting symptoms in all these conditions.
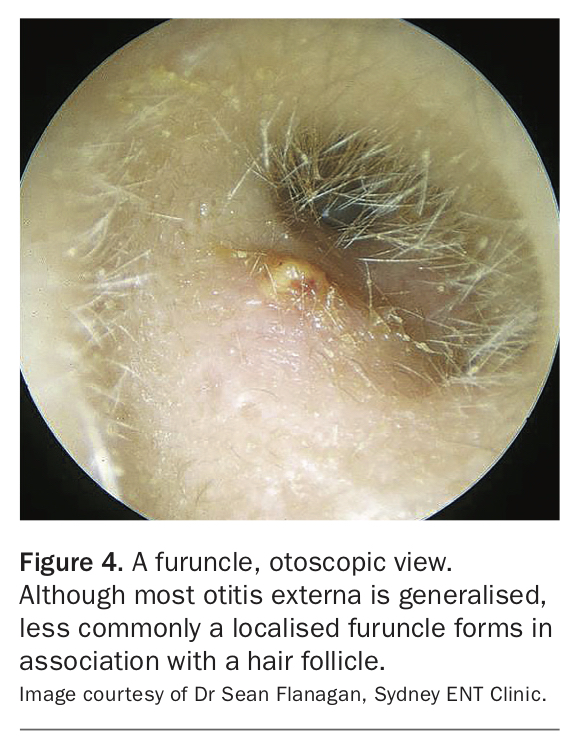
Furunculosis
The hallmark of furunculosis is the intense pain disproportionate to the size of the inflammatory lesion, which is usually only the size of a pimple (Figure 4). The reason for the extreme pain is the same as that in the extreme stages of acute otitis externa – the tight and adherent nature of the canal skin to the underlying cartilage. Great pain is produced with movements such as chewing and smiling and with manipulation of the area for examination or ear toileting. There may also be a small amount of purulent discharge from the lesion.
{kind=link}
The underlying infective organism is S. aureus, and the primary treatment is high doses of oral flucloxacillin for 14 days. Occasionally, lancing may be required.
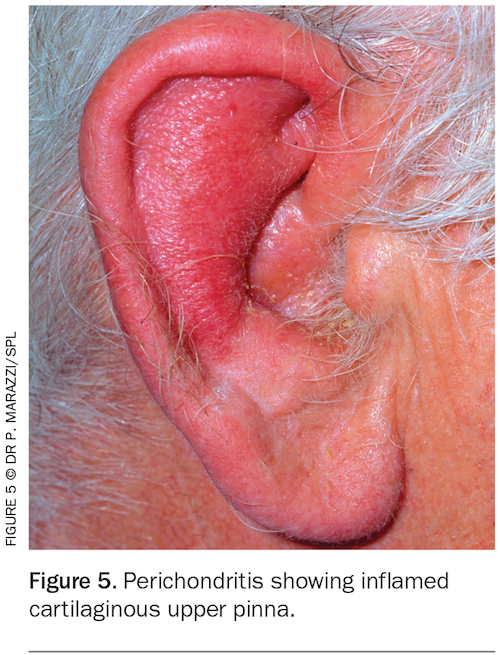
Perichondritis
In perichondritis, the cartilaginous upper pinna becomes inflamed and extremely tender to manipulation, whereas the noncartilaginous lobule is usually spared (Figure 5). Multiple earring piercings in the upper part of the pinna breach the perichondrium and predispose the area to infection, usually with Pseudomonas spp. but occasionally with S. aureus.
{kind=link}
Early perichondritis can be treated with oral ciprofloxacin. However, the condition can be surprisingly debilitating, and established perichondritis needs to be treated in hospital with intravenous antipseudomonal antibiotics (intravenous ciprofloxacin). Prolonged infection leads to abscess formation, extensive cartilage necrosis and cauliflower deformity.
An autoimmune form of perichondritis of the ear may occur (relapsing perichondritis). This is extremely rare and usually part of a systemic illness that presents with perichondritis of the nasal, laryngeal and tracheal cartilages also.
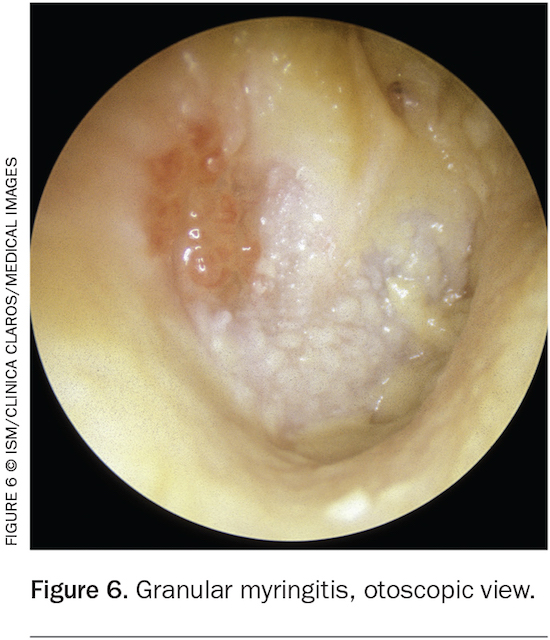
Myringitis
Myringitis presents with mild hearing loss as well as discharge. Examination shows a thickened inflamed tympanic membrane, often with large amounts of granulation tissue obscuring the drum (Figure 6). The surrounding external canal skin is normal. The cause is unknown but presumed to be infective. The condition is difficult to treat and sometimes persists for years. Blunting of the drum margins and foreshortening of the external canal occasionally occurs during healing, resulting in marked hearing loss. This may require surgery to excise the fibrous tissue and grafting of the deep canal and eardrum to improve hearing. Acute myringitis can sometimes be treated successfully with local mild chemical cautery and prolonged application of corticosteroid and antibiotic drops.
{kind=link}
A bullous form of myringitis also occurs, in which large haemorrhagic oedematous blebs form on the outer tympanic membrane surface and in the deep canal. The condition is extremely painful, with relief occurring after rupture of the bullae, which may be accompanied by a small amount of watery bloodstained discharge. This form of myringitis is self-limiting, lasting about two weeks. Mycoplasma pneumoniae has been cultured from the vesicle fluid, but it is not known if treatment with erythromycin shortens the duration of pain.
The discharging mastoid cavity
Chronic otitis media with cholesteatoma is usually treated by mastoidectomy surgery. This procedure involves removing part of the bony and cartilaginous external ear canal and changing the configurations of the middle ear cleft with the formation of a ‘mastoid cavity’ and a widened external canal. Despite the radical alteration of the configurations of the external and middle ear, many mastoid cavities are trouble-free and self-cleansing. Some cavities, however, are susceptible to otitis externa, usually following water exposure.
Annual toileting of the debris build up is the best way of preventing infections. If acute diffuse otitis externa supervenes, thorough toileting of the cavity and application of the general principles of treatment for acute otitis externa should give good results.
Otitis media with perforation and the discharging grommet
A common problem in patients with an ear discharge is to distinguish external ear canal infection from otitis media with perforation of the tympanic membrane or in the presence of a grommet. This is an important distinction because the aetiology and microbiology of external and middle ear infections differ considerably, and their treatments are different.
In otitis externa, it is safe to use potentially ototoxic ear drops because the intact tympanic membrane will prevent absorption via the middle ear to the inner ear. In the presence of a perforation or grommet, however, there is a risk of ear drops being absorbed into the inner ear and, if they are ototoxic, causing irreversible hearing loss and vestibular problems. This possible side effect has to be balanced against the demonstrated efficacy of the most commonly available topical antibiotic ear drop, combination dexamethasone/framycetin/gramicidin, in otitis media with perforation. Although this topical antibiotic therapy has been used with great efficacy in the opened tympanic cavity and discharging grommet setting for many years, the few documented cases of ototoxicity suggest a need for greater caution with its use, including limiting the duration of use to three to four days. If discharge persists beyond this period, the patient should be referred to an ear, nose and throat specialist.
Ciprofloxacin 0.3% ear drops are safe from ototoxic side effects and are the first choice for use in the opened middle ear, perforations and with grommets in place.
Destructive temporal bone conditions
Rarely, otorrhoea accompanied by pain or bleeding indicates a destructive process within the temporal bone, such as osteoradionecrosis, skull base osteomyelitis or malignancy.
Radiation-induced otitis externa: osteonecrosis
Radiation therapy involving the external ear canal and temporal bone results in various changes that present with discharge and pain. There is often an acute reaction during the course of therapy. This diffuse otitis externa tends to settle after the radiation therapy, but symptom resolution can be hastened by applying the usual treatment for the condition.
A long-term result of radiotherapy is an alteration in the migratory properties of the skin of the external canal, resulting in build up of epithelial debris. The treatment is repeated ear toileting at frequent intervals.
At the severe end of the spectrum there is extensive death of the skin and underlying bone, resulting in sequestrum formation. Patients present with continuous offensive discharge, pain and occasional bleeding. The disruption to their lives can be great, and the bleeding often causes lingering concerns about cancer recurrence. Treatment is repeated ear toileting, debridement of the sequestrum and consideration of obliteration of the middle ear cleft and external ear with vascularised tissue. All cases of osteonecrosis require specialist referral.
‘Malignant’ otitis externa
‘Malignant’ or necrotising otitis externa is osteomyelitis of the skull base. It occurs in elderly patients with diabetes or immunocompromised patients and is associated with a high degree of morbidity. Patients present with a purulent and sometimes bloody discharge and intense pain, and the external canal is filled with granulation tissue. Facial nerve or lower cranial nerve palsies are grave prognostic signs.
Early diagnosis can be made on nuclear imaging of the skull base showing intense uptake in the region of the temporal bone. The causative organisms are P. aeruginosa or invasive fungi such as Aspergillus, and treatment involves prolonged intravenous antibiotics.
Carcinoma of the external ear canal
Cancers arising from the skin or glandular elements of the external canal are extremely rare. Bleeding is a hallmark sign, but cancer can present with symptoms identical to those of chronic diffuse otitis externa, with examination of the ear canal showing oedema, swelling, ulceration and granulation tissue. Palpation of ulcerated areas often results in bleeding.
As cancers of this region are rare and the appearance of the canal is similar to that in otitis externa, a high index of awareness is required to diagnose these cancers early. Patients with any suspicious lesions should be referred urgently.
Conclusion
Most cases of ear discharge can be diagnosed on history and examination. Treatment based on simple principles and knowledge of the normal physiology of the ear canal usually produces satisfying results. However, patients who have a persistent discharge, worsening pain or bleeding or whose condition fails to respond to adequate therapy require specialist referral for assessment. A high index of suspicion is required to diagnose early the more sinister and sometimes life-threatening conditions of the temporal bone and skull base that also present with an ear discharge. MT
COMPETING INTERESTS: None.