Optimising micronutrients during pregnancy

Dr Best is a midwife; and Senior Research Fellow at South Australian Health and Medical Research Institute, Adelaide.
Professor Makrides is a dietitian; and Deputy Director and Theme Leader at South Australian Health and Medical Research Institute, Adelaide.
Associate Professor Grivell is a Maternal Fetal Medicine Subspecialist; and Matthew Flinders Fellow, College of Medicine and Public Health at Flinders University, Adelaide, SA.
Health problems in pregnancy

Optimising nutrition and micronutrient status during the perinatal period can have a significant impact on the health of the pregnant woman and her child. GPs are well placed to guide women on their nutritional needs during pregnancy and advise on any additional supplementation on an individual basis, in line with national evidence-based guidelines.
- Pregnant women often rely on their general practitioner for information regarding nutrition during pregnancy.
- Women should be encouraged to eat a healthy, varied diet during pregnancy to ensure nutrient requirements are met, and counselling should be provided regarding appropriate supplement use.
- Dietary patterns consistent with the Australian Dietary Guidelines will allow most women to meet micronutrient requirements in pregnancy. However, routine supplementation with folic acid and iodine is recommended.
- Supplementation with other micronutrients may be advised on an individual basis following assessment of nutritional status.
Women’s nutrition in the preconception period and throughout pregnancy is crucial to ensuring optimal outcomes for both the mother and child. Requirements for many vitamins and minerals, referred to collectively as micronutrients, increase during pregnancy to support the growth and development of the fetus. Inadequate stores or intake of micronutrients during this critical period, may have adverse effects on both the mother and the baby.1 It is therefore important that pregnant women make some dietary changes to ensure they meet their increased micronutrient needs. This article discusses common nutrient deficiencies that may occur in pregnancy and summarises the evidence base for supplementation for women during pregnancy.
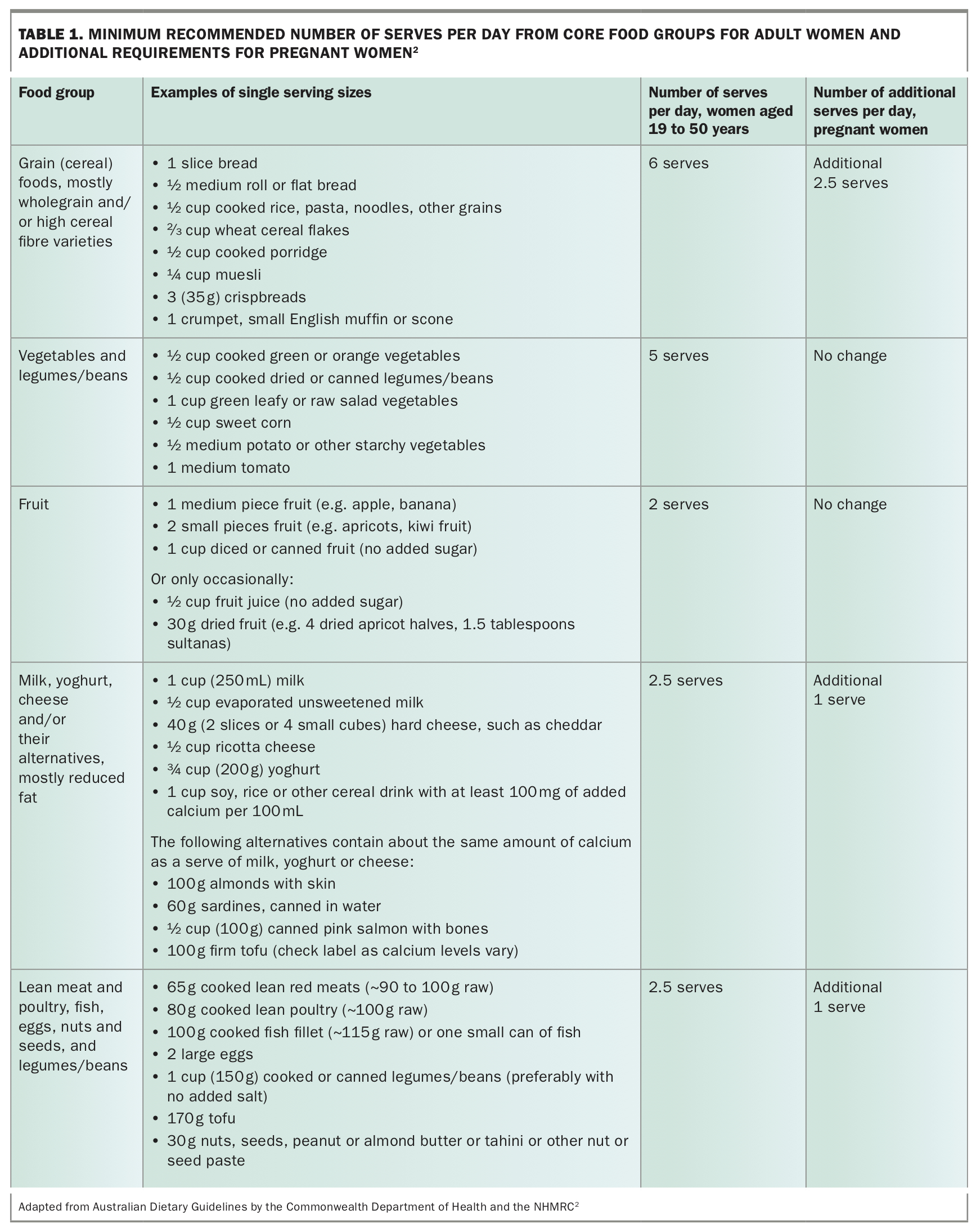
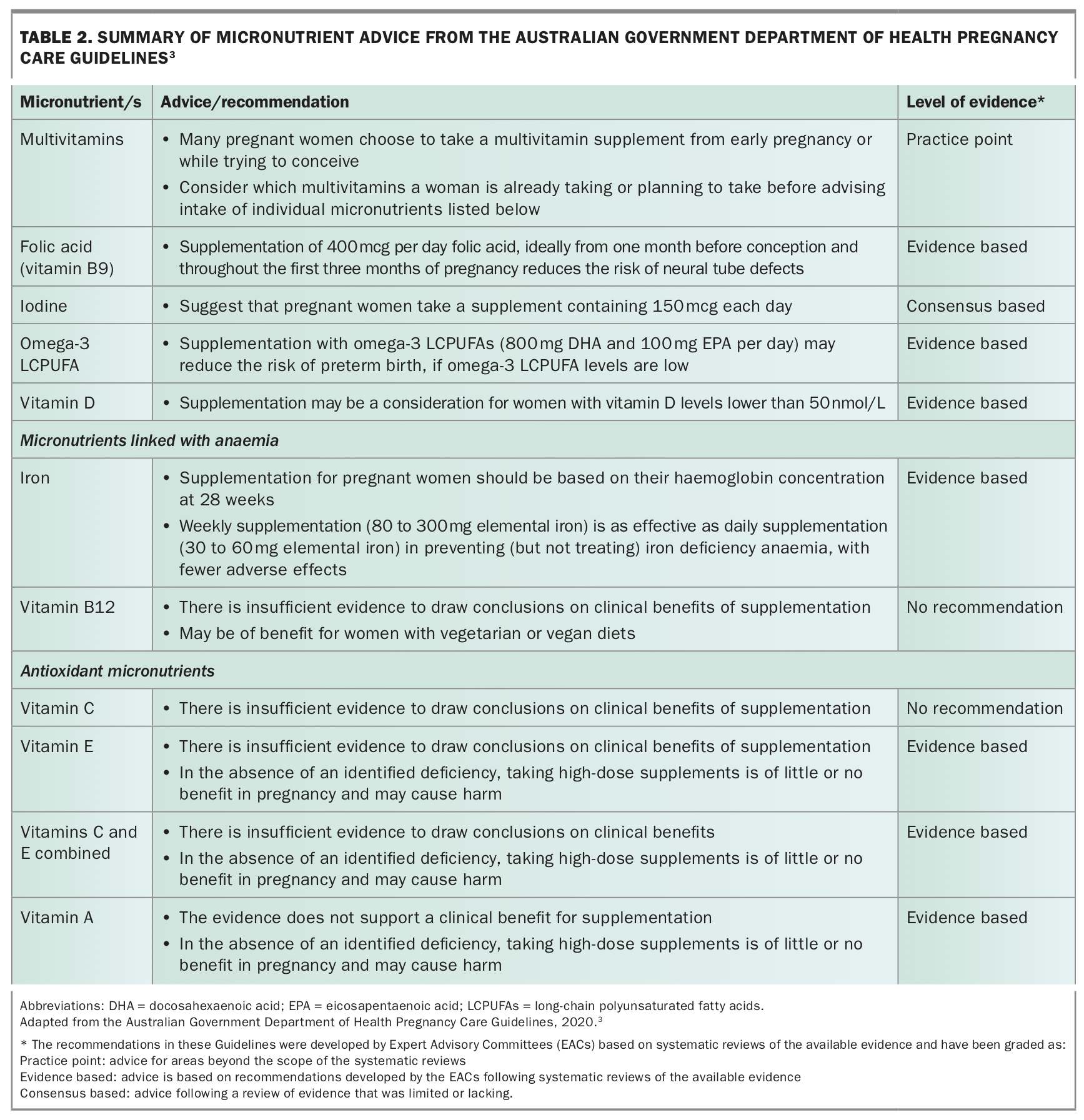
Pregnancy requires additional nutrient and caloric intake, although the recommended increase in calories is relatively small.2,3 Pregnant women can largely meet their nutritional needs by following government-endorsed dietary guidelines, such as the Australian Dietary Guidelines, and by adding extra daily serves of some core food groups, listed in Table 1.2 By adding extra serves of grains and cereals, dairy and other protein-rich foods such legumes, eggs, nuts, fish, seafood and unprocessed meats, it is possible to meet the extra need for important micronutrients such as iron, zinc, iodine, folate and omega-3 fatty acids. However, some water-soluble micronutrients such as folate can be leeched or destroyed during the cooking process, which adds to the difficulty of meeting the increased requirements for some nutrients. Although micronutrient supplementation is often used as a preventative health measure in pregnancy, only some supplements are beneficial and routine supplementation of all women is only recommended for specific micronutrients including folic acid and iodine.3 Supplementation with other nutrients such as omega-3 long-chain polyunsaturated fatty acids (LCPUFAs), vitamin D or iron may be advised based on depleted nutrient status of the women. Women should be advised that, in the absence of an identified deficiency, taking high-dose supplements of vitamin A, C or E is of little or no benefit in pregnancy and may cause harm (Table 2).3
{kind=link}
{kind=link}
Many pregnant women rely on their GP for information regarding nutrition, emphasising the importance of evidence-based advice as an essential component of antenatal care.4 Antenatal visits should include questions about the woman's current eating patterns and an assessment of known risk factors for micronutrient deficiencies, including ethnicity (which has been linked to vitamin D levels) and diet (e.g. vegan or vegetarian diets).5,6 Advice regarding supplementation with micronutrients should be tailored to the individual woman with consideration of the availability and affordability of foods appropriate to the woman’s cultural practices and preferences, and the need for and affordability of supplements.
Folate and folic acid
Folate is a B-vitamin that is naturally present in many foods including leafy green vegetables, citrus fruit, breads, cereals and legumes. It serves many important functions and plays a crucial role in cell growth and the formation of DNA. Folic acid is the synthetic, more stable form of folate, and is often added to foods or used in supplements.
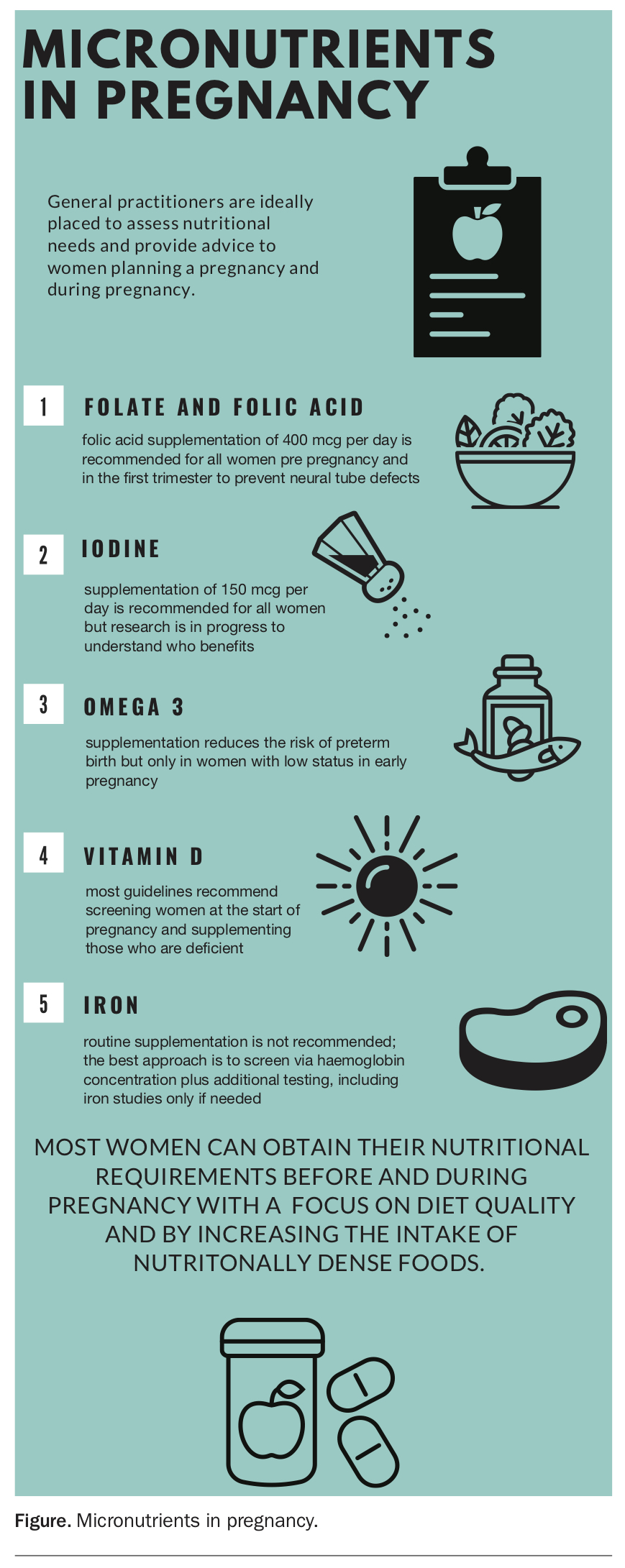
There is consistent scientific evidence that folic acid is of high importance for the prevention of neural tube defects (NTDs), and health authorities around the world recommend supplementation.7 Given that it can take three weeks to increase serum folate to adequate level, folic acid supplementation should be started before conception and continued until neural tube closure, which normally occurs around 28 days after conception. The current evidence-based guidance recommends women take a daily dietary supplement containing 400 micrograms of folic acid for at least one month before trying to become pregnant until 12 weeks of gestation (Figure).3 Prescription of the bioavailable form of folic acid, L-methylfolate, may be advantageous to women diagnosed with genetic polymorphisms that impair the conversion of supplemental folic acid to its active form.8
{kind=link}
Despite recommendations for supplementation, many Australian women do not have sufficient folate intake in early pregnancy;9 and for many women, neural tube closure occurs before they confirm their pregnancy. Therefore, mandatory folic acid fortification of bread-making flour was introduced in Australia in 2009. This action has increased folic acid intake in women of reproductive age by around 0.15 to 0.2 mg/day and has reduced the incidence of NTDs by about 14% in states where data are available.10 Even greater reductions in NTDs have been reported in the offspring of Australian Indigenous and teenage women.11 The preventative strategy of adding folic acid to food staples has been adopted by more than 80 countries worldwide.12
Although routine folic acid supplementation has been universally adopted for the prevention of NTDs, systematic reviews of the available evidence suggest that continuing supplementation beyond the periconceptional period does not improve other pregnancy outcomes such as premature birth, low birth weight or miscarriage.13,14 Similarly, a recent large randomised controlled trial showed that high-dose folic acid supplementation throughout pregnancy did not to reduce the risk of preeclampsia.15 There are no clear benefits for taking higher doses of folic acid or continuing supplementation beyond 12 weeks of pregnancy.
Iodine
Iodine is a trace element that is naturally present in some foods. The main dietary sources of iodine in Australia include bread, eggs, dairy, iodised salt and seafood. Iodine is used by the body to produce thyroid hormones, which are important for the growth and development of the fetal nervous system. During pregnancy (and breastfeeding), thyroid activity increases, therefore, pregnant women have a higher risk of iodine deficiency because of their increased iodine requirement.16 There is no reliable way to measure iodine status in an individual; however, urinary iodine concentration is used as a biomarker to determine iodine status on a population level.
Observational studies suggest that mild to moderate iodine deficiency during pregnancy may result in childhood learning difficulties and affect the development of motor skills and hearing.17 The results of the 2004 national survey of school-aged children showed that mild iodine deficiency (based on urinary iodine concentration) had re-emerged in south-eastern parts of Australia.18 In response, in addition to folic acid fortification in 2009, the Australian government also mandated the replacement of non-iodised salt with iodised salt for bread-making. Mandatory fortification has increased levels of iodine in the food supply and improved iodine status in the general population and women of child-bearing age (52% increase).10 Moreover, a consensus-based recommendation was made that women who are considering becoming pregnant, who are pregnant, or are breastfeeding should consume 150 micrograms of iodine per day through supplements, as well as obtaining iodine from a healthy diet (Figure).
Australia and New Zealand are the only countries to have combined policies of mandatory iodine fortification of foods and recommended for supplementation during pregnancy and lactation. This double-barrelled approach was recently brought into question by an evaluation of iodine nutrition during pregnancy in South Australia, which showed that children of pregnant women whose iodine intake was at the extreme ends (either too low or too high) had poorer performance on cognitive and language tests compared with children of pregnant women with adequate iodine intake levels.19 A randomised controlled trial to determine the effect of iodine supplementation in pregnancy on early childhood neurodevelopment is underway in Australia and will provide evidence regarding optimal iodine intakes for pregnant women (https://clinicaltrials.gov/ct2/show/NCT04586348).
There are limited single-nutrient iodine preparations and most women will select a multivitamin and mineral prenatal supplement containing iodine. Women should be advised not to exceed recommended intakes for all supplements, but iodine is a particular concern. Seaweed and kelp supplements are high in iodine but can contain toxic levels and are therefore not recommended during pregnancy.
Omega-3
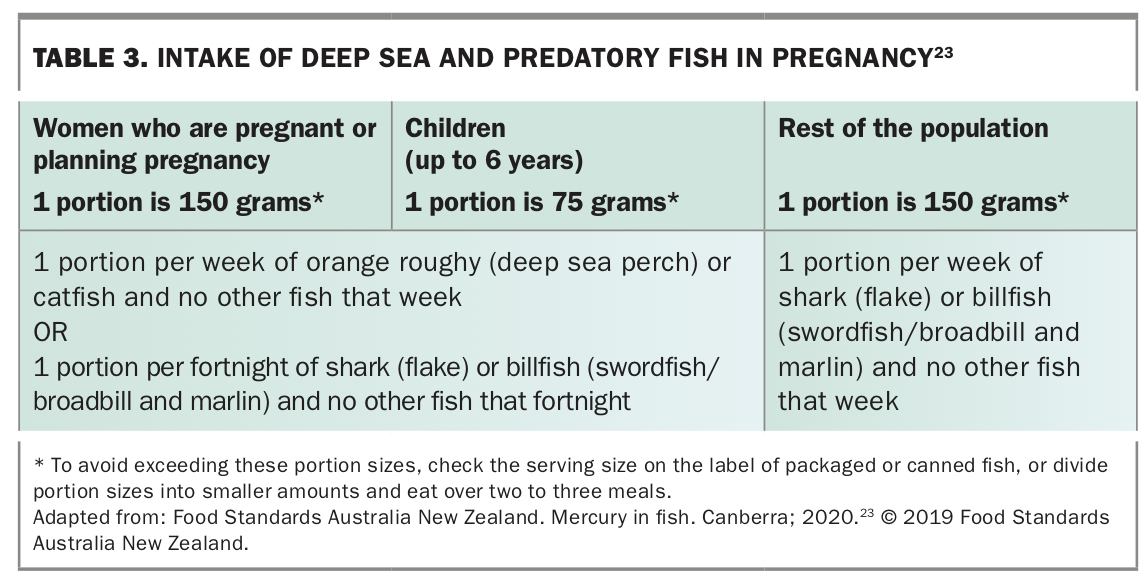
Fish and fish oils are rich sources of omega-3 LCPUFAs, particularly docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA). In population studies, intake of omega-3 LCPUFAs in pregnancy has been associated with longer pregnancy and improved perinatal outcomes.20, 21 However, pregnant women are reluctant to increase their fish intake because of concerns around mercury levels in seafood. Women may even decrease their intake because of these concerns and confusing advisories.22 Women can safely consume two to three serves of cooked seafood per week by avoiding the larger, deep sea predatory fish (Table 3).23 Additionally, canned fish such as tuna and salmon are low in mercury and can be consumed more regularly.
{kind=link}
The recent Cochrane Review assessing the effects of omega-3 LCPUFAs (taken as supplements or as dietary additions during pregnancy) on pregnancy outcomes showed a lower risk of preterm birth (<37 weeks) and early preterm birth (<34 weeks) for women receiving omega-3 LCPUFAs compared with those not receiving omega-3 LCPUFAs.24 Preterm birth at less than 37 weeks was reduced by 11% in women who received omega-3 LCPUFAs compared with women who did not receive omega-3 (risk ratio [RR], 0.89; 95% confidence interval [CI], 0.81 to 0.97) and early preterm birth at less than 34 weeks was reduced by 42% (RR, 0.58; 95% CI, 0.44 to 0.77). Many of the trials in this review were conducted before prenatal supplementation with low levels of omega-3 LCPUFA was common. The largest and most recent Australian trial suggests that routine omega-3 supplementation of all women in pregnancy will not be effective in reducing overall premature birth rates, rather it will only benefit women with a low omega-3 status in early pregnancy in this way.25-27 Women with sufficient omega-3 status in early pregnancy are already at lower risk of preterm birth and further omega-3 supplementation may increase this risk.26 The latest update of the Australian Pregnancy Care Guidelines includes an evidence-based recommendation for women with low omega-3 levels to take an omega-3 supplement (800 mg DHA and 100 mg EPA) to reduce their risk of preterm birth.3
Identifying women with low omega-3 status by assessing diet is difficult unless they are vegans or vegetarians who also do not consume eggs. In South Australia, a state-wide program of serum omega-3 screening in early pregnancy commenced in April 2021. This screening program will identify women with low status and guide their treatment to assess the effectiveness of a precision nutrition approach to reducing preterm birth on a population basis.
Vitamin D
Vitamin D (also known as calciferol or D2 and D3) is a fat-soluble vitamin that is found in only a small number of foods (namely fish-liver oils, fatty fish, mushrooms, egg yolks and fortified foods), but is easily synthesised cutaneously by humans through exposure to sunlight.3
Vitamin D has specific functions, including bone and muscle development, and in pregnancy plays a role in fetal calcium metabolism and bone development. Vitamin D deficiency in pregnancy may be associated with adverse pregnancy outcomes, particularly hypertensive disorders, preeclampsia and gestational diabetes for women and small for gestational age for neonates.28 Varying policies and practices are in place internationally to screen for and treat vitamin D deficiency in pregnancy including universal supplementation (for high-risk populations); screening serum levels in all women and treating those labelled as deficient; and screening by risk factors, assessing serum levels and treating those who are deficient.28
A recent Cochrane review examining whether vitamin D supplementation during pregnancy, alone or in combination with calcium or other vitamins and minerals, could safely improve maternal and neonatal outcomes concluded that supplementation with vitamin D alone probably reduced the risk of preeclampsia, gestational diabetes and low birth weight but had no impact on neonatal health outcomes.29 Further rigorous, high-quality and larger randomised trials are needed to evaluate the effects of vitamin D supplementation in pregnancy, particularly in relation to the risk of maternal adverse events.29
Routine vitamin D supplementation is not currently recommended for the general population in Australia. Pregnancy care guidelines in many state and territory jurisdictions recommend screening via blood/serum levels at the antenatal booking visit and treating women when serum levels indicate deficiency.
Iron
Iron deficiency is the most widespread nutritional deficiency during pregnancy and the leading cause of anaemia. Anaemia in pregnancy is common, occurring in up to 40% of pregnancies and may be associated with significant maternal and perinatal morbidity. When anaemia in pregnancy is identified and managed appropriately, maternal outcomes improve.30
A recent Cochrane review comparing the effects of daily oral iron supplements with no iron supplement and placebo suggested that preventive iron supplementation during pregnancy reduces maternal anaemia at term by 70% (RR, 0.30; 95% CI, 0.19 to 0.46,), iron deficiency anaemia at term by 67% (RR, 0.33; 95% CI, 0.16 to 0.69) and iron deficiency at term by 57% (RR, 0.43; 95% CI, 0.27 to 0.66).30 The impact on pregnancy outcomes is less clear, with no statistically significant results seen for maternal or neonatal outcomes.30 As such, in most populations it is more appropriate to screen women for iron deficiency by haemoglobin concentration initially. Further testing includes full blood count (if this has not already been conducted), serum ferritin level and specific tests for folate and vitamin B12 levels, if mean cell volume is high.3 Women subsequently identified as iron deficient can then be treated appropriately. Oral iron supplementation remains first-line treatment for iron deficiency anaemia identified in the antenatal period. Intravenous iron should be offered to women who do not respond to oral iron or who are unable to comply with therapy.31
Conclusion
General practitioners are well placed to provide both planned and opportunistic prepregnancy and early pregnancy nutritional advice to women throughout their reproductive years. For all women of reproductive age, a dietary history with focus on specific risk factors will assist GPs in identifying women who may be at risk for micronutrient deficiency. Advice on and assistance to improve diet quality will provide significant nutritional benefit, after which specific treatments can be offered when indicated. Referral to a dietitian may be helpful, for practical advice and support for pregnant women with deficiencies. For women planning a pregnancy and those in early pregnancy, unless there are specific risk factors (i.e. restrictive diets), micronutrient needs can be met with a balanced diet with the addition of a few core food groups or serves of core foods. Many pregnant women take a multivitamin supplement from early pregnancy or while trying to conceive. These supplements contain most of the individual vitamins/minerals discussed in this article, so when providing advice, consider which multivitamins a woman is already taking or planning to take. For many micronutrients, excessive intake can be a concern and should be avoided in pregnancy. MT