Vaping in young people: lives up in smoke

Dr Palit is a Fellow in Paediatric Respiratory Medicine at Royal Children’s Hospital, Melbourne; and a Senior Lecturer in Health Services Management, School of Population Health, UNSW Sydney.
Dr Milne is a Staff Specialist in Adolescent and Addiction Medicine at the CICADA Centre (Care and Intervention for Children and Adolescents affected by Drugs and Alcohol), Sydney Children’s Hospitals Network, Sydney, NSW.
Dr Vandeleur is a Staff Specialist in Respiratory and Sleep Medicine at Royal Children’s Hospital, Melbourne, Vic.
Adolescent health

E-cigarette use (‘vaping’) is increasing among adolescents and young people in Australia but carries significant health risks and is subject to strict regulations. GPs are well positioned to identify their young patients who use e-cigarettes, assess and intervene early to help reduce vaping-related harms.
Note
The report of an Australian case of EVALI (e‐cigarette or vaping product use‐associated lung injury) referred to in this article was published on 4 October 2021. The online full text and PDF versions (see link above) of this article have been updated with the reference.
- E-cigarette use (‘vaping’) is increasing in popularity among young people in Australia.
- Vaping is associated with multiple adverse health effects, including increased risks of respiratory illness, cardiovascular disease and nicotine addiction, and there is growing evidence that e-cigarette use is a precursor to conventional tobacco smoking.
- Australia has a strong regulatory framework that limits the use, supply and availability of e-cigarettes and vaping devices.
- Assessment of young people is key to preventing harms - ask about vaping, screen for patterns of use and assess risk to identify any comorbid physical or mental health issues.
- E-cigarettes should not be recommended as smoking cessation aids in young people.
The uptake of e-cigarette use, or ‘vaping’, among adolescents and young people in Australia is a problematic trend. Although e-cigarettes are touted as a safer alternative to tobacco smoking and glamourised on social media, they have significant health risks.
This article aims to inform GPs about the health risks of vaping and the regulatory framework for vaping in Australia, including recent legislative changes. It outlines an approach to assessment and intervention in young people who use e-cigarettes. Engaging young people, educating them about the harms and intervening early offers the greatest opportunity for positive behaviour change in adulthood. Working together across health and social care, we can prevent a new generation being exposed to the adverse effects of nicotine.
What are e-cigarettes?
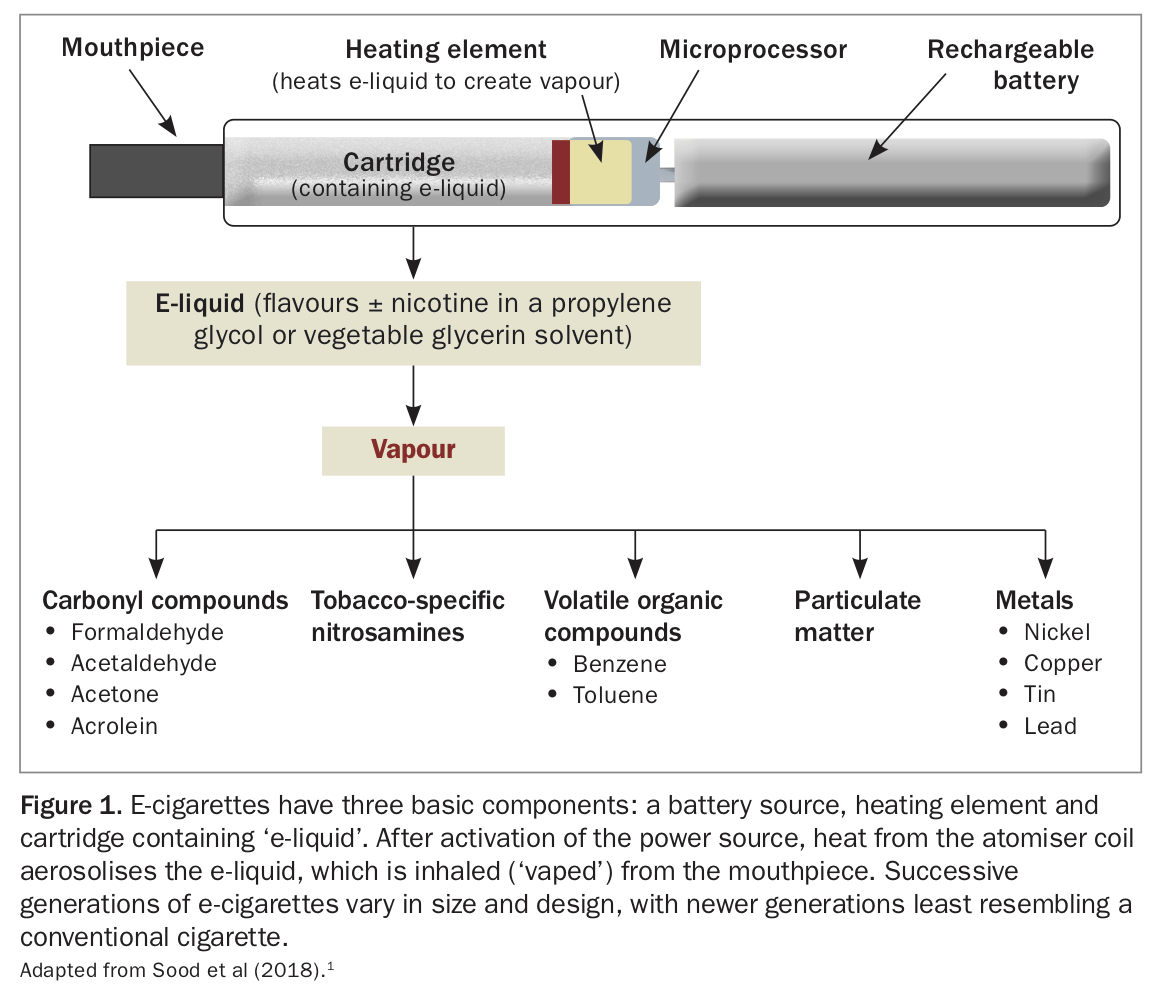
E-cigarettes are battery-operated devices that come in many shapes and sizes but have the same basic components (Figure 1).1 They produce an aerosol by heating a liquid, known as e-liquid or e-juice, to produce vapour that users inhale, commonly referred to as vaping. E-cigarettes are also known as e-cigs, e-hookahs, mods, vape pens, vapes, juuls, tanks, sticks, stigs and, in academia, electronic nicotine delivery systems (ENDS). The composition of e-liquid varies, but it typically contains solvents, additives and flavouring agents and may or may not contain nicotine.
{kind=link}
Vaping prevalence in young people in Australia
Vaping has increased in popularity around the world, fuelled by youth-friendly flavours, directed advertising on social media and new types of e-cigarettes aimed at young people. Although Australia has one of the lowest rates of adolescent cigarette smoking, with fewer than 2% of 12 to 17-year-olds reporting regular tobacco use, there has been a steady increase in the number of young people using e-cigarettes.2 Among Australian secondary school students in 2017, 14% reported they had ever used e-cigarettes.3 Ever-use increased with age, from 5% of 12-year-olds to 22% of 17-year-olds. Boys were significantly more likely than girls to report ever-use. About 37% of 12 to 15-year-old users and 27% of 16 and 17-year-old users reported vaping at least once during the previous month.3
The Australian National Drug Strategy Household Survey asked respondents about vaping for the first time in 2013, and then in 2016 and 2019.2 Lifetime e-cigarette use was reported by 9.6% of adolescents aged 14 to 17 years, rising to 26.1% of 18 to 24-year-olds, the highest reported usage in all age-groups. Vaping use was over-represented among nonsmokers aged 18 to 24 years, rising from 4.9% in 2013 to 19.6% in 2019.2
It is increasingly apparent that young people vape for many of the same reasons people smoked decades earlier: social acceptance, novelty, celebrity influence, sophistication and rebellion. Driven by pop-savvy industry, sophisticated marketing and peer influence, behaviours such as sharing of vapes, experimenting with flavours and perfecting tricks has contributed to the emergence of a subculture of youth vaping.4,5 A case in point is the rise of single-use ‘puff-bars’, disposable vapes with a high nicotine concentration that come in flavours and colours that appeal to youth.
Harms associated with vaping
Health risks of e-cigarette aerosols
E-liquids commonly contain a pharmacologically active agent, usually nicotine or cannabinoids such as tetrahydrocannabinol (THC), dissolved in a solution consisting of glycerin, propylene glycol and a wide range of flavouring agents.6 Depending on the combination of solvents and flavours used, toxins detected in the resultant aerosol can include carcinogens such as formaldehyde, acetaldehyde, acetone and acrolein; volatile organic compounds such as benzene and toluene; tobacco-specific nitrosamines; particulate matter; and metals such as nickel, copper, zinc, tin and lead.1
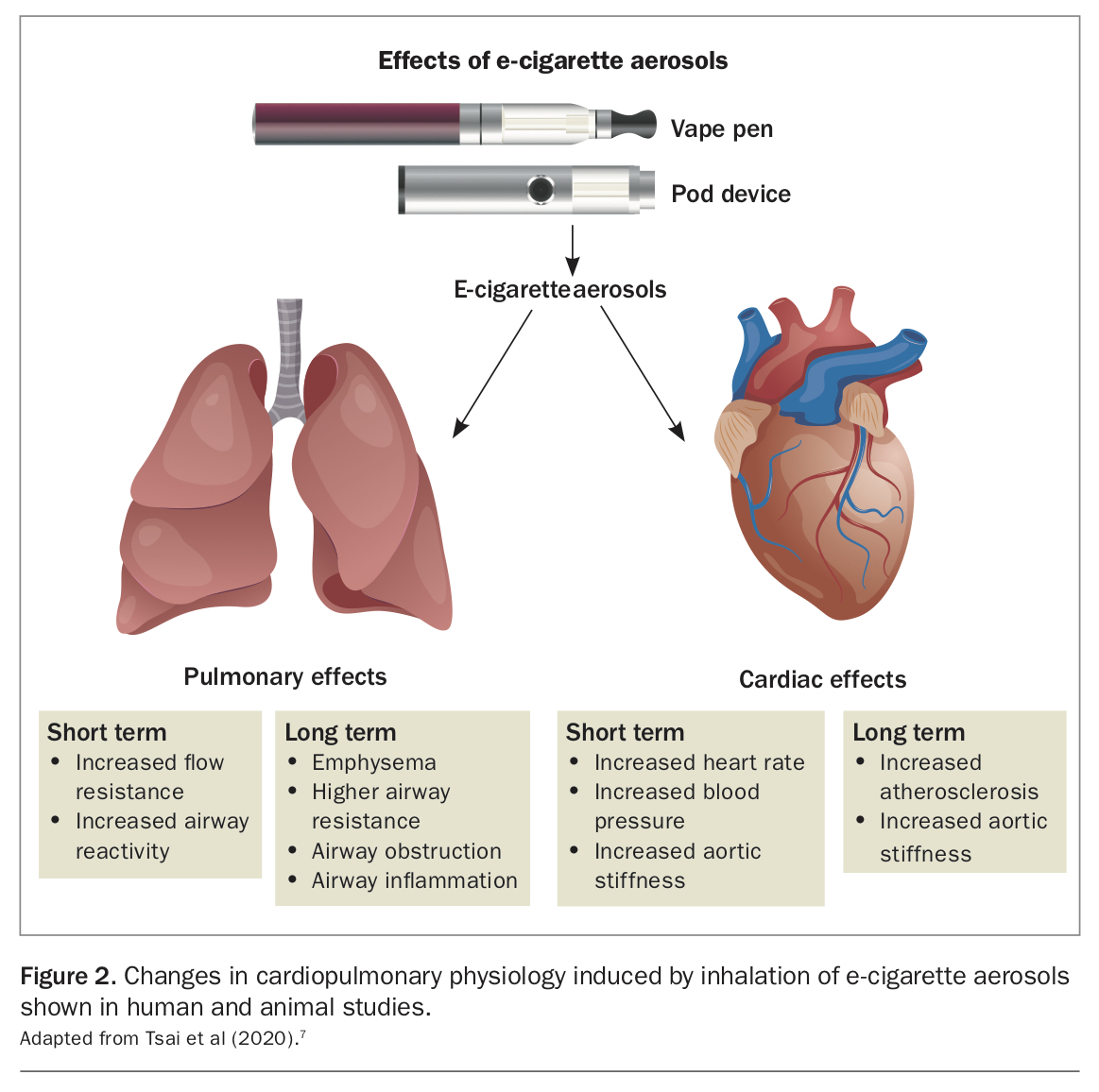
The long-term risks of vaping are still largely unknown; however, studies have shown that exposure to e-cigarette vapour can lead to cellular toxicity, cellular dysfunction, alterations in cellular metabolism and repair mechanisms and inflammation through changes to both protein function and gene expression pathways.4 Studies of acute and subacute e-cigarette exposure in humans suggest that vaping affects lung health, inducing pathological changes and inflammatory processes in the small airways that can exacerbate both asthma and chronic obstructive pulmonary disease. Similarly, sustained exposure to e-cigarette aerosols containing nicotine increases heart rate, blood pressure and airway resistance, contributing to the development of long-term cardiovascular disease (Figure 2).7
{kind=link}
More than 20,000 flavours are on the market.4,8 Although many flavouring agents are approved by the TGA and widely used in the food industry, their intention was for gastrointestinal consumption, not inhalation.
Further, from our experience and literature reports, young people who vape often make their own e-liquids, incorporating substances such as THC or cannabidiol oil.1,4,6,9 These devices, their contents and aerosols will contain known and unknown harmful chemicals, and patients may present with a range of systemic effects associated with drug toxicity, poisoning and overdose.
E-cigarette or vaping use-associated lung injury
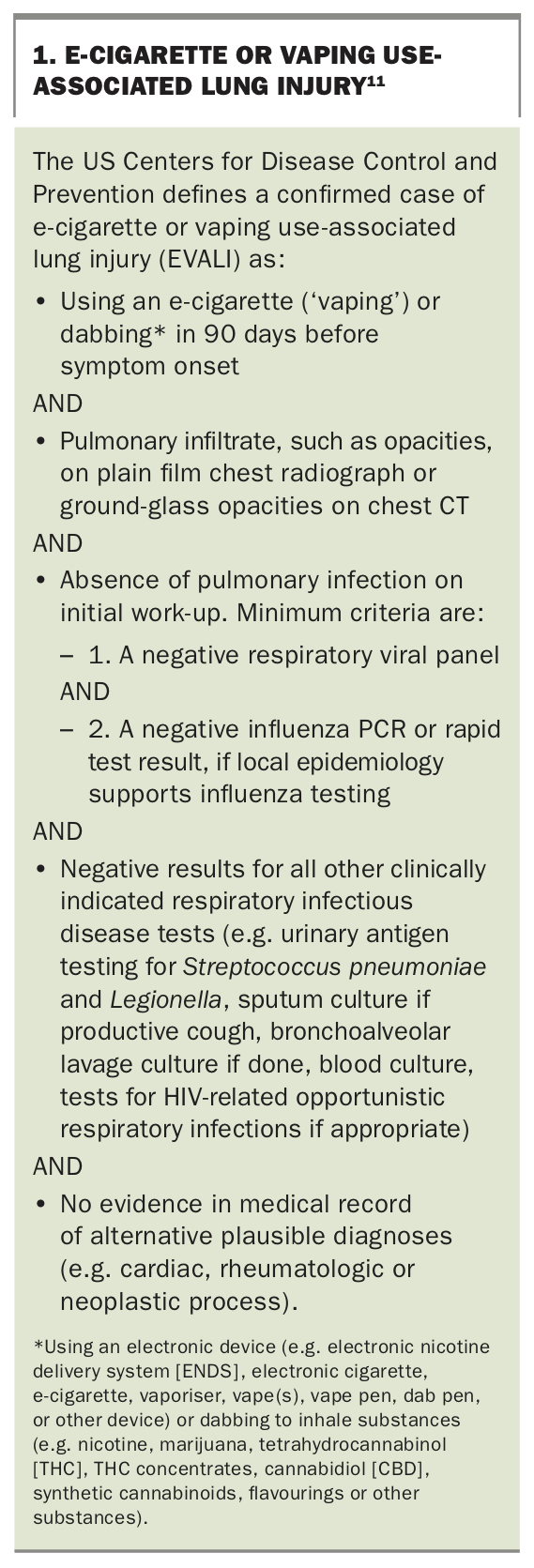
By February 2020, at the height of the US vaping ‘epidemic’, a total of 2807 cases of e-cigarette or vaping use-associated lung injury (EVALI) and at least 68 associated deaths had been reported to the US Centers for Disease Control and Prevention.10 EVALI is an evolving syndrome associated with recent vaping use that comprises a mixture of nonspecific systemic symptoms (e.g. fever, chills, diarrhoea and vomiting) and respiratory symptoms (e.g. dyspnoea, cough, chest pain and hypoxia), along with detection of lung opacities on imaging (Box 1).11
{kind=link}
Laboratory data and several case series involving analysis of bronchoalveolar lavage fluid samples from patients who presented with significant respiratory compromise showed that vitamin E acetate, an additive in some THC-containing vaping products, was strongly linked to the EVALI outbreak.10 We are aware of at least one case of an adolescent severely unwell with EVALI in Australia.12 EVALI is likely under-reported and should be considered in patients presenting with respiratory or systemic symptoms who report recent vaping use and no significant history of respiratory disease or infective symptoms.
Nicotine effects and addiction
Nicotine-containing e-cigarettes deliver nicotine by creating an aerosol of ultrafine particles. As well as having the side effects discussed above, nicotine is highly addictive and has effects on learning, attention and memory in the developing adolescent brain.13 Adolescents who are exposed to nicotine may become addicted more rapidly, and with lower consumption, than adults. Nicotine-containing e-cigarettes often deliver higher doses of nicotine than conventional cigarettes, and several exposures to high levels of nicotine can cause addiction. Other studies have shown that exposure to nicotine during adolescence can have a long-term negative impact on higher cognitive function.4,5,14,15 The US Surgeon General reported in 2016 that ‘nicotine exposure during adolescence can cause addiction and can harm the developing adolescent brain’.5
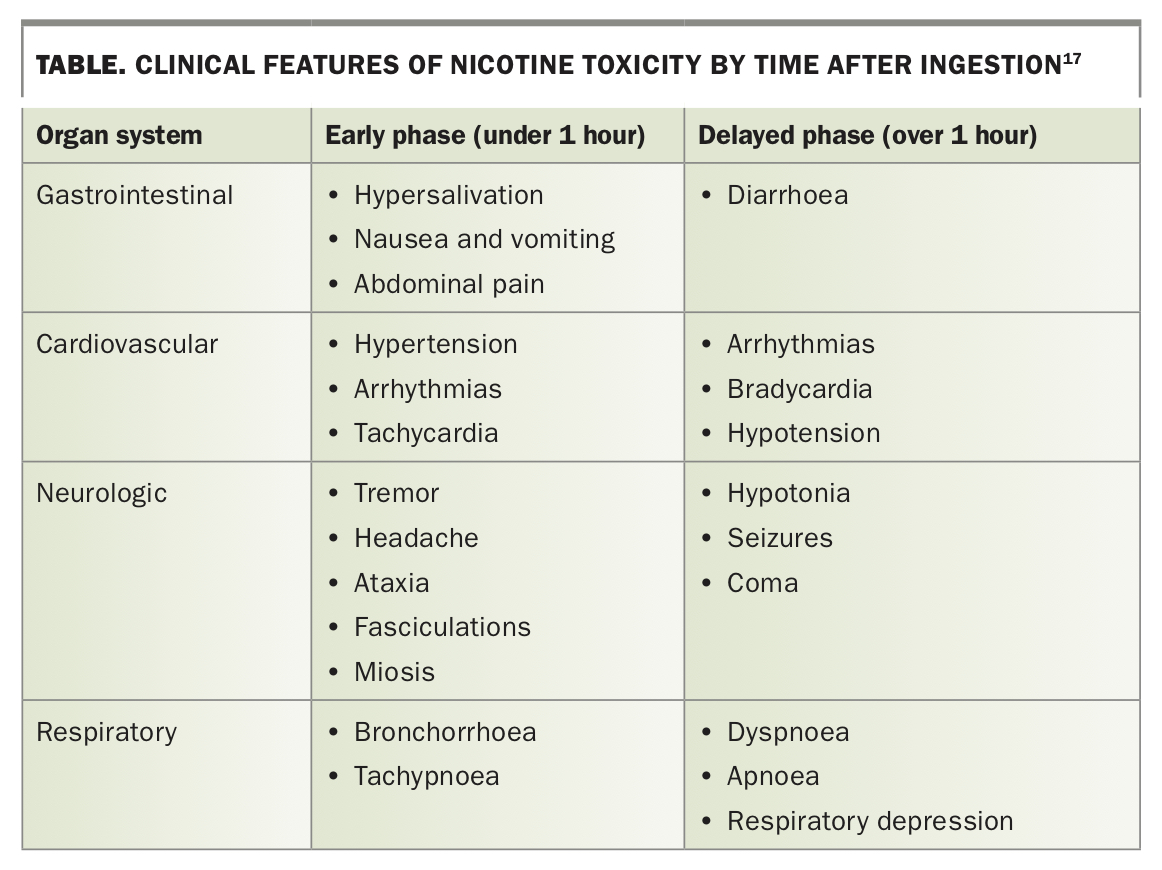
Nicotine-containing e-liquid also has the potential to cause poisoning if swallowed or absorbed through the skin. Acute nicotine toxicity has a biphasic pattern, owing to its short half-life of one to four hours.16 The clinical effects of the early and delayed phases of nicotine toxicity are shown in the Table.17 The risk of accidental injury with nicotine-containing e-liquid is high because of a lack of minimum product standards for e-liquid containers, meaning they may leak, are easily opened and can have much higher concentrations of active ingredients than reported.10,18 There have been several reports of accidental and intentional overdose with nicotine e-liquid, resulting in severe toxicity and, in some cases, death.19 In 2018, a toddler died in Australia after accidentally ingesting high-concentration liquid nicotine at home, originally imported from overseas by his parents for use in e-cigarettes.20
{kind=link}
Passive exposure
As with conventional tobacco smoking, secondhand exposure to e-cigarette vapour and inhaled toxins has the potential to pose a health risk to bystanders. Additionally, exposure to certain metals such as nickel and silver may be greater for e-cigarettes than for tobacco cigarettes. The most common symptoms reported by people passively exposed to vaping products include headache, nausea, eye irritation, sore throat and respiratory difficulties.21,22
Other adverse events
As the popularity of vaping has increased, serious adverse events have been reported related to their highly variable manufacturing quality. Over 200 incidents of vaping devices overheating, catching fire or exploding have been reported. In some cases, these events have caused significant injuries, disfigurement, disability and property damage.23
Regulatory framework for vaping
At a population level, one of the most pressing concerns about vaping is the renormalisation of smoking behaviours, which may lead to more young people taking up the habit and fewer adults quitting smoking. In response to this and the epidemic of youth vaping seen overseas, Australia has maintained a strong therapeutic framework for the regulation of vaping products. This approach recognises the need to prevent adolescents and young people taking up vaping and to reduce the role of e-cigarettes as gateway drugs to tobacco smoking. Primary care providers should be aware of the vaping regulations in Australia, both to educate and to advocate for their patients and families.
Supply and availability
- Vaping devices that do not contain nicotine are classed as consumer goods and captured under tobacco control laws. Accordingly, they are subject to the same restrictions as cigarettes (e.g. restricted for under 18-year-olds).
- The sale of nicotine-containing e-cigarettes and liquid nicotine is illegal without a prescription throughout Australia.
- From 1 October 2021, consumers will need a valid Australian prescription to import nicotine-containing e-cigarettes and liquid nicotine from overseas. This aligns with current domestic restrictions under state and territory laws prohibiting the supply of nicotine-containing e-cigarettes without a valid medical prescription.
- There are currently no vaping products listed on the Australian Register of Therapeutic Goods for supply. Consequently, ENDS can only be accessed via other means (e.g. personal importation, special access scheme or authorised prescribing scheme).9,18
Advertising and promotion
- Nicotine-containing e-cigarettes and liquid nicotine for smoking cessation are regulated as prescription medicines. The advertising of prescription medicines to consumers is generally prohibited in Australia.
- Most states and territories do not allow advertising of non-nicotine-containing vaping devices.
Sale and use
- Nicotine is classified as a Schedule 7 - Dangerous Poison under the Commonwealth Poisons Standard.
- In all Australian states and territories, it is an offence to manufacture, sell or supply nicotine as an S7 poison without a license or specific authorisation.9
- Vaping and e-cigarette use is generally subject to the same restrictions as smoking in public places.9
Pricing and taxes
- Vaping products in Australia are not subject to tobacco excise tax or minimum pricing.
Product standards
- The TGA is currently developing a product standard for nicotine-containing vaping products that are otherwise subject to general consumer safety laws.18
- Other countries have standards based on nicotine concentration limits (e.g. 20mg/mL in the European Union and UK), flavouring, additives and other features.
Packaging and labelling
- From 1 October 2021, all liquid nicotine products supplied in Australia require child-resistant closures to reduce the risk of accidental exposure or ingestion of nicotine.18
- Other considerations include safe storage instructions, warning statements (e.g. about addiction) and listing of active and excipient ingredients.9,18
Approach to address vaping in young people
All drugs should be considered 'gateway’ drugs. There are now strong data showing that e-cigarette use is a precursor to initiating cigarette smoking, particularly in young people.24 GPs, as primary care providers, are well positioned to ask adolescents about their vaping use and to assess for risk factors, nicotine dependence and adverse effects. A lack of familiarity with vaping devices, liquids and how they are used should not be a barrier to patients receiving appropriate care. Some useful resources on vaping for healthcare providers, parents and teenagers are listed in Box 2.
{kind=link}
GPs may be asked about e-cigarettes by patients, usually adults, who smoke and may be interested in using them to quit smoking. Young people may also seek prescriptions for nicotine vaping products so they can continue recreational vaping. The efficacy of e-cigarettes as a smoking cessation aid has not been fully established, whereas other smoking cessation interventions (e.g. nicotine replacement therapy in the form of gum, patches, sprays, inhalers or lozenges) are supported by an excellent evidence base. Further research is needed to assess the long-term safety and efficacy of e-cigarettes in harm minimisation.25,26 Consequently, we believe that e-cigarettes should not be recommended as smoking cessation aids for young people.
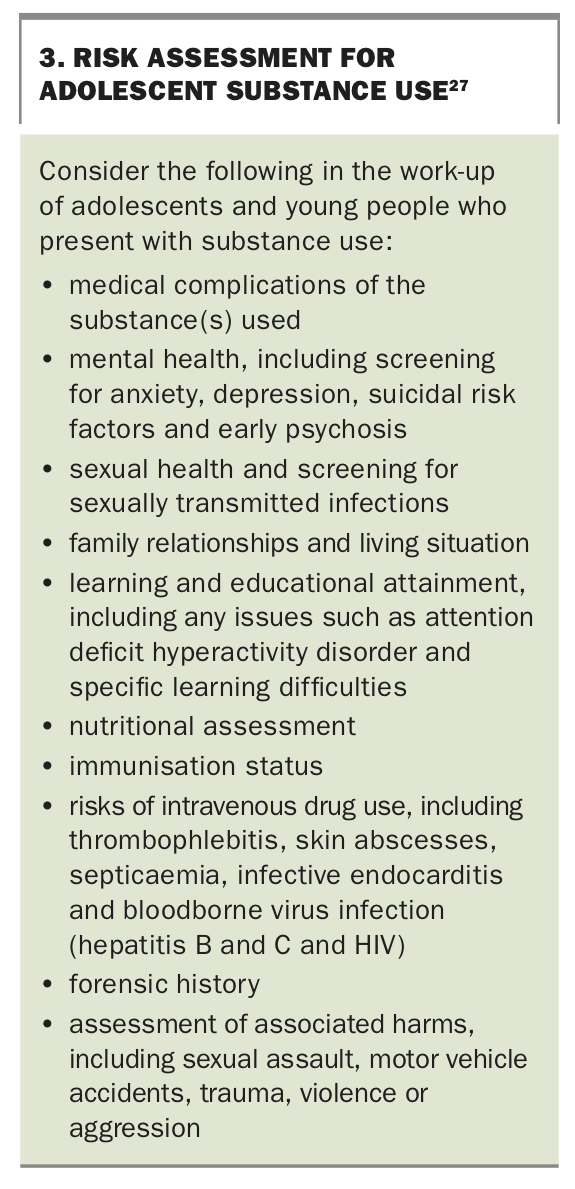
An evidence-based approach to the assessment and treatment of substance use in adolescents and young people was described in the September 2020 issue of Medicine Today.27 This work-up includes a risk assessment that should be performed for all adolescents and young people presenting with substance use (Box 3).27 Further research is needed to inform specific evidence-based interventions for adolescents who vape. Until this is available, GPs may apply the following principles of alcohol and other drug assessment and intervention to address vaping and its potential harms in young people.
{kind=link}
Assessment
Bridging questions are often helpful before taking a focused drug history. A good place to start is the HEEADSSS psychosocial interview for adolescents (covering home environment, education and employment, eating, peer-related activities, drugs, sexuality, suicide/depression and safety from injury and violence).28
Using clear, open and nonjudgemental communication, ask individually about each substance group and specifically about nicotine and marijuana use, as these are the most common substances inhaled. Ascertain age at first use and regular use, the type of vaping device used, and the pattern (e.g. daily, socially, on weekends) and frequency of use.
Quantify how much the individual vapes (e.g. How many puffs do you take at a time? How often throughout the day do you vape? When do you first start?), the strength of the e-cigarette (by concentration or category) and how frequently they cycle through their vapes (if they are disposable) or cartridges (if they are reusable). Young people often have limited insight into the volume of their use and may be surprised by the amount of nicotine consumed when compared with regular cigarette smoking.
Finally, ask the patient when they last vaped and whether they have experienced symptoms of withdrawal (e.g. nicotine or cannabis cravings), tolerance or any of the adverse effects described above.
It can be difficult to assess the safety and nicotine content of e-cigarettes and vaping liquids because of the wide variety of devices and labelling that is incomplete, ambiguous (‘low’, ‘medium’, ‘high’) or inaccurate.4 Supposedly nicotine-free e-cigarettes in Australia have been found to contain nicotine.29 Users may also replace the liquid in their devices or create their own liquid, most commonly containing marijuana. The efficiency of the vaporisation process influences how much of the drug is aerosolised, and the nicotine bioavailability affects how much is absorbed into the bloodstream.
A typical cigarette contains about 10 to 15mg of nicotine, with about 10% absorbed by the smoker.30 To assess the nicotine equivalency between any given vaping profile and cigarette smoking, it is necessary to measure the quantity of nicotine in the e-liquid and vapour and concentration of nicotine in the blood plasma after use. Recent studies have evaluated the nicotine equivalence of JUULpods, a brand of disposable nicotine-containing vaping device popular among youth in the USA. Estimates vary by study design and user behaviour; however, the common 5% JUULpod (40mg of nicotine per pod) is estimated to deliver nicotine equivalent to smoking 13 to 30 cigarettes.31
As a ‘rule of thumb’, one medium-strength vaping device (12 to 8mg/mL nicotine) with an estimated 200 ‘puffs’ is equivalent to smoking about 20 cigarettes. It is important to recognise that significant variation exists between individual vaping profiles.
Vaping is a voluntary and preventable behaviour. Gaining an understanding of why the young person vapes, and any accompanying beliefs, perceived benefits or misconceptions will help target appropriate interventions. Vaping use may be a response to stress and anxiety, peer influences, thrill-seeking behaviours, perceived harmlessness and, in some cases, nicotine addiction.
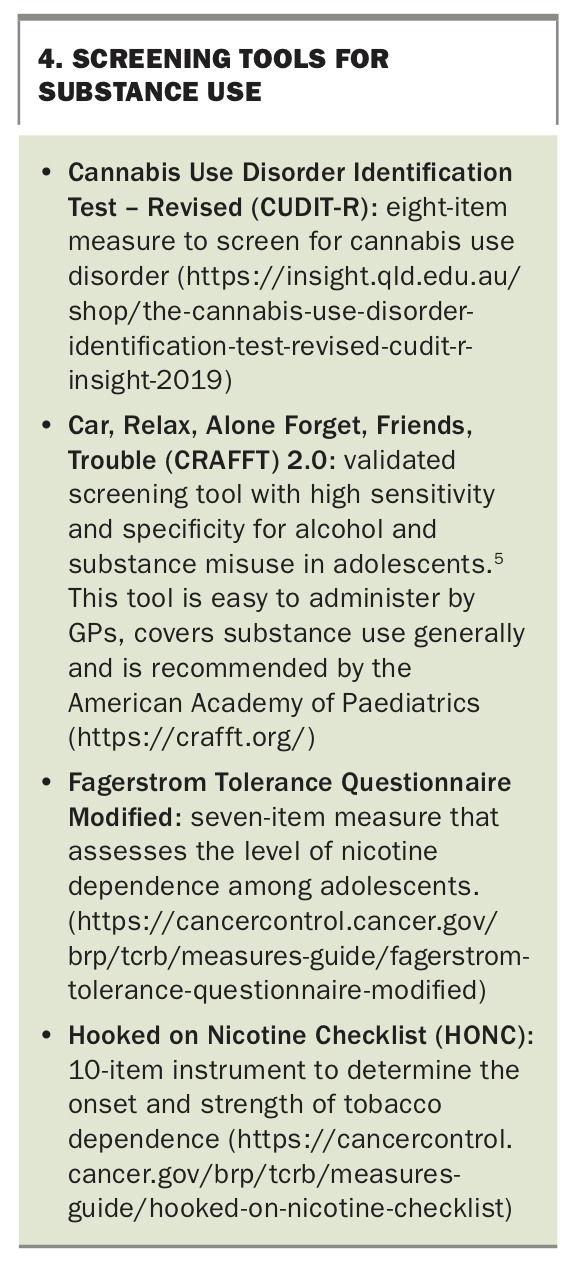
Several standardised screening tools are validated to identify harmful use of substances in young people. Those applicable to vaping are listed in Box 4. These tools are administered via interview or self-report (e.g. a questionnaire completed in the practice waiting room) and will help to distinguish between social, problematic and dependent patterns of nicotine and marijuana use.26
{kind=link}
Intervention
A detailed discussion of interventions in young people who vape is outside the scope of this review. However, effective approaches to intervention in young people should be strengths-based, aimed at increasing protective factors, reducing risk factors and building resilience.32 Primary intervention aims to prevent or delay the onset of vaping use through the use of brief interventions (e.g. the 5A’s approach to smoking cessation), motivational interviewing, psychoeducation (Box 2) and principles of harm minimisation (Box 5).33,34
{kind=link}
Secondary intervention seeks to address problems associated with current vaping use, preventing subsequent tobacco use and averting progression to possible nicotine or marijuana dependence.26 Engaging adolescents, employing brief interventions that promote self-management and referring to youth drug and alcohol, community mental health and paediatric services are often needed early in the drug use spectrum to prevent substance misuse and to achieve positive behaviour change (Box 5).
Conclusion
The rise of youth vaping in Australia despite restrictions on availability and supply is a significant public health concern. Not only does vaping carry significant health risks but evidence is growing that it is a gateway to conventional smoking. Key to addressing adolescent vaping use is for all care providers to recognise the harm, intervene early and work collaboratively across the health, education and political spectrum to maintain current safeguards and protect our future generations. MT