Preventing falls in older people with dementia

Dr Taylor is a Senior Postdoctoral Research Fellow at the Falls, Balance and Injury Research Centre, Neuroscience Research Australia, Sydney; and Conjoint Lecturer at UNSW Sydney, Sydney.
Professor Close is a Geriatrician at the Prince of Wales Hospital, Sydney; Clinical Director at the Falls, Balance and Injury Research Centre, Neuroscience Research Australia, Sydney; and Conjoint Professor at UNSW Sydney, Sydney, NSW.
Dementia

Falls are common among older people with dementia and often have serious consequences. A number of validated assessment tools are available to help identify fall risk factors. GPs have an important role in screening older patients for dementia and implementing evidence-based management strategies to help reduce falls.
- Older people with dementia experience more falls (>60% of those living in the community fall annually) and with more serious consequences than the general older population.
- GPs have a critical role in screening and assessing for dementia and fall risk in older patients, and a number of validated assessment tools are available.
- In community-dwelling older people with mild to moderate dementia, exercise that challenges balance may prevent falls.
- In residents of care facilities, the evidence is inconclusive regarding exercise, but vitamin D supplementation and increasing dietary calcium and protein intake may prevent falls and fractures.
- Some pharmacotherapies, such as centrally acting or psychotropic medications, increase fall risk and should be avoided in older people.
- Fracture risk can also be reduced by assessing bone health and treating osteoporosis.
Falls are common among older people with dementia, with more than 60% of people with dementia living in the community falling annually and more than 40% falling multiple times.1,2 In residential aged care, 50% of residents with dementia fell over a six-month period.3 Fall-related injuries, including hip fracture and head injury, are more common in older people with dementia, and this population is less likely to regain their previous level of function and more likely to be placed in residential care and die after a fall than older people without dementia.4 The cost of falls and fall-related injury is substantial in this population; to the individual, their family and the healthcare system. This article outlines how GPs can screen for cognitive impairment and assess and manage fall risk for this population.
Dementia vs cognitive impairment
A diagnosis of dementia, more recently termed major neurocognitive disorder, involves clinical assessment by a trained medical professional and requires an individual to have a cognitive impairment that affects their ability to function independently in daily life. When assessing a person in the context of diagnosing dementia, the clinician needs to exclude other possible causes of cognitive impairment such as depression and delirium, consider the individual’s previous level of cognitive function and, when possible, use information from an informant, such as a caregiver or family member who is in regular contact with the person.
Many studies on fall risk factors and fall prevention strategies targeting ‘people living with dementia’ were pragmatic in their recruitment approach and used inclusion criteria of ‘diagnosed dementia’ and cut-points on validated cognitive assessments. Some of these studies, therefore, refer to the study population as ‘cognitively impaired’, and this has resulted in the terms cognitive impairment and dementia being used interchangeably in the literature. For the purposes of this article, we will refer to the study populations as having dementia.
Identifying impaired cognition
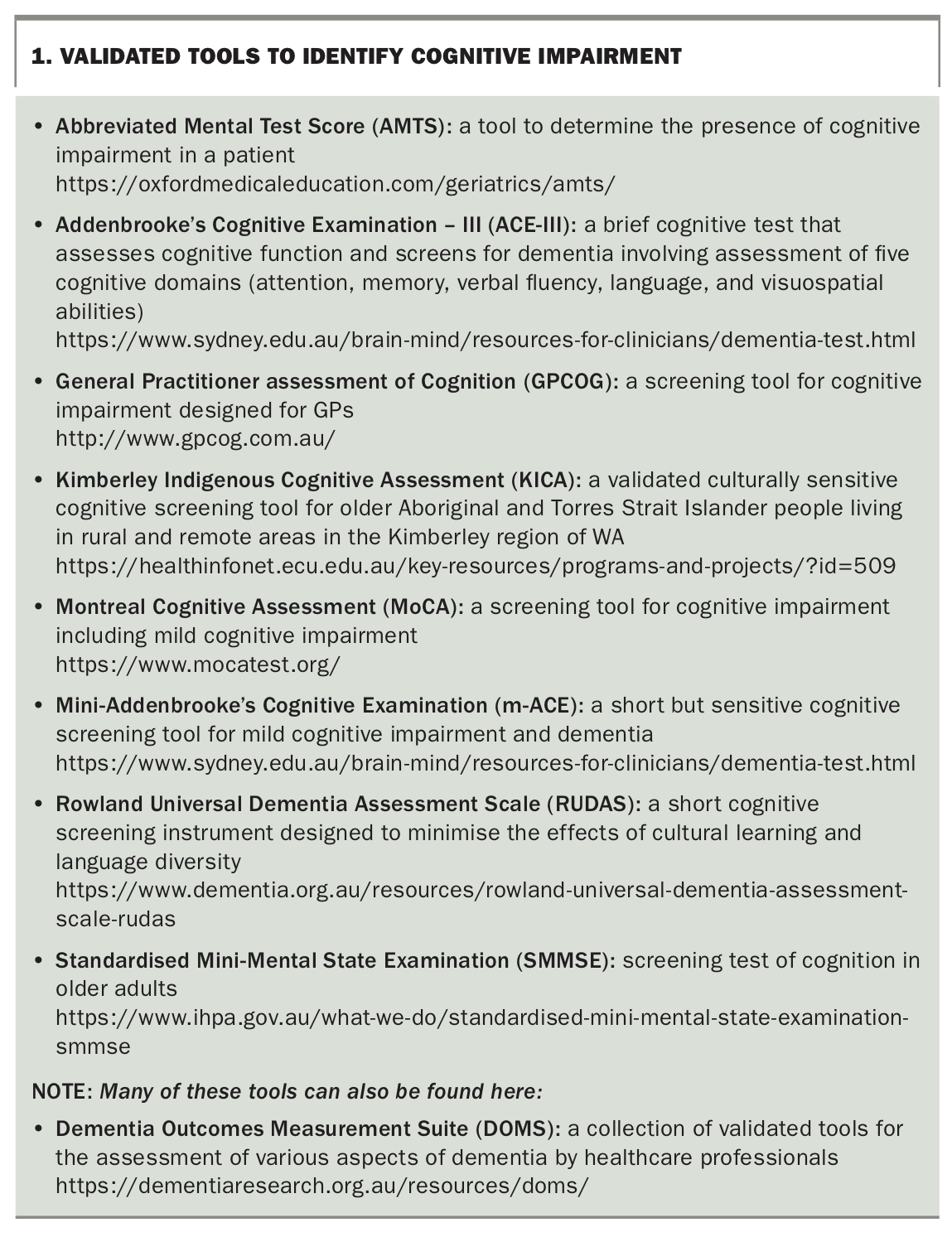
Cognitive impairment can be challenging to identify, particularly in the early stages of cognitive decline. A range of assessment tools are available to help clinicians objectively determine an individual’s level of cognition. Box 1 highlights assessment tools that can help GPs identify cognitive decline and monitor cognitive performance over time.
{kind=link}
Fall risk: screening and assessment
Falls are usually multifactorial and different individuals will present with different risk factors. Screening will help identify who is at risk, but not necessarily why. Screening for falls risk should be undertaken annually for all older people. In people with dementia who are in the moderate- to high-risk group for falls, identifying risk factors and implementing interventions to reduce risk becomes important and screening should be more frequent (i.e. six monthly).
There are many ways to screen people with dementia for fall risk. The simplest way is to ask whether they have had a fall in the past six to 12 months. People who have fallen in the past year are at least twice as likely to fall in the coming year.5-7 If a person has had two or more falls in the past 12 months, is presenting with a fall or is reporting walking or balance difficulties, they should undergo multifactorial assessment.8,9 This can be done in the GP practice, at a specialised clinic, at their residential aged care facility, at a physiotherapy clinic as part of a management plan, in their home (e.g. an occupational therapy home visit) or any combination of these to ensure that appropriate assessment and management plans are implemented.
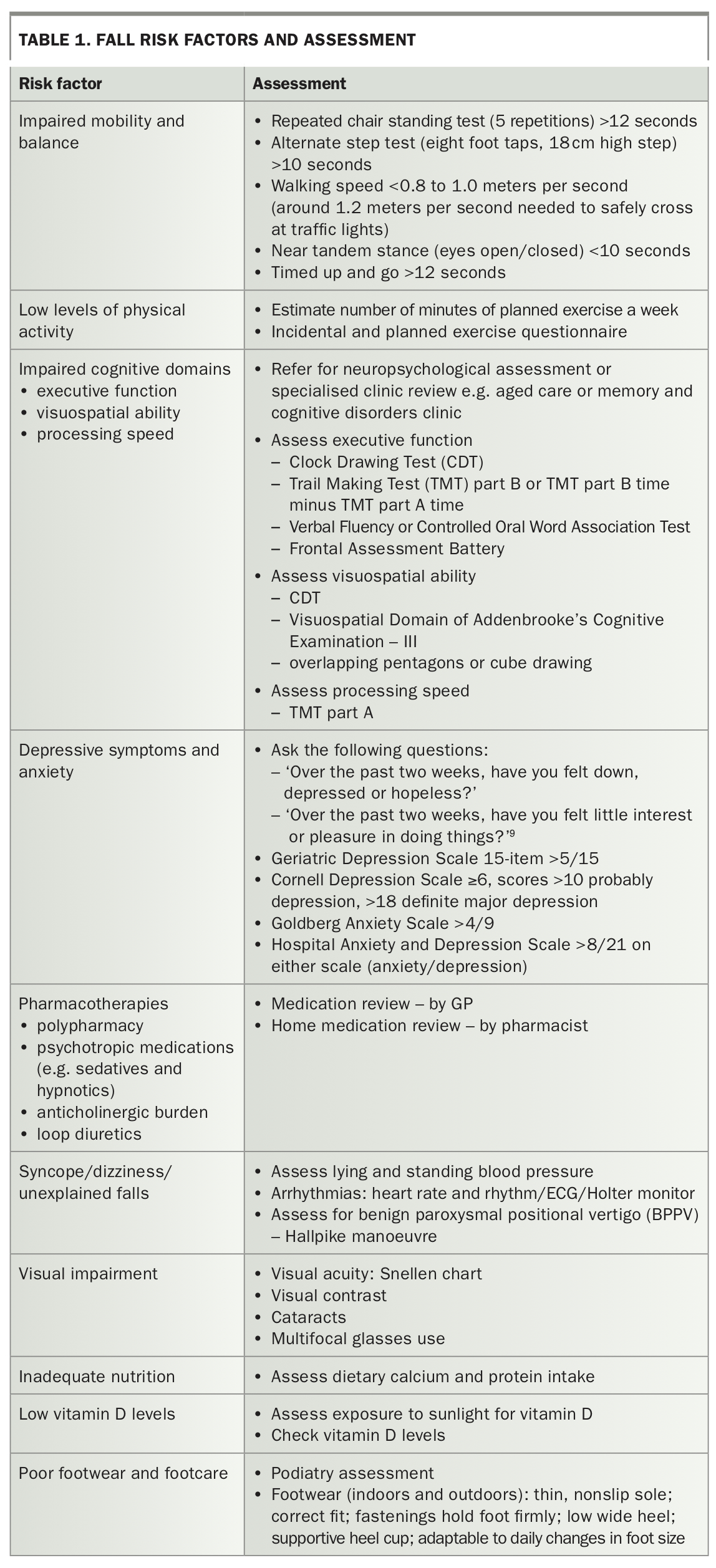
When an individual is identified as being at increased risk of falls, it is important to systematically identify risk factors and put in place appropriate intervention strategies. Table 1 highlights potential fall risk factors for people with dementia and potential approaches to assessment. In people with dementia, impaired balance and mobility, slow gait speed, depressive symptoms and physical inactivity increase fall risk.2,3,5 Impaired executive function, processing speed and visuospatial ability and higher levels of anxiety and concern about falls have also been identified as fall risk factors.5 Centrally acting or psychotropic medications (e.g. sedatives, hypnotics, antidepressants and antipsychotics), as well as polypharmacy (more than four medications), have been identified as fall risk factors in both community and residential care settings, and GPs play a crucial role in reviewing medications and rationalising their ongoing use.3,5,10,11
{kind=link}
A number of relatively simple assessments can be undertaken in the GP clinic or recommended by the GP. These include assessing vitamin D levels and bone health; vision (has the patient’s vision been assessed in the last 12 months, do they use bifocal or multifocal glasses, do they have cataracts?); blood pressure (including postural); and physical activity levels. Although these assessments are not specific people with dementia, they have either been conducted in populations that included older people with dementia or represent good clinical practice for assessing and managing fall risk.
Several fall risk assessment tools have been developed for use in people with dementia living in residential care. The fall-related impulsive behaviour scale (FIBS) is quick and easy to administer and involves three simple questions to residential care staff or a carer:
- Does the resident try to sit down before getting right up to the chair/toilet/bed?
- Does the resident attempt to stand before wheelchair brakes have been applied or footplates moved or walking frame placed in front of them?
- Does the resident try to walk without help when asked not to?
Each question is scored on a Likert scale (0 = never or not applicable, 1 = occasionally, 2 = often, 3 = frequently, 4 = very frequently) and the score is the sum of the four questions. Residents who scored 1 or more were almost three times more likely to fall over the subsequent six-month period.12
An alternative four-item assessment can be used to assess fall risk in older people with dementia living in residential care facilities. The assessment is more involved and time consuming and involves assessing four risk factors:
- balance, measured by postural sway (defined cut-point for fall risk: sway >4500 mm with eyes closed)
- attention and orientation using the Addenbrooke’s Cognitive Examination (defined cut-point for fall risk: score <9)
- anxiety using the Goldberg Anxiety Scale (defined cut-point for fall risk: score >4)
- antidepressant use.3
Risk of falls increased with each additional risk factor; all residents with four risk factors fell during six months of follow up.3
Interventions
Much of the evidence for intervention in falls prevention is derived from studies involving people who do not have dementia; therefore, caution is needed when extrapolating to a population with dementia. Fortunately, an increasing body of evidence is focused specifically on interventions in people with dementia.
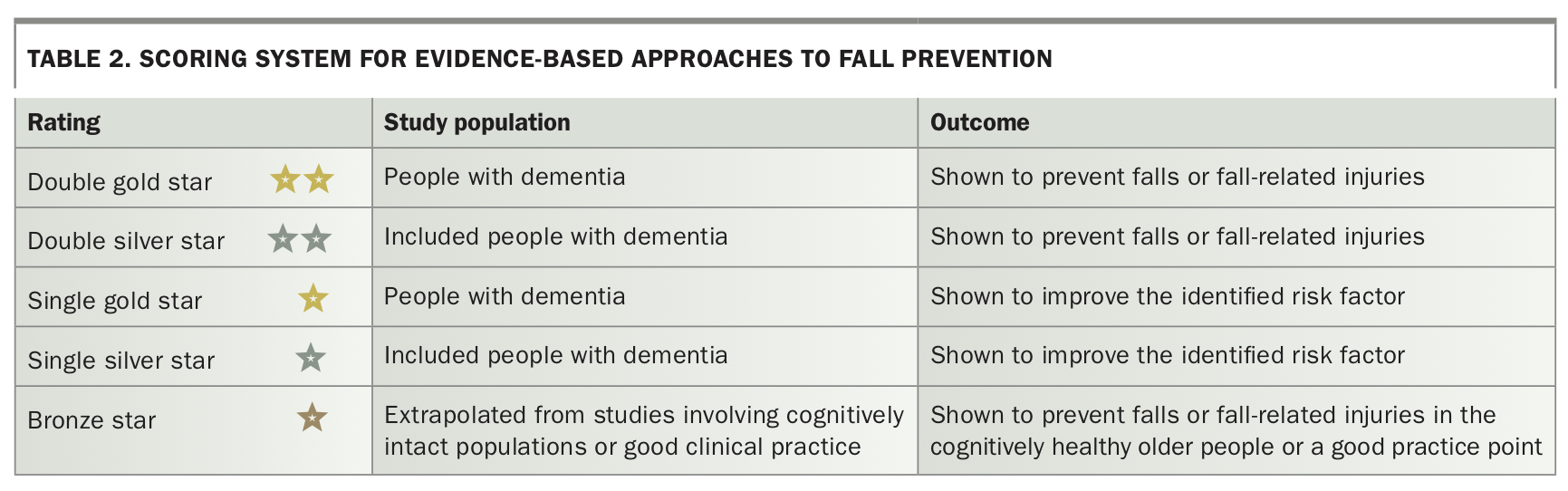
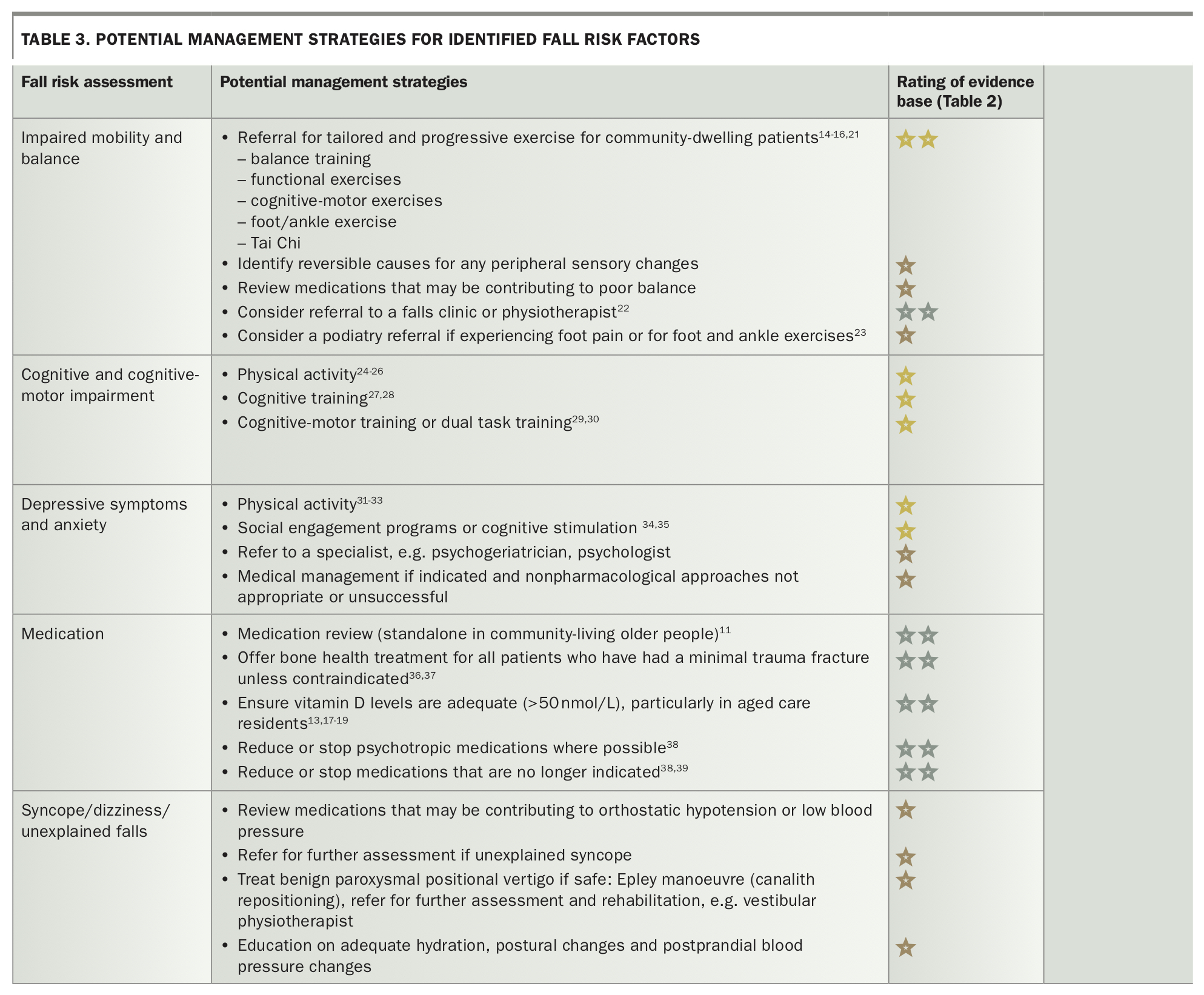
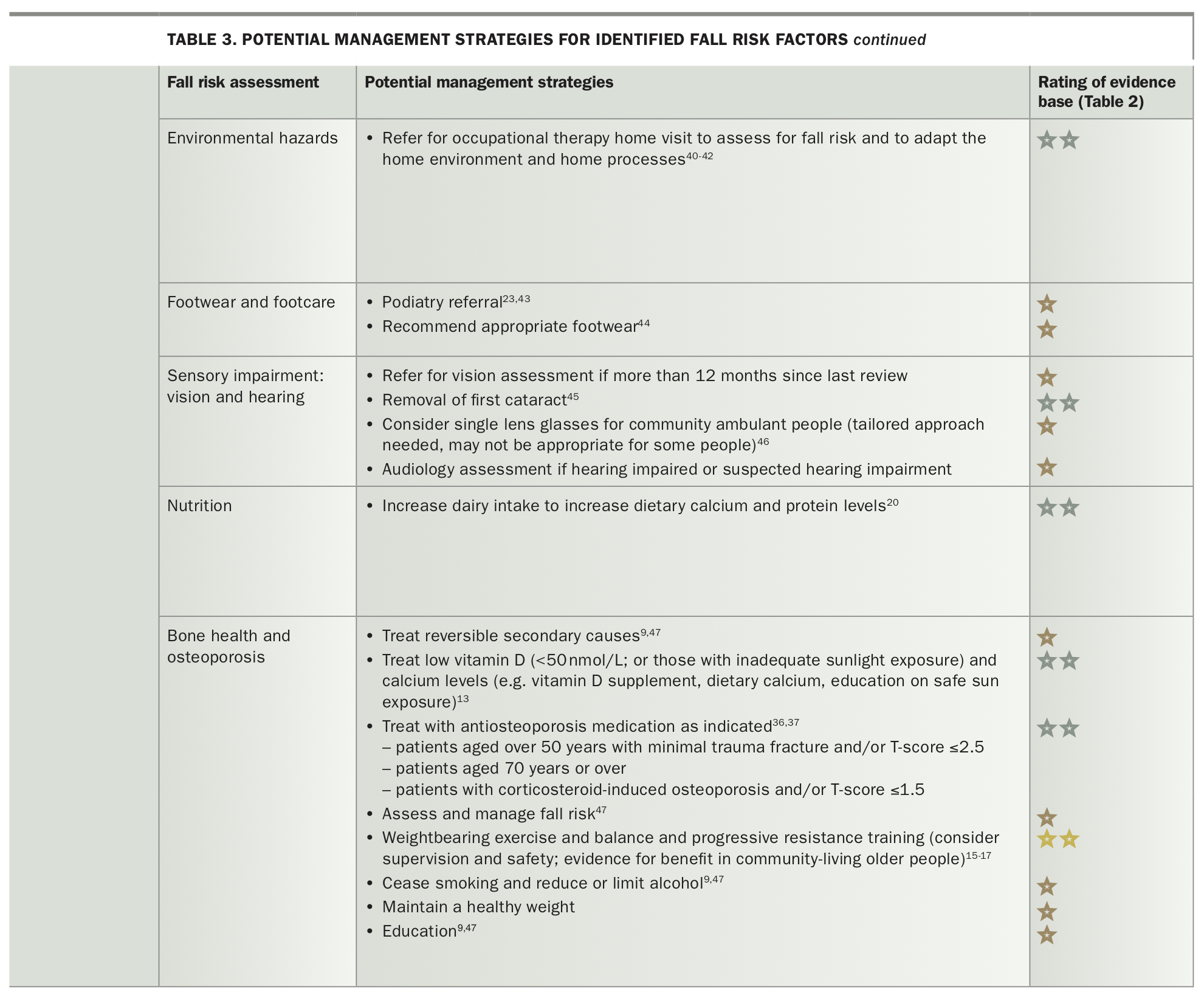
Here we provide an overview of potential approaches to intervention for fall prevention and attempt to rate the level of evidence based on how it was generated (Table 2) to guide the clinician to areas where there is more certainty around likely beneficial interventions for the intended population (Table 3 Pt One and Pt Two). 9,11,13-47 In Table 3, fall prevention strategies have been assigned a rating (gold, silver, bronze stars) according the population studied and its level of evidence. A description of the rating system is provided below and in Table 2.
{kind=link}
{kind=link}
{kind=link}
- Double gold stars represent studies where evidence has been generated specifically in people with dementia and the intervention has been shown to prevent falls or fall-related injuries such as fractures.
- Double silver stars represent interventions where the original studies included some people with dementia and the intervention has been shown to prevent falls or fall-related injuries.
- A single gold star represents studies where evidence has been generated specifically in people who have dementia and the intervention has been shown to improve the identified risk factor (as opposed to falls or fall-related injury as an outcome).
- A single silver star represents interventions where the original studies included some people with dementia and the intervention has been shown to improve the identified risk factor.
- A bronze star represents fall prevention evidence that has largely been extrapolated from studies involving cognitively intact populations or is considered a good practice point.
Fall prevention by setting
The evidence for fall prevention broadly, and specifically in people with dementia, is setting specific, i.e. community, residential care.13,48 People living in residential care tend to have greater levels of impairment (cognitive and physical) and the level of support available and environment in which the interventions are being delivered are inherently different from the community setting. These differences support setting-specific approaches to fall prevention interventions and perhaps explain why, so far, interventions, their delivery and effectiveness differ by setting.13,48
Preventing falls in the community
Exercise probably prevents falls in people with mild to moderate dementia living in the community, but the reduction in fall rate is shown by just a few studies (Table 3 Pt One and Pt Two).14 The exercise programs have usually been prescribed by a trained professional with experience in working with people with dementia, are at least six months in duration and provide some level of supervision by a trained professional. Evidence suggests that exercise-based interventions may be more beneficial for fall prevention in people with mild to moderate dementia who have better physical function.15,16
{kind=link}
Preventing falls and fall-related injury in residential care
A recent Cochrane review showed that overall, the evidence to support fall prevention interventions in people with dementia in residential aged care is inconclusive, or is neither harmful nor effective for most intervention strategies, e.g. exercise and multifactorial interventions.13 In people with dementia who are vitamin D deficient, vitamin D supplementation may reduce the rate of falls (Table 3 Pt One and Pt Two).13 Although these recommendations are not specific to people with dementia, the studies contributing to this recommendation include people with dementia.17-19 There is no reason to believe that this intervention would be any less effective in people with dementia.
One recent Australian study showed that increasing dietary calcium and protein intake by eating more dairy products (milk, yoghurt and cheese) prevented falls and fractures (including hip fractures) in people living in care facilities.20 People with dementia were included in this study (in a subgroup with data reported for this variable, around 50% had dementia) and osteoporosis-related medication use was similar between the intervention and control groups. Subgroup analysis of another Australian study, published since the Cochrane review, showed exercise reduced falls and fall-related injury in people with mild to moderate dementia living in care facilities.49
Bone health
Osteoporosis is associated with increased fracture risk; therefore, bone health is an important factor that should not be overlooked in this population. Interventions to improve bone health may benefit patients through improved fracture prevention. Although bone health medications have been shown to reduce fracture risk, older people with dementia are undertreated.50,51 Medications used to improve bone health are summarised in Box 2. People should be replete in calcium and vitamin D before initiating the antiosteoporosis medications. There is no requirement for dual-energy x-ray absorptiometry in older people who have sustained a low trauma fracture (fall from standing height or less) before prescribing these medications. Appropriate treatment selection to improve bone health requires careful patient assessment. Important considerations before starting treatment include: 47
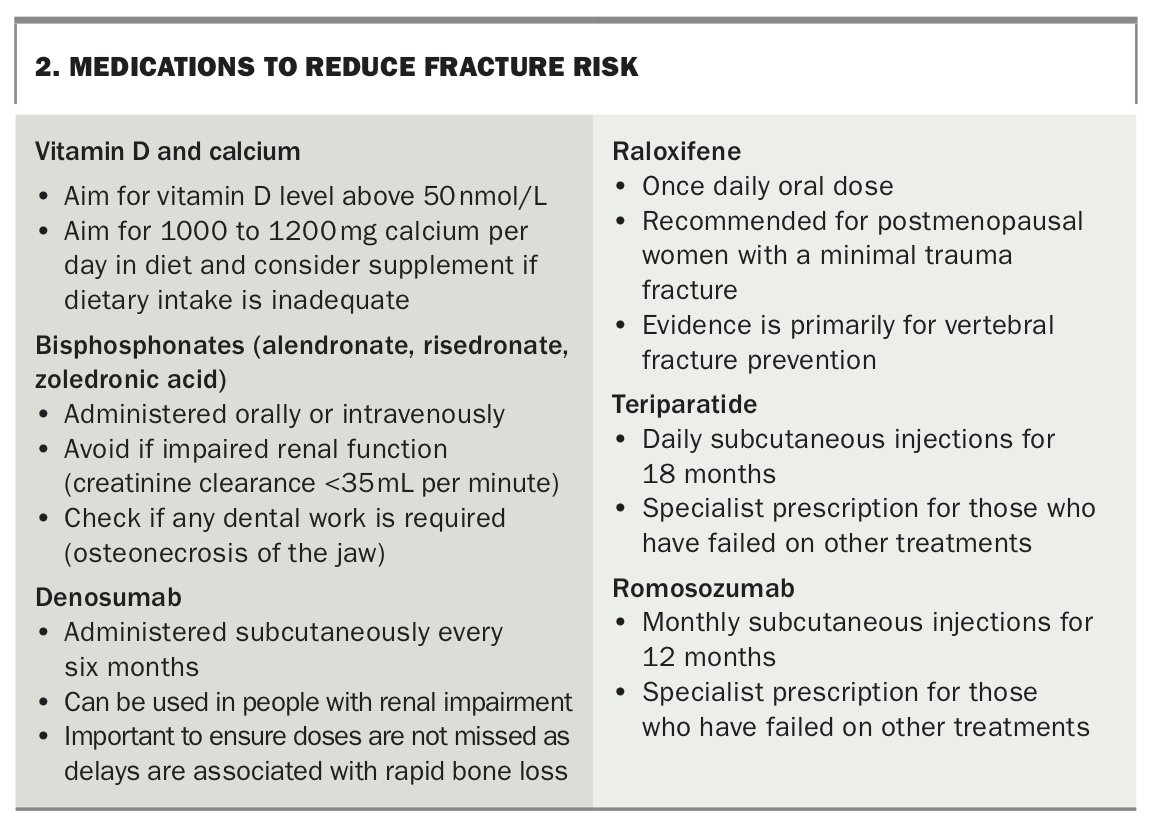{kind=link}
- the patient’s preferences
- whether the patient is likely to adhere to the medication regimen
- ensuring any secondary causes of osteoporosis have been addressed
- ensuring appropriate vitamin D and calcium levels
- addressing oral health care needs
- assessing whether the patient’s renal function is sufficient for the treatment selected.
Specialist referral for prevention and management of falls
Specialist clinics may be able to support the GP in their assessment and management of fall risk in people with dementia. Geriatricians may also be able to support GPs in this area. However, specialist clinics and specialists may not be available in all areas of Australia, such as some regional and remote areas. Therefore, GPs are pivotal in assessing and managing fall risk in older patients.
GPs may also refer community-dwelling older people with dementia to allied health professionals such as physiotherapists, exercise physiologists, podiatrists, pharmacists and occupational therapists to assist with assessing and managing fall risk (Table 3 Pt One and Pt Two). For community-dwelling older people with dementia, these services can be accessed privately or through community-based hospital or outreach services. For those in residential aged care, access to these services may be facility dependent, although family members may be able to organise some services privately.
Conclusion
Older people with dementia are at high risk of falls and often suffer more severe consequences and have poorer outcomes as a result. GPs have an important role in screening and managing fall risk in older patients, particularly in regional and remote areas. Screening, assessing and managing fall and fracture risk has the potential to improve the lives and outcomes for many patients with dementia. The research supporting prevention strategies in this group is slowly growing, with more evidence needed to help appropriately direct prevention efforts. MT
Further reading
Lord SR, Sherrington C, Naganathan, V eds. Falls in older people. In: Risk factors, strategies for prevention and implications for practice. 3rd ed. Cambridge: Cambridge University Press; 2021.
Guideline Adaptation Committee. Clinical practice guidelines and principles of care for people withdementia. Sydney: Guideline Adaptation Committee; 2016. Available online at: https://cdpc.sydney.edu.au/wp-content/uploads/2019/06/Dementia-Guideline-Recommendations-WEB-version.pdf (accessed March 2022).
Montero-Odasso M, Camicioli R eds. Falls and cognition in older persons: fundamentals, assessment and therapeutic options. Switzerland: Springer International Publishing; 2020.
Poulos CJ, Gresham M, Poulos RG, Maurice C, O’Connor CM. Supporting independence and function in people living with dementia. A handbook of reablement programs for service providers and others with an interest in improving function. 2nd ed. Sydney: HammondCare; 2019. Available online at: https://www.hammond.com.au/documents/reablement-guides/479-hc-handbook-2019-2nd-edition/file (accessed March 2022).