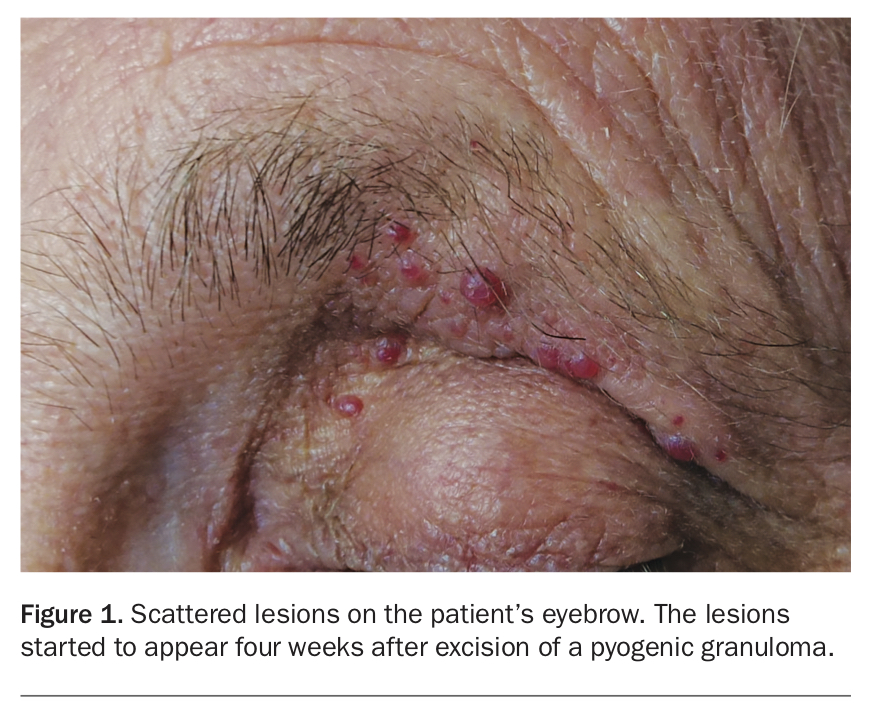
Red-pink papules around a scar on the eyebrow

Test your diagnostic skills in our regular dermatology quiz. What are these scattered lesions on a man’s eyebrow?
Case presentation
A 55-year-old man presents with multiple smooth red-pink papules on his left eyebrow (Figure 1). The lesions started to appear four weeks after excision of a pyogenic granuloma, and within 12 weeks there were 11 papules scattered around the excision site. Associated mild lichenification of the upper and lower eyelids is noted, consistent with dermatitis. There is also evidence of dermatitis on the patient’s forearms and hands.
{kind=link}
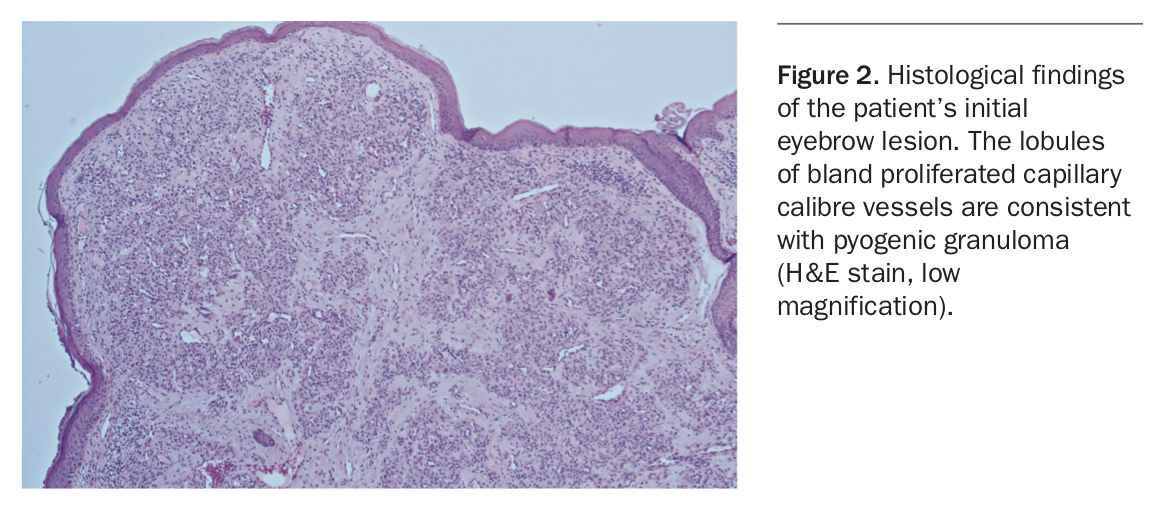
The pyogenic granuloma had presented as an asymptomatic erythematous papule that had been developing over two to three months and was prone to bleeding. The lesion was excised with no complications; histopathology demonstrated a dense proliferation of capillaries in the dermis with no endothelial atypia, consistent with a pyogenic granuloma (Figure 2).
{kind=link}
The patient’s clinical history is significant for allergic rhinitis and adult-onset atopic dermatitis. He has no other medical issues and is not taking any regular medications. There is no personal or family history of skin cancer.
Diagnosis
This patient presents with satellitosis, a phenomenon in which new lesions arise as satellites that are separate and distinct from a primary lesion. Other terms for the new lesions include agminated, eruptive or clustered. The term disseminated has been used to denote new lesions that are more widespread over the body.1
Pyogenic granuloma (lobular capillary haemangioma) is a common benign vascular proliferation of the skin or mucous membranes. Recurrent pyogenic granuloma with satellitosis, also known as Warner Wilson-Jones Syndrome (WWJS), is a rare complication of pyogenic granuloma, and this is the correct diagnosis in this case.2 It is, however, more common in children and unusual in this patient’s age group. The lesions of WWJS are typically 1 to 10 mm in size and appear as asymptomatic red-pink papules within one week to four months and even up to two years after treatment of the primary lesion.3 It has been proposed that trauma may play a role in the development of these lesions – for example, lesions located on the scapulae may result from pressure occurring during sleep.1 In this patient, the lesions were located close to the region affected by eczema, which may have been traumatised by repetitive scratching.
Differential diagnoses
Conditions to be considered among the differential diagnoses in this case include the following.
- Amelanotic melanoma. The presentation of amelanotic melanoma is highly varied. The diagnosis should always be considered in a patient with high risk factors presenting with an erythematous, sometimes scaly, macule, nodule or plaque. It is also a great masquerader.4 Amelanotic melanomas can have polymorphic vascular structures (as seen in pyogenic granulomas) and should be considered for a wide range of differential diagnoses. Dermoscopy may show an atypical vascular pattern, pinpoint vessels and transverse bands. Histopathology may be highly varied; however, Fontana-Masson staining can reveal melanin granules.5 Metastatic melanoma can present with satellitosis. Metastatic carcinoma of a different primary cancer can also be considered – these may be close to the primary cancer anatomically, and histopathologically will have features of the primary malignancy. Although rare, they usually indicate very advanced disease.
- Bacilliary angiomatosis (BA). This infection, which is caused by two Gram-negative bacterial species, Bartonella quintana and Bartonella heneselae, is typically seen in immunocompromised patients such as those with HIV infection. Superficial and nodular types of BA can resemble pyogenic granuloma as they often appear as single or multiple vascular lesions and can also display satellitosis.3 These lesions can also affect other organs such as the liver and spleen. Diagnosis can be confirmed by histopathology, including Warthin-Starry stain showing clumps of bacilli, as well as vascular proliferation in a lobular pattern.6 First-line treatment is doxycycline or erythromycin, with the addition of gentamicin in patients with bacteraemia.7
- Angiosarcoma. The fourth-most common type of cutaneous sarcoma, angiosarcoma presents as haemorrhagic plaques that may evolve into violaceous nodules.8 They can arise on the face and scalp, areas of chronic lymphoedema and sites of previous irradiation, and can have multifocal or satellite lesions.9 Histopathology shows varying degrees of endothelial atypia, depending on the degree of differentiation, and may also show intracytoplasmic vacuoles and an inflammatory infiltrate. Immunohistochemistry confirms the diagnosis with positive stains for spindle cell tumours and vascular markers.8 Treatment may involve staging and screening for metastasis with computed tomography and definitive surgical excision with a role for adjuvant radiotherapy and chemotherapy; however, there are no clear guidelines. The prognosis is poor, with mean five-year recurrence-free survival and overall survival reported as 16% and 38%, respectively.9
- Kaposi sarcoma (KS). The lesions of KS may appear like BA or pyogenic granulomas, and should be considered in all patients with a history of HIV infection. The cutaneous lesions of KA are highly varied (like for BA), ranging from pink macules and patches to violaceous plaques, nodules and polyps. These can arise in a cluster, mimicking satellitosis. There are four clinical variants of KS: chronic/classic (typically in men in central Europe and the Mediterranean), African endemic, iatrogenic immunosuppression-associated and AIDS-related. It is a neoplastic or hyperplastic process driven by a viral infection, typically human herpesvirus.8 Histology shows spindle cells and proliferation of abnormal vasculature, a leukocytic infiltrate with plasma cells and intradermal hyaline globules.8 Management depends on the subtype: classic KS usually follows an indolent course whereas HIV and immunosuppression- associated KS requires more extensive work up to assess for respiratory and gastrointestinal involvement, together with management of the underlying disease.
- Eccrine poroma. These benign lesions, which can be solitary or multifocal, arise from eccrine sweat glands (which are widely distributed throughout the body) and tend to arise in areas of where density of the glands is high – more commonly, the palms, soles, trunk, head and neck. They can be nodular, ulcerated or plaque-like and are highly vascular with a tendency to bleed – similar to pyogenic granuloma. Histologically, there are sheets and groups of basaloid poroid cells spreading from the epidermis into the dermis. Hidroacanthoma simplex and dermal ductal tumours are variants limited to the epidermis and dermis, respectively. Eccrine porocarcinoma is the malignant version of eccrine poroma, in which there are cytonuclear atypia, infiltration and invasion, prominent nucleoli and high amounts of mitotic figures.10 Definitive treatment is achieved with surgical excision.
Management
All of the conditions listed above may appear macroscopically like pyogenic granuloma and may display the phenomenon of satellitosis. A conservative approach is the recommended treatment for WWJS, as lesions usually resolve spontaneously within six to 12 months and recurrence of WWJS is rare.1,3 Other treatment options are those for pyogenic granuloma – these include surgical excision, curettage and cautery, cryotherapy, imiquimod, laser therapy, systemic corticosteroids, intralesional bleomycin/corticosteroids and radiotherapy.1,3,11 For this patient, pulse dyed laser (V Beam) was chosen for treatment because of the surgically challenging location of the lesions, convenience and patient preference, with complete resolution after two sessions of treatment.
Conclusion
It is important for clinicians to recognise WWJS because it is a rare benign disease that usually self-resolves but should be distinguished from a malignant process or another underlying systemic disease, such as HIV infection. The underlying pathophysiology of WWJS is unclear, but a high index of suspicion should exist in settings of trauma, such as in this case patient’s scenario. MT
References