A tragic loss: pregabalin prescribing risks

Ms Tuohey is Practice Manager Legal (Professional Conduct) Victoria, Avant Mutual, Melbourne.
Dr Nickels is Practice Manager Claims (Professional Conduct) Victoria; and Senior Medical Advisor, Avant Mutual, Melbourne, Vic.
Pain
Medicolegal medicine

This series highlights common medicolegal issues in general practice. Written by a team from medical defence organisation Avant, the series is based on actual cases, with details changed for privacy and some issues summarised for the sake of discussion. This scenario highlights an emerging trend of pregabalin misuse identified by coronial investigations into deaths involving mixed drug toxicity.
Since the analgesic and anticonvulsant pregabalin was listed on the PBS for the treatment of neuropathic pain in 2013, its use in Australia has increased dramatically. However, there is growing disquiet worldwide about the risk of pregabalin harms and misuse. Australian coroners, particularly in Victoria, have raised concerns about an increase in cases in which pregabalin is implicated in deaths due to multiple drug toxicity.
The following case scenario of a patient taking prescription pregabalin who died of mixed-drug toxicity illustrates some of the medicolegal issues for medical practitioners prescribing pregabalin. It also demonstrates the importance of real-time prescription monitoring systems for prescribers.
Case scenario
Dr Green, a GP in Melbourne, was contacted by the police after his patient Adam, aged 29 years, was found deceased at his home. Emergency services had been called, but Adam could not be revived. Multiple prescriptions were found in Adam’s name, prescribed by multiple doctors. An autopsy identified mixed-drug toxicity involving oxycodone, pregabalin and amitriptyline. Dr Green was required to give evidence at a coronial inquest.
Adam first presented to Dr Green at the age of 27 years with a history of a traumatic knee injury and chronic back pain from a motor vehicle accident five years earlier. At the time, he was being prescribed oxycodone. Over the years, he underwent multiple surgical procedures on the knee.
Adam reported to Dr Green that his pain levels were not being managed and, despite Dr Green’s efforts to reduce his oxycodone dose, this was not achieved. Dr Green began prescribing pregabalin, which he considered preferable to opioids. Specifically, he believed it could be taken on a long-term basis safely and without the risk profile and potential for misuse associated with opioids.
Unbeknown to Dr Green, Adam was receiving pregabalin from five other doctors. In the three months before his death, he was prescribed multiple drugs that act as central nervous system depressants: oxycodone, pregabalin and amitriptyline.
The Coroner determined that the cause of death was mixed-drug toxicity caused by these drugs.
Medicolegal issues
Discovering that a patient in your care has been harmed is difficult for any medical practitioner. Particularly so, as in this case, when the risks of a particular medication are starting to be better understood. In such cases, the medical practitioner’s care will be considered in light of the standards at the time the care was provided. As understanding of medication risks evolves, it is important for doctors to keep up to date with medication and prescribing guidelines, as well as to ensure they follow the fundamentals of good practice in prescribing, patient communication and record-keeping.
Discussion
Prescribing standards
Medical practitioners need to satisfy themselves that their prescribing complies with their obligations under the Medical Board of Australia’s Code of Conduct for Doctors in Australia to provide good patient care.1 This includes making sure that any medication prescribed is safe, appropriate, and prescribed in accordance with an accepted therapeutic standard.
Concerns about pregabalin prescribing
With growing apprehension about the risks associated with opioid use, it is increasingly common for medical practitioners to seek alternatives to assist patients manage chronic noncancer pain. According to recent data provided by the PBS, pregabalin ranked as the seventh most subsidised drug in Australia in 2020-21.2
Medical practitioners may consider pregabalin to have a lower risk profile than opioids for managing neuropathic pain. However, there are reports of misuse. Tolerance and withdrawal symptoms have been reported.3 There have also been reports of euphoria as a side effect and of users taking large doses of pregabalin for euphoric and dissociative effects.3,4 Recreational use is reportedly increasing.5
Coroners, particularly in Victoria, have been raising concerns about the increasing implication of pregabalin in deaths due to multiple drug toxicity.4,6,7 In 2019, pregabalin was the sixth highest contributing drug in overdose deaths in Victoria, behind diazepam, heroin, methamphetamine, methadone and alcohol.4,8
In February 2021, the TGA announced that boxed warnings were being added to medications containing pregabalin and gabapentin. The warnings advise that pregabalin poses risks of misuse and dependence. The risks increase when pregabalin is prescribed in conjunction with sedating medications including opioids.9 In 2021, a practice review warning was issued to GPs across Australia about the potential harmful and hazardous use of pregabalin.10
A way to reduce the risk of overdose is to consider completing a risk assessment for misuse. Precautions used when prescribing other pharmaceuticals should also be considered when prescribing pregabalin, especially in patients with a substance use history. In light of potential harms, there should be a strong evidence-based indication before pregabalin is prescribed. Medical practitioners should watch for signs of misuse and dependence, such as presenting earlier than expected for supply.
When prescribing for patients with chronic noncancer pain, it is always important for medical practitioners to:
- establish and follow a pain management plan
- regularly review the plan and update it to reflect changing circumstances
- educate patients and engage them in a treating partnership
- adhere to professional guidelines
- maintain comprehensive medical records and document patient discussions
- seek specialist pain or addiction management input when concerned.11
Real-time prescription monitoring
In the above case of Adam, the Coroner concluded that the ‘ease with which he was able to obtain pregabalin from six different clinicians and in amounts in excess of therapeutic need, undoubtedly contributed to the continuing misuse, which ultimately played a part in his death’.
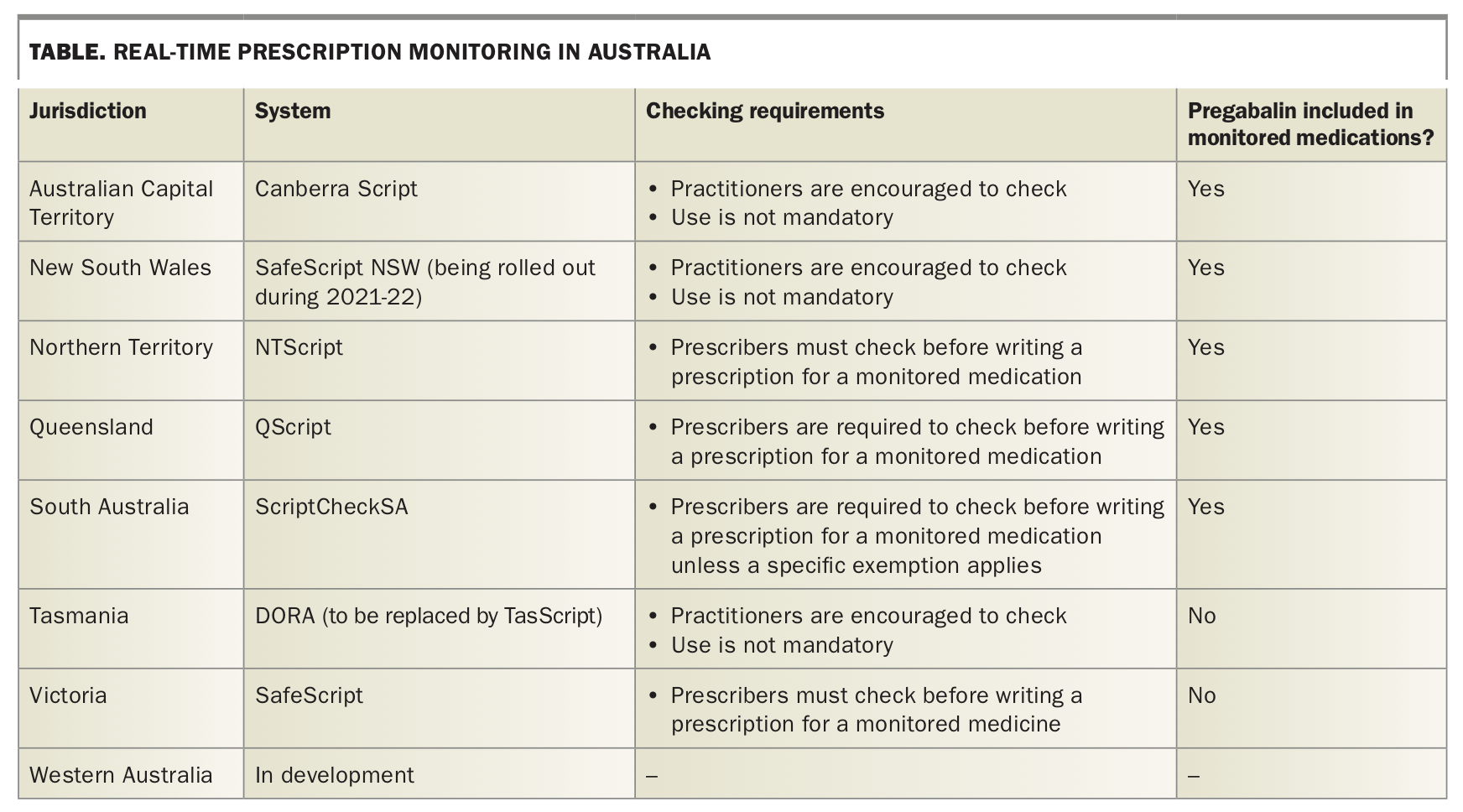
To help doctors manage prescribing of scheduled medications, the states and territories are beginning to implement real-time prescription monitoring of certain ‘monitored medications’. However, coroners continue to express concern at the speed of rollout and lack of a national system.
The systems in place for real-time prescription monitoring in different parts of Australia are shown in the Table. Victoria currently has a real-time prescription monitoring system. Since April 2020, it has been compulsory for prescribers in Victoria to check the SafeScript database before writing a prescription for a medication monitored through the system.12
{kind=link}
The medications monitored vary between the states and territories. Pregabalin is included in the list of monitored medications in many jurisdictions (Table). At the time of writing, it had not yet been added to Victoria’s SafeScript, despite repeated calls from coroners in Victoria.4,6,7 After reviewing recommendations in 2019, the Department of Health and Human Services Victoria (DHHS) decided not to add pregabalin. DHHS has not yet responded to the most recent recommendations.13
Although not all medications are currently monitored, real-time monitoring systems are important tools, particularly for detecting polypharmacy. The long-running Prescription Shopping Program can also help doctors who suspect their patient may be obtaining more prescriptions than clinically warranted, and may identify concerns relating to medications that are not monitored by real-time prescribing services. However, this applies only to medications obtained on the PBS and from multiple prescribers or at extremely high levels.
Medical practitioners still need to exercise care and clinical judgement in prescribing. If checking these monitoring systems raises alerts about a patient’s prescribing history, it does not prevent doctors prescribing. Real-time monitoring is a clinical tool that provides information about high-risk circumstances and helps doctors make more informed and safe clinical decisions. The notifications are not intended to dissuade or prevent prescribers from prescribing medicines they believe are clinically necessary.
Informing and educating patients
In the case of Adam, as in several recent coronial cases involving pregabalin, the Coroner concluded that the deceased had not intended to take his own life. As we discuss in more detail below, the Coroner considered that Dr Green’s prescribing practices were suboptimal and contributed to Adam’s death.
Although some recent studies have flagged concerns about intentional misuse of pregabalin, coroners and pain specialists have suggested that patients may be unaware of the risks posed by the medication. Patients may have exceeded the prescribed dose when their pain did not immediately respond, or may have combined it with other medications.14
As the New South Wales Coroner noted in another recent case in that state, ‘Unfortunately [the deceased] found it easy to obtain a range of drugs without, it seems, much education about the real dangers that mixing them could bring’.15 The deceased’s partner told the inquest he ‘never thought a person can die by the medicine prescribed by [a] doctor’.
These cases serve as a reminder that doctors always need to discuss treatment options with patients, including potential harm and material risks, and endeavour to confirm patients understand the information they have been given.1
Medical records
When a death is investigated by the coroner, or prescribing is investigated by the Medical Board of Australia, a common cause for concern is the level of detail in a prescriber’s clinical records. When conducting a retrospective investigation into a fatal outcome involving mixed-drug toxicity, it is unhelpful to see multiple repeat entries such as ‘prescription printed: pregabalin 300 mg capsule one before bed’.
Avant’s analysis of recent claims where medical records were a factor showed that records were found to be below standard in 11%, or one out of every nine claims.16 However, it was rare for documentation issues to be the primary basis of the claim (less than 1% of matters).
Poor record-keeping was much more commonly identified in claims where the doctor’s care was considered below standard on the main issue of the claim, such as diagnostic or medication error. However, inadequate record-keeping did affect claims outcomes. Some claims could not be defended because of incomplete or missing records. Complaints to regulators resulted in more severe outcomes when records were found to be poor.
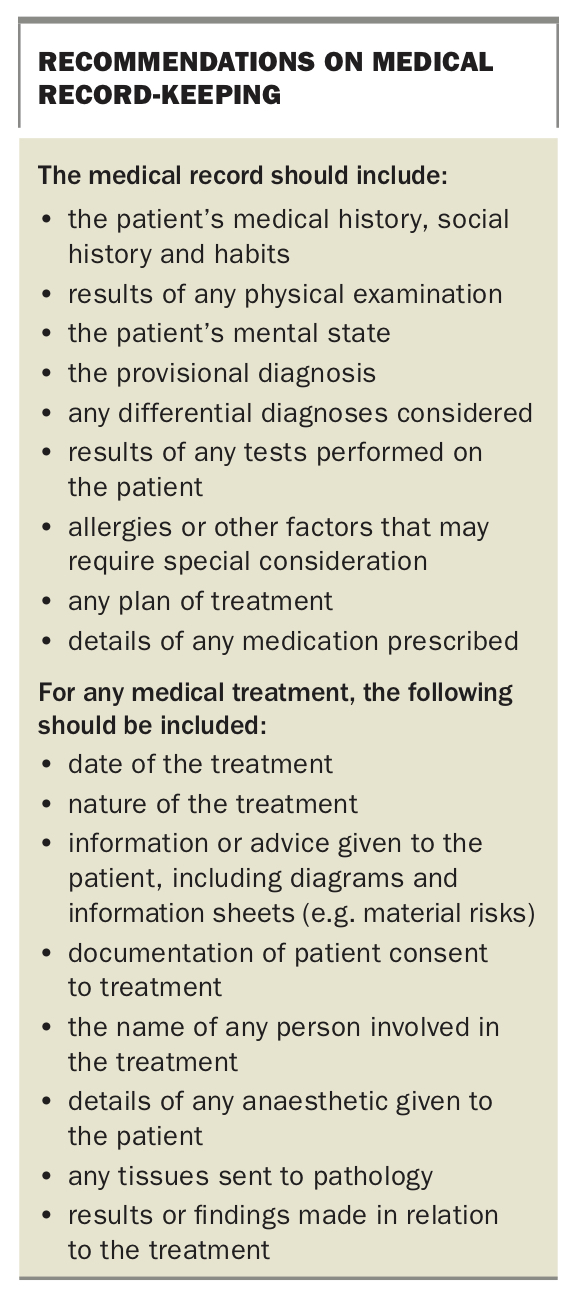
The requirements for medical record-keeping are set out in the Medical Board Code of Conduct and standards such as the Royal Australian College of General Practitioners’ Standards for General Practices (5th edition).17 In New South Wales, record-keeping requirements are also prescribed by legislation.18 Patient medical records need to identify the patient and include any information relevant to the diagnosis or treatment of the patient, details of the treatment provided, and any information or advice given to the patient (Box). When, as in the case of Adam, treatment involves helping patients manage complex issues, it is particularly important to document the rationale behind treatment decisions.
{kind=link}
In this case, the Coroner was critical of Dr Green’s record-keeping as well as his prescribing. Often the records contained a simple description of the presenting complaint and the prescriptions printed. There was no record of a review of Adam’s medications, the clinical indication for prescribing pregabalin, and any issues discussed or warnings provided. The Coroner considered Dr Green had failed to comply with professional record-keeping standards.
By contrast, in another recent decision also involving mixed-drug toxicity, the Coroner noted that the records clearly showed the doctors’ ‘considerable effort to manage [the patient’s] chronic pain and medication regime and to prevent medication escalation’.6
Conclusion
Coroners in all states and territories have recognised the complexities doctors face in treating patients with chronic noncancer pain and complex comorbidities. Over the years, they have repeatedly called for tools such as real-time prescription monitoring, to help doctors and patients manage drug dependence and diversion issues. As the Victorian Coroner noted, overall drug overdose deaths decreased in 2019 for the first time in a decade.4,19 Real-time monitoring tools, such as SafeScript in Victoria, are slowly becoming available and are helping doctors to be aware of patients who may be at risk of misusing medications.
Nevertheless, although real-time prescription monitoring is an important and valuable tool, it is not infallible. Doctors need to continue to take reasonable steps to satisfy themselves that it is safe and appropriate to prescribe all medications, and to explain the risks to patients. It is always important to document the discussion with the patient and the justification for ongoing prescribing. MT