Chronic pain – complexities in adolescents and young adults

Dr Alcock is a Specialist Anaesthetist and Pain Medicine Physician; and Clinical Lead of the Queensland Interdisciplinary Paediatric Persistent Pain Service, Children’s Health Queensland, Brisbane.
Ms Westerman is a Senior Occupational Therapist with the Queensland Interdisciplinary Paediatric Persistent Pain Service, Children’s Health Queensland, Brisbane, Qld.
Pain
Adolescent health

Adolescents and young adults experience chronic pain at similar rates to adults. Chronic pain in this group is associated with a high prevalence of adverse childhood experiences, mental health difficulties and neurodiversity. Recovery from persistent pain is the aim of developmentally sensitive therapy. Therapy includes validating the young person’s pain experience and needs-based interventions that focus on the mind–body connection and security in interpersonal relationships.
- Adolescents and young adults experience chronic pain at similar rates to adults.
- The medical assessment of a young person with chronic pain is an integral part of the biopsychosocial assessment, which searches for noxious contributors to the pain.
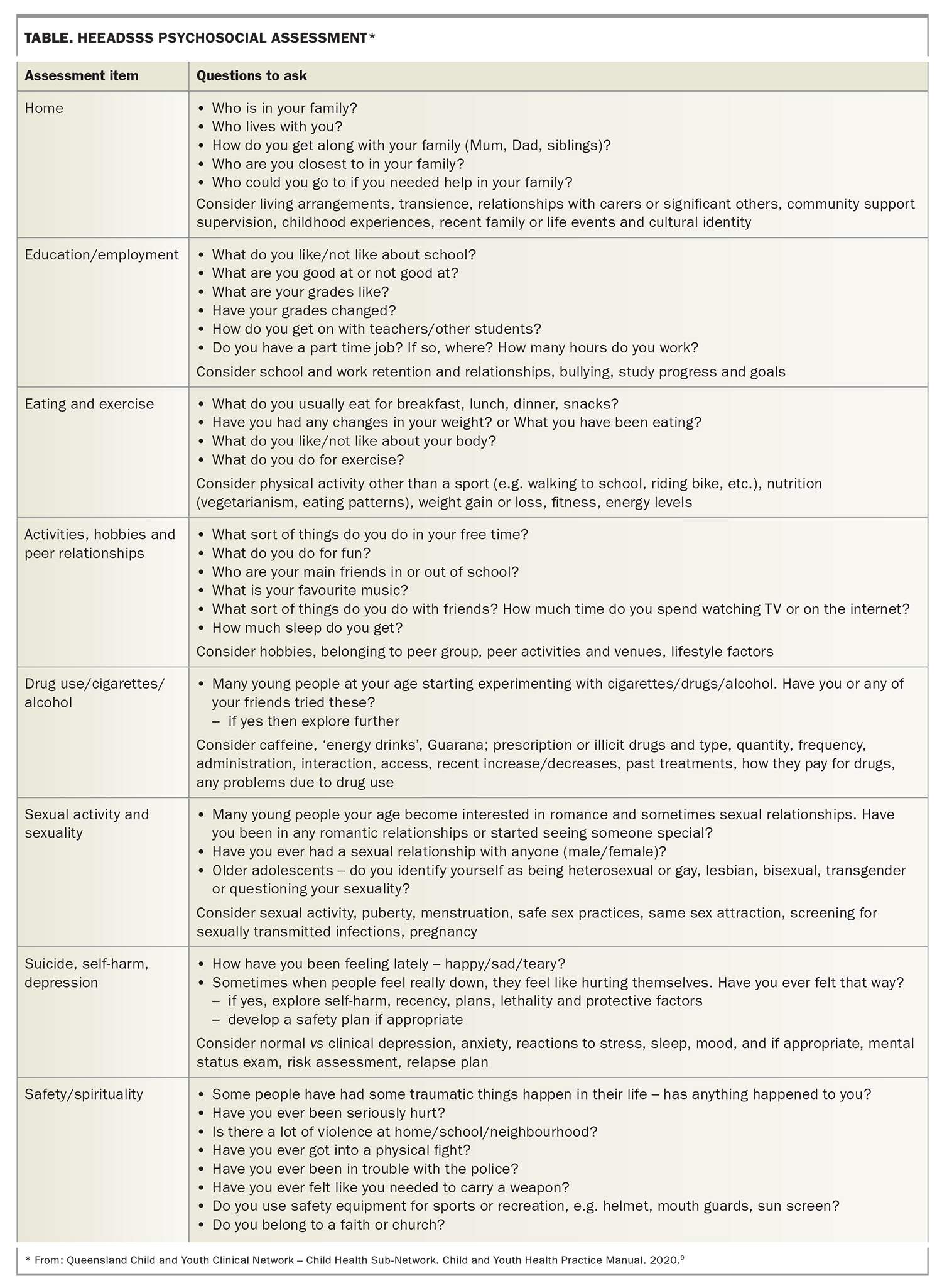
- The psychosocial components of the biopsychosocial assessment can be guided by the HEEADSSS (home, education/employment, eating and exercise, activities, drug use, sexual activity and sexuality, suicide and self-harm, safety/spirituality) assessment.
- Even in the absence of noxious contributors, chronic pain can be explained; our understanding of the neurophysiology underpinning chronic pain is rapidly evolving and translatable into clinical practice.
- Consistent messaging to young people with chronic pain that their body is safe, their pain is real and that recovery is possible is a key part of therapy.
- Developmentally sensitive therapy takes a needs-based approach that focuses on the mind–body connection and security in interpersonal relationships.
Chronic pain is defined as pain that persists or recurs for more than three months.1 If a noxious inciting event has occurred, chronic pain typically persists beyond the expected period of tissue healing. Chronic pain is common in adolescents and young adults, with estimated community prevalence rates ranging from 11 to 38%.2,3 Most young people access support for their chronic pain outside of pain clinics, including in primary, tertiary and community healthcare settings. Chronic pain is best managed with a biopsychosocial approach.
Adolescence and young adulthood
An adolescent is defined as a person aged between 10 and 19 years inclusive, whereas ‘young adult’ refers to a person aged from 20 to 24 years.4,5 The composite term ‘young people’ refers to the entire 10 to 24-year-old age range.
The adolescent and young adult years are a period of great change neurodevelopmentally. This change is heavily influenced by the environment a young person is living in and their interpersonal relationships. During these years, young people are increasingly aware of their identity and values, and have an ability to direct and shape their own health and wellbeing. This period of adaptive potential allows for trajectories to be transformed and for the impact of early childhood risk factors to be ameliorated, which may help reduce the burden of non-communicable disease later in adult life.6
Adolescence and young adults with pain
The prevalence of chronic pain is higher in girls and young women and increases with the onset of adolescence. Chronic pain can be a primary or secondary condition.1 It is a whole-of-life issue, often associated with functional difficulties, including reduced participation in school, study or employment; sleep disturbance; nutritional issues; changes in movement and occupational engagement; and tensions in interpersonal relationships. Compared with the general population, young people with chronic pain experience a higher prevalence of adverse childhood experiences, mental health difficulties and neurodiversity.
Medical assessment of a young person with chronic pain
When a young person presents with chronic pain, the initial priority is to assess with history, examination and judicious investigations for noxious contributors. When noxious contributors are not identified, this valuable information tells us the young person’s body is physically safe and helps to confidently switch from a biomedical to a biopsychosocial approach. Some young people with chronic pain live with chronic medical conditions such as juvenile idiopathic arthritis, cerebral palsy or a past history of cancer. Many live with psychological conditions such as anxiety, depression or post-traumatic stress disorder. Using information from medical assessment to support the young person, their caregiver and other clinicians to understand the interplay between these issues is key. Although a young person may be living with a condition where pain is an accepted symptom, pain that is persistent and interfering with development, function and participation needs assessment and support.
Chronic pain can be explained, even in the absence of noxious contributors
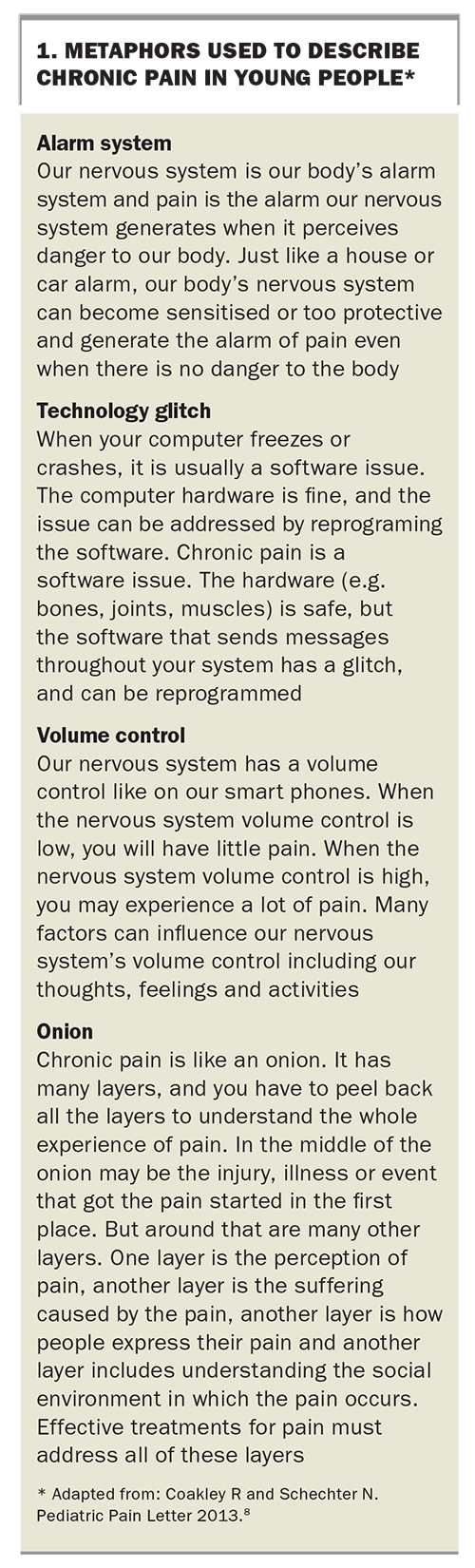
We have an evolving understanding of the neuroscience underpinning chronic pain and can translate this information into our clinical practice. Advances in research related to stress and trauma further support our ability to explain mind–body phenomena. For example, a thought, emotion or memory can influence physical sensations via multiple mechanisms, including through descending pathways from the brainstem, activation of the autonomic nervous system and activation of the hypothalamic-pituitary-adrenal axis. The cumulative impact of early childhood adversity and adversity during sensitive developmental periods can become biologically embedded. This can result in adaptive nervous system responses to new perceived threats, and shape future experiences.7 Using metaphors to explain the changes occurring in the nervous system when chronic pain occurs can help validate the young person’s experience of pain, conceptualise pain as a biopsychosocial issue and guide the way to recovery. Examples of useful metaphors to help young people understand their chronic pain are summarised in Box 1.8
{kind=link}
The biopsychosocial assessment of a young person with pain
In a biopsychosocial assessment, the medical assessment is integrated with sensitive exploration of the patient and family’s psychosocial history. The HEEADSSS structure (home, education/employment, eating and exercise, activities, drug use, sexual activity and sexuality, suicide and self-harm, safety/spirituality) can be used to guide the psychosocial history. Examples of questions to ask for each item of the HEEADSSS assessment are summarised in the Table.9 Biopsychosocial assessment is a continuous process throughout a therapeutic relationship and is typically done both with the family and with the young person alone.
{kind=link}
Although a young person may focus on their pain being the source of all their challenges, holistically exploring domains such as sleep, mood, learning, development and health literacy can present opportunities to reduce the impact of pain. For example, many young people with chronic pain experience sleep difficulties and addressing sleep early can have a positive impact on reducing pain. Exploring relationships between domains of health alongside risks and protective factors allows for personalised intervention.
The use of diagnostic labels in young people with pain
Diagnostic labels have different meanings to young people and their families. For many, having a label for their pain can provide validation and support communication around a health experience. Identifying with diagnostic labels may also help young people develop agency and social connections and provide access to conceptual frameworks for managing their condition. Conceptual frameworks can range from being biomedically focused (e.g. linking pain to tissue damage), with limited capacity to enable recovery, through to more holistic frameworks with a focus on mind–body connection and wellbeing.
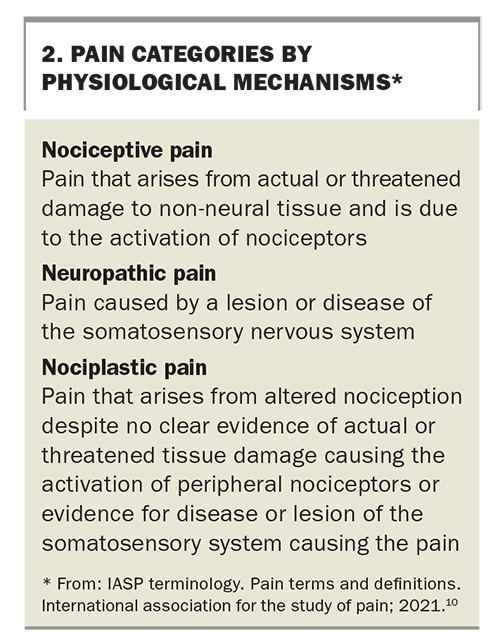
Much of the therapeutic focus for young people with chronic pain is informed by the biopsychosocial factors related to their pain rather than a diagnostic label. Understanding what each young person wants from a diagnostic label can help frame conversations around terminology. When asked to provide diagnostic clarification, it may be more useful to describe the physiological mechanisms contributing to a young person’s pain. Explaining and using the terms nociplastic, nociceptive and neuropathic pain (Box 210) in conversations with young people and their families, with relatable metaphors, can support communication about the neuroscience of pain. As many young people with chronic pain have experienced adverse childhood experiences, these discussions should be informed by knowledge of brain development and attachment.
{kind=link}
When the young person and their family value having a diagnostic label, the International Classification of Diseases, 11th revision (ICD-11) classification of chronic pain is used.1 There is flexibility in how this classification can be applied. For many patients, the use of overarching terms to describe their pain, such as ‘chronic pain’ or ‘chronic primary pain’, are sufficient. For others, more specific terms, such as ‘chronic primary widespread pain’ or ‘chronic postsurgical pain’, may be of more value. Some specific terms, such as fibromyalgia and complex regional pain syndrome, have diagnostic criteria that have not been validated in young people and can be associated with stigmatising preconceptions in the community. Consequently, caution is advised if using these terms and their diagnostic criteria in young people.
How to respond to adolescents with chronic pain
Send consistent key messages
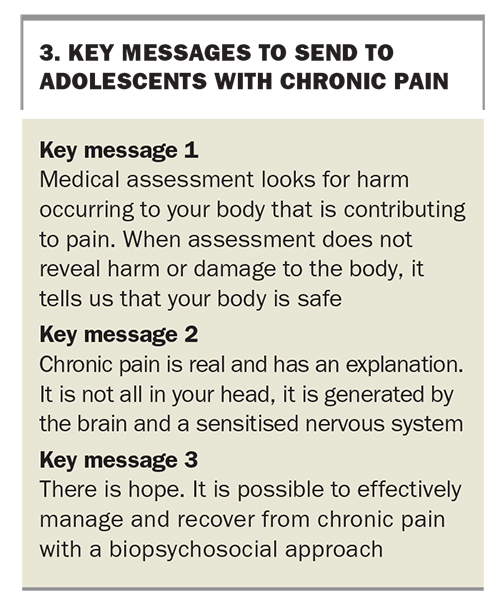
Three key messages that are important to provide consistently to young people with chronic pain are: your body is physically safe; your pain is real and has an explanation (although the brain and nervous system create pain, it is not ‘all in your head’); and it is possible to effectively manage and recover from chronic pain with a biopsychosocial approach (Box 3).
{kind=link}
Pain education
Pain education typically involves an adolescent and their family learning about the neuroscience of pain and pain as a biopsychosocial issue. This learning enables a young person to develop skills to manage and recover from chronic pain. Pain education can be delivered through discussion during a medical consultation, the self-guided use of online resources or through dedicated pain education appointments with a health practitioner. In the authors’ experience, pain education is more effective when it is more interactive, developmentally sensitive and personalised.
Medication
A small number of studies have evaluated the use of medication, including paracetamol, NSAIDs, anticonvulsants and antidepressants, for young people with chronic pain. Because of the limitations of these studies, it is not possible to draw any conclusions about the efficacy of these medications or risk of adverse effects. Furthermore, the use of most of these medications for the indication of chronic pain in young people is off label. The WHO supports the use of medication in young people with chronic pain if used judiciously on a case-by-case basis and as part of a biopsychosocial management plan.11
A mechanisms-based approach to pain can be useful to guide prescribing. For example, when significant nociceptive contributors are present, paracetamol or an NSAID may be considered. For both neuropathic and nociplastic pain, gabapentin or pregabalin or an antidepressant, such as amitriptyline, may be considered. Opioids are not recommended for chronic nonmalignant pain. Medications for other health issues may indirectly have benefits for a young person’s pain. For example, melatonin may help improve sleep or a selective serotonin reuptake inhibitor may be useful in treating anxiety or depression.
When and where to refer
Some young people with pain may benefit from referral to an allied health practitioner, a pain service or a mental health or developmental service. Indicators for referral include low levels of school attendance or participation, severe sleep disturbance, considerable use of passive coping strategies (e.g. wheelchair, medications), previously undocumented flags of neurodiversity or perceived risk of suicide or deliberate self-harm. Unfortunately, the first time a vulnerable young person’s developmental profile or mental health is considered may be in the assessment of their chronic pain. Sensitively providing referrals or scaffolding to access other services is important. Ideally, where possible, supporting the integration of chronic pain into the holistic understanding of health and wellbeing is done collaboratively with the young person and other health practitioners.
Developmentally sensitive therapy
Therapy with young people is most successful when it is developmentally sensitive and focuses on strengths. Adolescents and young adults are neurodevelopmentally driven to be socially engaged, particularly with peers, and to explore and express their identity. Building a therapeutic alliance with adolescents requires an authentic connection founded on trust, with specific attention to confidentiality and shared decision-making. Young people appreciate clinicians who are holistic and curious about their identity and life (not just their health problem), and who appropriately share aspects of their own lives. Taking a strengths-based approach can support a young person to feel comfortable and be able to engage in clinical settings. A strong therapeutic relationship is essential to creating a therapy environment where strategies for managing chronic pain are integrated into a young person’s daily life.
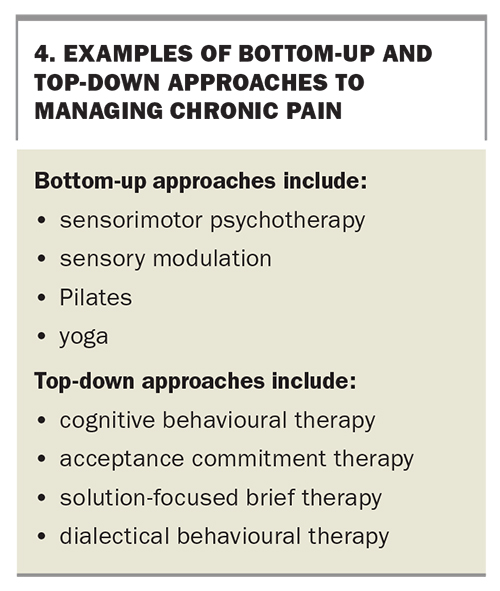
A mix of ‘bottom up’ and ‘top down’ approaches may be used to manage chronic pain (Box 4). Bottom-up approaches engage the evolutionary older regions of the brain and take a sensory, observational and regulation focused approach. Interventions may involve developing interoception and mind–body awareness while engaging in activity. During a pain flare, bottom-up approaches involving movement, music, touch and the breath can help manage the flare through soothing the nervous system. Caregivers can learn bottom-up therapeutic approaches to help the young person establish routines around sleep, movement, mealtimes and occupational engagement more broadly, and create safety for them. Furthermore, a focus on developing these skills in caregivers or teachers can help them model and respond to a young person when uncomfortable sensory and emotional experiences occur. Top-down approaches engage the neocortex and take a cognitive, talk-based and goal-directed approach.
{kind=link}
Both top-down and bottom-up approaches are needed for long-term recovery from chronic pain. Therapy sessions that incorporate regulating interventions which promote mind–body connection can help a young person to be calm, alert and interpersonally responsive. Mind–body connection supports the young person to engage in coaching, learning and cognitive-behavioural interventions. Expressive therapies (e.g. music or art therapy), partnered with psychology, physiotherapy and occupational therapy, can result in multimodal therapy sessions. The avenues to access such therapy vary between regions. Specialist adolescent pain services and adolescent medicine services tend to be located in tertiary settings. Child and youth mental health services may be more accessible regionally and can provide multidisciplinary or transdisciplinary services. Many clinicians in the community can also provide high quality care to adolescents with chronic pain, and benefit from medical support that clarifies the medical condition of the patient and the biopsychosocial conceptualisation of pain.
How to evaluate progress
Pain level, quality of life and function outcomes can help evaluate progress. Each young person will have their own sense of what meaningful function is, based on their values, sociocultural context and goals. Evaluating health and wellbeing is also key. Exploring self-efficacy in managing health and wellbeing can offer person-specific outcome measures. Working towards personalised goals supports this process.
An overall perspective on adolescent health and wellbeing is useful to inform what sustainable management and recovery looks like. Research is currently underway to better define, conceptualise and measure adolescent wellbeing.12 The proposed definition for adolescent wellbeing is when ‘adolescents thrive and are able to achieve their full potential’.12 The accompanying conceptual framework includes assessing:
- adolescent physical health and nutrition
- social connectedness
- access to a safe and secure living environment
- access to learning and employment opportunities
- agency and resilience.
This definition and conceptual framework are useful tools in assessing improvements in young people’s health and wellbeing.
Conclusion
Adolescents and young adults in our community often experience chronic pain and may experience difficulties across functional domains. Young people with chronic pain experience higher rates of adverse childhood experiences, mental health issues and neurodiversity compared with the general population. Medical assessment is an integral part of the biopsychosocial assessment of a young person with chronic pain. The HEEADSSS structure can help guide the psychosocial assessment and reminds us that holistic care is essential when working with young people. Mechanistic descriptors to classify pain can be used in discussions with patients and families. In responding to young people with pain, a validating and hopeful approach is essential. All communication should consistently reinforce that their body is physically safe, their pain is real and can be explained, and that effective management and recovery is possible.
Management often includes pain education, which is most effective when it is personalised and interactive, and can help inform further bottom-up and
top-down interventions. It is not possible to draw conclusions about the efficacy or safety of medications for chronic pain in young people from the current literature; when used, they should be used judiciously on a case-by-case basis. When evaluating progress, pain, quality of life and function can be assessed. A proposed definition and framework for adolescent wellbeing can provide guidance on what sustainable management and recovery can look like for a young person with pain. MT
COMPETING INTERESTS: None.