Common skin problems in children. Rashes other than atopic dermatitis


In addition to atopic dermatitis, numerous other endogenous and exogenous dermatoses are seen in prepubertal children including nappy rash, psoriasis, neonatal acne and allergic rashes. Many of these childhood dermatoses will clear over time with environmental modification or no intervention, but some may require treatment.
- Most cases of nappy rash are due to irritation and maceration, but Candida albicans infection, seborrhoeic dermatitis and psoriasis are other common causes.
- Not all babies with seborrhoeic dermatitis recover; one-third will develop psoriasis and another third, atopic dermatitis.
- The early signs of psoriasis in children include cradle cap, nappy rash, and post- and infra-auricular scaling and fissuring.
- Childhood-onset psoriasis, ichthyosis vulgaris and keratosis pilaris are often confused with atopic dermatitis.
- Urticaria is the only childhood skin condition that is effectively treated with antihistamines.
- Hypersensitivity to insect bites and plant contact dermatitis are common in children and preventative measures are often the best treatment.
The earliest dermatoses seen in infants other than atopic dermatitis are nappy rash, seborrhoeic dermatitis and neonatal acne. In preschool-aged children, florid insect bite reactions may be a problem. Skin conditions that are often confused with atopic dermatitis are childhood-onset psoriasis and the keratinisation disorders, ichthyosis vulgaris and keratosis pilaris. The most common allergic skin conditions in children, other than insect bite reactions, are virally induced urticaria and contact allergy to plants.
Early dermatoses
Nappy rash
Nappy rash is the term used to describe any rash occurring in the area under the nappy. It has become less common, probably due to the use of highly absorbent disposable nappies.
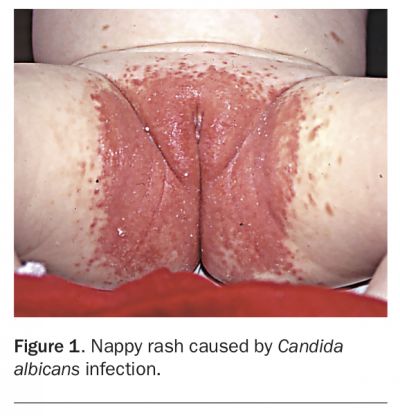
A simple irritant dermatitis is the most common cause of nappy rash, but there are many other causes, including Candida albicans infection (Figure 1), seborrhoeic dermatitis and psoriasis (Figure 2). There are also some very rare causes, such as zinc deficiency and Langerhans cell histiocytosis, and thus any infants with a severe, nonresponsive rash, particularly with lesions in areas other than under the nappy, should be referred to a dermatologist. Nappy rash can be mild or it can become so inflammatory that ulceration occurs. Rarely, it may become papular or nodular and result in lesions that can appear alarming. This condition is called pseudoverrucous papules and nodules (PPN).1
{kind=link}
{kind=link}
Generally, a simple irritant rash does not involve the flexures, whereas endogenous dermatoses and infections do. Irritant nappy rash results from loss of barrier function of the epidermis due to maceration from urine and irritation from faecal enzymes. Sometimes topical products, including soap and over-the-counter treatments, aggravate the rash. In many cases of nappy rash, the affected area is colonised with C. albicans.
Management
Generally, management for all forms of nappy rash is the same, even when the rash is very severe. Treatment involves environmental modification and specific medical management. Highly absorbent disposable nappies are preferable to cloth nappies. If cloth nappies are used, parents should be advised to change them every two hours and avoid using plastic overpants and nappy liners. As with any sort of dermatitis, a soap substitute should be used instead of soap and a dispersible bath oil used in every bath. At each nappy change, a damp cloth and bland emollient should be used instead of commercial wipes, and further emollient applied. Zinc and castor oil preparations are popular as a nappy rash treatment, but any greasy emollient is effective.
In many cases, environmental modification alone is inadequate and the medical treatment of choice is 1% hydrocortisone cream used in conjunction with a topical antifungal such as nystatin or an imidazole (clotrimazole or miconazole). There are several combined products, such as clotrimazole plus hydrocortisone, which are convenient and not much more expensive. The treatment should be used three times daily until the rash has resolved. Generally, hydrocortisone 1% is the only corticosteroid that should be used in the nappy area.
Inadequate response to treatment may be due to:
- noncompliance with treatment
- irritancy or allergy from topical therapy
- bacterial or viral infection
- psoriasis
- an underlying rare condition.
Pustules, erosions, vesicles, ulcers or areas of weeping may indicate a bacterial or viral infection, particularly in infants in whom there has been an inadequate response to therapy. A bacterial, and possibly a viral, swab should be taken and treatment started according to culture and sensitivity results. C. albicans will grow from a bacterial swab.
In the very rare instance of a herpetic infection, no specific treatment is needed, as the lesions will heal spontaneously within two weeks. If the infection is severe with ulceration or urinary retention, the infant may need to be admitted to hospital for intravenous aciclovir.
Seborrhoeic dermatitis
Seborrhoeic dermatitis is the term used to describe a clinical presentation that may occur in three common infantile dermatoses: idiopathic seborrhoeic dermatitis, atopic dermatitis and psoriasis. The eruption is seen most often before 2 months of age. Initially, the face, scalp, neck, axillae and nappy areas are involved, but the rash may generalise (Figure 3). The lesions are well defined and have a greasy scale. Characteristically, babies with seborrhoeic dermatitis are well and not itchy.
{kind=link}
The rash in classic, idiopathic seborrhoeic dermatitis is self-limiting, clearing spontaneously in a few weeks or sooner if treated. However, both atopic dermatitis and infantile psoriasis may also present in this way, and in these cases, the rash recurs. In about one-third of cases, seborrhoeic dermatitis will remit completely and the babies will have no further problems with their skin; in the other two-thirds, psoriasis or atopic dermatitis will develop. Infection with either C. albicans or Staphylococcus aureus is common; it should be suspected if crusting, weeping or pustulation are present and actively treated.
Very rarely, Langerhans cell histiocytosis (an increase in Langerhans cells in the skin) may simulate seborrhoeic dermatitis. The cause for this is unknown. In small children it may cause death as the infiltrate may also involve internal organs. The condition is differentiated from seborrhoeic dermatitis by the presence of purpura and erosions as well as treatment resistance.
Management
Management of seborrhoeic dermatitis is essentially the same as that for atopic dermatitis.2 Scalp scaling responds to treatment with liquor picis carbonis (LPC, or coal tar solution) 2% and salicylic acid 2% in a moisturising base, and the nappy area is treated with a combination of 1% hydrocortisone and an anticandidal cream, such as nystatin or an imidazole. It is a good idea to follow up the infant to ensure that this is not the first presentation of a chronic dermatosis such as atopic dermatitis or infantile psoriasis.
Childhood acne
Acne is usually thought of as a condition seen in teenagers, but it may also occur in babies and prepubertal children. Because acne is an androgen-dependent condition occurring in genetically predisposed patients, it may be seen in children at times when there is a high enough androgen level to permit expression of the tendency. Neonatal acne is the term used to describe acne occurring in the first two years of life. The acne is often predominantly comedonal and its onset is soon after birth. It is more common in boys, varies in severity and often needs no treatment, but it can be severe enough to cause scarring. Parents should be warned that neonatal acne may, and often does, recur at puberty. Children with early onset acne usually go on to suffer from teenage acne.
Acne is also seen in prepubertal children after the age of 8 years, when the androgens secreted at adrenarche stimulate sebaceous glands in predisposed individuals. It is not usually necessary to investigate for androgen excess unless there are other concerning signs such as excess facial hair. Acne presenting for the first time after 12 months of age and before the age of 8 years raises the possibility of androgen excess. Such patients should be referred to a dermatologist or an endocrinologist.
Management
Neonatal acne is self-limiting and usually remits by 12 months of age, but it may persist to 24 months. If treatment is needed, topical therapy usually used for mild teenage acne is appropriate. This includes topical tretinoin 0.025% cream once daily and erythromycin 2% gel once daily. Rarely, neonatal acne may be nodulocystic and can be treated with oral isotretinoin to prevent permanent scarring. In this case referral to a paediatric dermatologist is required.3 For prepubertal children with acne, topical therapy is also often adequate. Oral antibiotic therapy is usually not required, but in severe cases, oral erythromycin may be used (tetracycline is contraindicated in this age group because it may stain teeth).
Other childhood rashes
Psoriasis
Although psoriasis is less common in children than in adults, up to 30% of cases have their onset in childhood and in about 5% the onset is before the age of 2 years. The average age of diagnosis in childhood cases is about 8 years.
There are surprisingly few meaningful studies on the incidence, prognosis and nature of childhood psoriasis. We know little about how likely it is to remit compared with the disease in adults, and this is largely because there is no definitive definition for childhood psoriasis. In many studies, the diagnosis is usually clinical and, therefore, open to interpretation. A recent publication has sought to clarify how to differentiate childhood psoriasis from eczema (Box).4
{kind=link}
The earliest sign that a child is destined to suffer from psoriasis is often cradle cap or persistent nappy rash that typically involves the flexures and has a well-defined edge. The term ‘napkin psoriasis’ refers to a psoriatic nappy rash associated with cradle cap, plaques on the trunk and axilla and often a facial rash, particularly on the cheeks.
In children, psoriasis may present with the typical plaques seen in adults (Figure 4a); however, these are usually smaller, thinner and less scaly. Acute guttate psoriasis with eruption of small lesions after a streptococcal throat infection is a frequent presentation. Common presenting sites include the scalp, retroauricular folds, face, flexures and genital areas. Scalp scaling and a persistent retroauricular rash or infra-auricular fissuring are common and often subtle signs. Acral psoriasis with nail dystrophy (Figure 4b) and erythema and scaling of the fingertips may occur, and may involve only one or a few digits. However, the most common nail change is pitting, and is a useful diagnostic clue. Unusual presentations include persistent rashes on the palms and soles (Figure 4c), intertrigo of the hands and feet (Figure 4d), follicular eruptions, persistent angular cheilitis and blepharitis.
{kind=link}
Rarely, acute pustular psoriasis may occur in children, with sudden onset of widespread erythema studded with sheets of pustules and associated fever and systemic toxicity. Children with this condition should be admitted to hospital and monitored for systemic infection and evidence of dehydration. Mild topical corticosteroids, wet dressings and oral antibiotics are used for treatment. Recovery may take several weeks.
In some children, psoriasis and atopic dermatitis occur together. This is not surprising, considering how common each is, and recent evidence suggests they may be linked genetically in some patients. When this occurs, typically there are eczematous lesions in the cubital and popliteal fossae, but also psoriatic plaques on the dorsal surface of the elbows, knees and other typical areas such as the scalp. Parents will often relate that the dermatitis component clears easily and promptly with topical corticosteroid, while other lesions are resistant to treatment. Concurrent psoriasis is one of the most common reasons for ‘nonresponsiveness’ in treating atopic dermatitis.
In children a common precipitant of psoriasis is streptococcal throat infections. Stress and trauma may also play a part, as they do in adults.
Psoriasis is an unpredictable, recurrent or chronic condition. It is seldom severe in children, and psoriatic arthritis is very uncommon.
Management
Management of psoriasis in children may vary depending on the site, nature and severity at different stages. It is important that treatment is individualised. Almost all of the topical therapies used for adult psoriasis may be used in children.
Generally, topical coal tar preparations are safer in the long term and usually more effective than topical corticosteroids for treating psoriasis in children. There are drawbacks, however, and irritancy, cost and poor patient acceptance because of their odour may limit their use. Tars are usually started at a strength of 4% LPC on the body and limbs. This may be increased up to 10% LPC with the addition of salicylic acid to reduce scale, but this is not often required. Weak tars, usually no more than 2% LPC, may be used on the face and flexures. Tar treatment needs to be carefully monitored but when tolerated and used persistently is very rewarding. Topical corticosteroids may be used in conjunction with tars, particularly where the rash is itchy.
Calcipotriol combined with betamethasone dipropionate has good patient acceptance because of its lack of odour and can be more effective than topical corticosteroid monotherapy. It is usually well tolerated. It is too potent to use on the face and flexures in children but is useful on the trunk and limbs.
Topical pimecrolimus may also be useful for psoriasis affecting the eyelids but in general is too weak to be effective. Narrow band UVB phototherapy, oral retinoids, methotrexate and ciclosporin A may be used in very severe cases of childhood psoriasis, but this situation rarely arises and if it does, the patient needs to be referred to a paediatric dermatologist.
When an attack of psoriasis has been precipitated by a streptococcal infection, the infection should be treated with oral antibiotics. Eradication of streptococci will not always improve the psoriasis. In some patients, psoriasis is exacerbated by chronic or recurrent streptococcal infections, particularly of the ear, nose and throat. In these patients there may be a role for prophylactic antibiotics and some benefit from tonsillectomy.
Response to psoriasis treatment is typically slow, much more so than to atopic dermatitis treatment. This is because psoriasis is a hyperproliferative rather than an inflammatory condition. The normal turnover time of the epidermis is about six weeks, and this is usually the minimum time needed to obtain a good response from any treatment aimed at treating the rash. Unless patients are warned of this, many will give up long before their treatment has had a chance to become effective (see the Patient and Carer Handout). Once the rash has cleared, preventative treatment with tar ointments can be effective at maintaining remission, and topical corticosteroids should be restarted at the first sign of any new lesions.
Treatment of psoriasis can be complex, and if a patient’s response is particularly slow, referral to a dermatologist is recommended.
Pityriasis alba
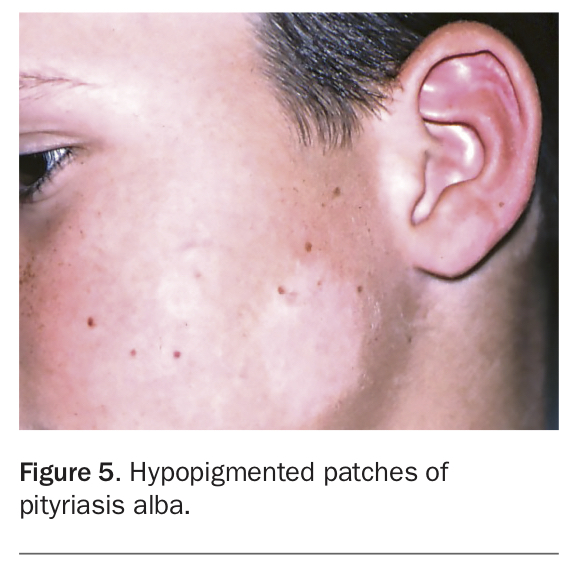
Pityriasis alba is a common mild form of dermatitis in which postinflammatory hypopigmentation is marked. Patients present with poorly defined hypopigmented scaly patches on the face (Figure 5). It is most obvious in summer, when the skin is tanned, and in dark-skinned children, and it is more common in children with atopy. Usually, symptoms are minimal.
{kind=link}
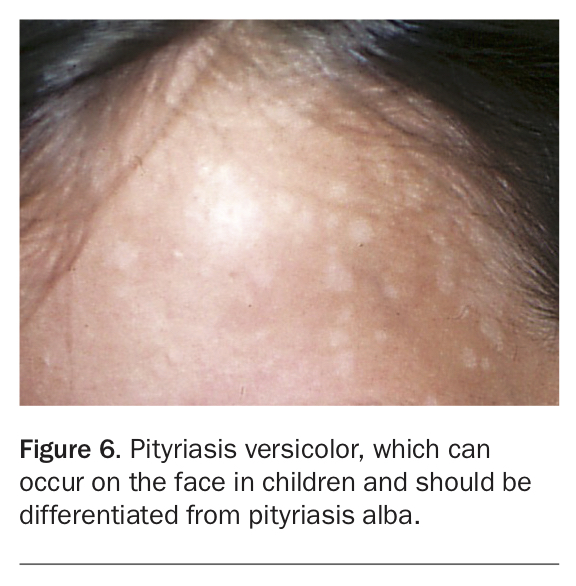
Pityriasis alba must be differentiated from pityriasis versicolor, a fungal skin condition that, in children, typically occurs on the face (Figure 6). Vitiligo should also be considered as a differential diagnosis but is not scaly and has a very sharp border, with obvious depigmentation rather than hypopigmentation.
{kind=link}
Management
It is often not necessary to treat pityriasis alba, as it is more a cosmetic than symptomatic problem. Avoidance of skin irritants such as soap and shampoo and use of a soap substitute as well as an emollient twice daily are often all that is needed.
Hydrocortisone ointment 1% twice daily will settle irritation and scaling but will not restore pigmentation. This requires graduated sun exposure to the pale areas while using a sunscreen daily to avoid excess tanning of the skin that is not affected. As this is quite difficult to do, it is often better to ignore the condition, which improves with age.
Ichthyosis
Ichthyosis is a genetically determined skin condition. It presents at or soon after birth and persists throughout life. Affected patients have chronically dry, scaly skin.
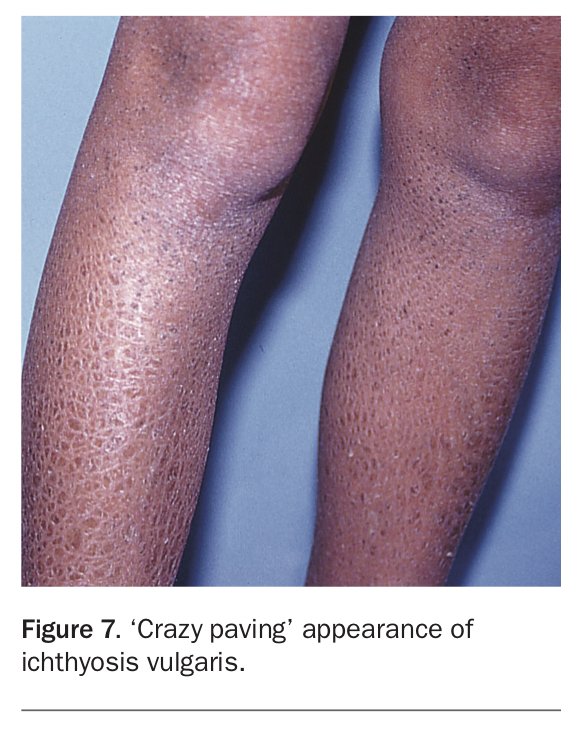
Ichthyosis is often confused with atopic dermatitis, but it lacks the itch and inflammatory component (unless there is concomitant atopic dermatitis). There are many forms, dominantly inherited ichthyosis vulgaris, X-linked and a number of recessively inherited forms. Most are quite rare; ichthyosis vulgaris is the most common. In patients with ichthyosis vulgaris, the skin surface is dry and scaly. This may be obvious only on the lower legs. Additionally, these children have ‘hyperlinear’ palms and soles; in other words, the normal lines seen on these surfaces are accentuated. In the more severe X-linked ichthyosis, seen only in boys, the lower legs may exhibit a ‘crazy- paving’ appearance (Figure 7) and the whole skin may be dry, particularly early in life. All forms of ichthyosis are more troublesome in dry, cool weather. The recessive ichthyosis skin dryness is of a degree that will not be confused with eczema and patients’ very abnormal skin is usually obvious from birth, when most present as ‘collodion babies’ with an appearance of being encased in plastic wrap as neonates.
{kind=link}
Management
Treatment of ichthyosis consists of avoidance of products that dry the skin, such as soap, shampoo and bubble bath. A dispersible bath oil and moisturiser need to be used daily and can make the skin appear relatively normal. Generally, greasier preparations are more useful, particularly in winter. Excess scale may be removed with a preparation containing a keratolytic such as urea 10%, salicylic acid 2 to 6%, lactic acid 10% or propylene glycol 10 to 20%. Urea cream containing sodium pyrrolidone carboxylate is particularly useful. However, keratolytics may cause stinging and may be poorly tolerated by children. Topical corticosteroids are not required in the treatment of ichthyosis unless there is also atopic dermatitis.
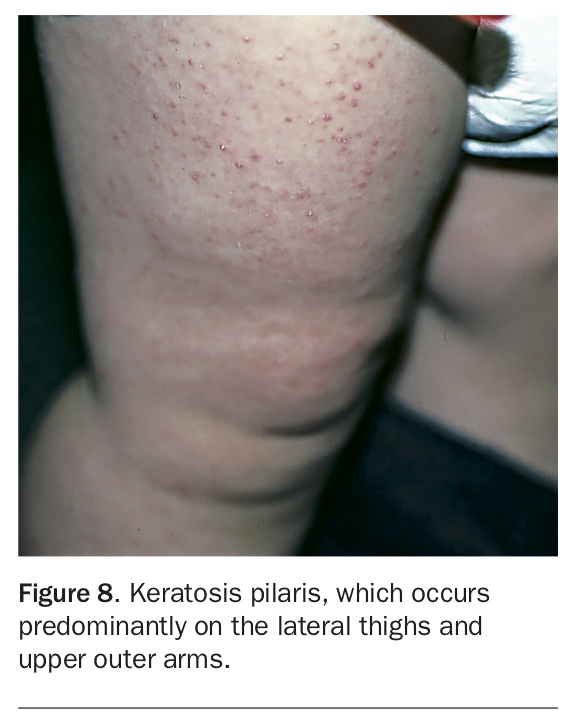
Keratosis pilaris
Present in about 50% of the population, keratosis pilaris is a very common, dominantly inherited condition. It comprises very small keratotic papules found predominantly on the upper outer arms and lateral thighs (Figure 8). It is often also found on the cheeks in young children. Rarely, it generalises and is then termed follicular ichthyosis. Sometimes the lesions appear pustular but are usually sterile.
{kind=link}
Keratosis pilaris is asymptomatic. Some parents see it as a cosmetic problem and a few are truly distressed by it. Occasionally, it may appear erythematous, which can be a cosmetic problem, particularly if it is on the face. Sometimes it is confused with dermatitis and inappropriately treated with corticosteroids.
The prognosis of this condition is good. The facial papules disappear around puberty, and although the lesions elsewhere may be most prominent in the second decade, they become less obvious with advancing age.
Management
Keratosis pilaris is a normal variant. It is difficult to treat effectively and is best ignored. If treatment is desired, keratolytics such as urea, salicylic acid or glycolic acid can be used overnight in combination with an abrasive therapy (e.g. an abrasive sponge or facial scrub) in the shower in the morning. Care should be taken when using these topical preparations in children as they may sting or cause redness, irritation or dryness.
If facial redness is a problem, keratosis pilaris can be treated with vascular laser, although the results are variable. This treatment is uncomfortable and expensive, requiring a general anaesthetic in most children. It may be best, therefore, to wait until patients are old enough to make the decision for treatment themselves. Unless very highly motivated, most patients tire of topical treatment eventually and accept the condition.
Common allergic rashes
Papular urticaria
The term papular urticaria is used to describe hypersensitivity to insect bites, usually from mosquitoes and fleas. It is a misleading term, as it bears no relation to ordinary urticaria and the condition is not helped by antihistamines.
Seen in young children aged between 2 and 6 years, papular urticaria usually occurs in spring and summer. The lesions most often occur on exposed surfaces (Figure 9), although fleabites usually occur under clothes. Individual lesions are intensely itchy papules, blisters and crusts. Scratching leads to excoriation, infection and ulceration that may result in scarring and hypopigmentation. The prognosis of this condition is good, with most children becoming hyposensitive to the bites after two to four years. In children of any age, grass ticks can also produce very persistent itchy papular rashes.
{kind=link}
Management
The best approach in regard to papular urticaria is prevention with insect repellent, protective clothing and insect control, using insecticide, screens and treatment of pets. These strategies must be maintained throughout spring and summer. If infection occurs, it can usually be treated with topical antibiotic ointment and itch can be relieved with topical corticosteroid. It is best to use a potent corticosteroid and to cover the lesions with a dressing to prevent excoriation. In areas where grass ticks occur, avoidance of playing outside is the best prevention.
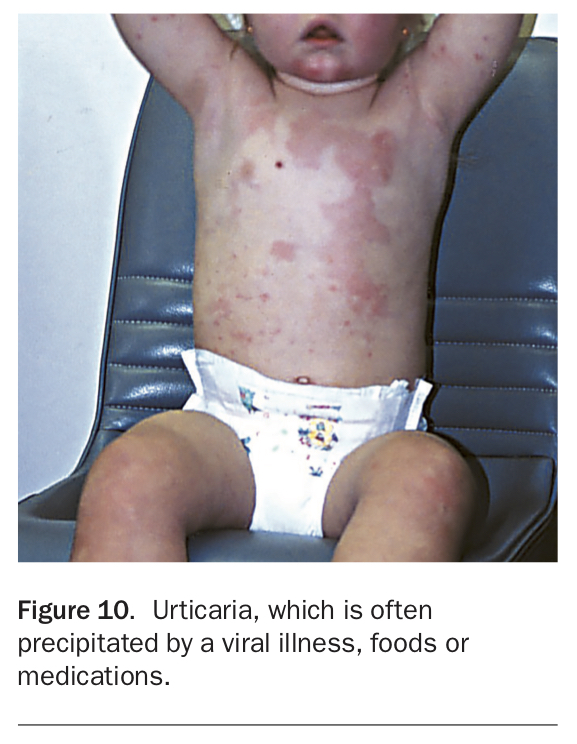
Urticaria
Urticaria (hives) is most often a benign, self-limiting, condition in children (Figure 10). The most common precipitant is a preceding or current viral illness but foods and medications can be less often involved. Intestinal giardiasis may cause urticaria and, occasionally, urticaria may be a complication of scabies and fungal infections. Extensive systemic investigations are rarely indicated for children with this condition.
{kind=link}
Management
The best approach to urticaria management is simply to treat children empirically with an oral nonsedating antihistamine such as cetirizine or loratadine for two weeks or until the rash has resolved, and then gradually withdraw it. If the rash recurs, the antihistamine can be restarted and an attempt made to withdraw it every two weeks. If urticaria persists for more than six weeks, it is worth excluding giardiasis, and an elimination diet may be considered. In children, this is best done with the help of a dietitian with an interest in food allergy.
Antihistamines have been linked to sudden infant death syndrome in children under 2 years of age and should only be used in children younger than 12 months if the rash is very distressing; in this case only a nonsedating preparation should be used.
Plant dermatitis
Acute contact dermatitis from touching allergenic substances is not common in children as they have much less contact with potential allergens than adults. However, children are more prone than adults to have contact with plant allergens, which may occur while they are playing outside.
Although the rhus tree (Toxicodendrom succedaneum) was once a well-known culprit of plant dermatitis, this has now been declared a noxious weed, and many of these trees have been removed. They are still found in some gardens, however, and have a potent allergen that cross-reacts with the allergens in the ubiquitous plant genus grevillea. Grevillea is currently the most common plant allergen for children.
Grevillea Robyn Gordon, an attractive hardy plant with red flowers, used to be quite ubiquitous but has been removed from public places because of the problem of allergy. Other grevillea varieties such as Superb, Ned Kelly and the silky oak tree are close relatives, and the allergens of these all cross-react with each other.
Allergic contact dermatitis presents with an intensely itchy and often blistering rash. It may cause significant oedema on the face and around the genital area. It often has a streaky, asymmetrical pattern, reflecting where the plant brushed against the skin (Figure 11). Often contact has been very brief and is not remembered by the child.
{kind=link}
Management
If untreated, lesions of plant dermatitis tend to keep appearing for several days and may take weeks to resolve. They respond well and rapidly to a short course of oral prednisone, starting with 0.5 mg/kg/day until settled then reducing the dosage over two weeks. An attempt should be made to identify the cause. This can be confirmed by applying a tiny bit of the plant to the skin, which will rapidly reproduce the rash. Take care when doing this as there is a risk of a severe reaction. Do not occlude the plant, and leave it on the skin for only five minutes.
Conclusion
Not all childhood skin conditions are atopic dermatitis, even though this is by far the most common problem. Nappy rash is rarely atopic and is more likely to indicate simple irritation, seborrhoeic dermatitis, C. albicans infection or psoriasis. Several endogenous dermatoses that can present in childhood are often confused with atopic dermatitis, including psoriasis, ichthyosis vulgaris and keratosis pilaris. Psoriasis is the most important of these, and many patients with ‘treatment resistant atopic dermatitis’ presenting to paediatric dermatologists turn out to have psoriasis. Pityriasis alba is a very common and harmless childhood facial depigmenting dermatosis that is most often confused with pityriasis versicolor and vitiligo, both of which are much less common. Acne may occur in babies, most often boys, and is not a cause for concern. The most common allergic rashes in children include florid reactions to insect bites, contact dermatitis from plants and urticarial reactions to viral illnesses. MT