Sudden sensorineural hearing loss: an urgent otological presentation

Sudden sensorineural hearing loss (SSNHL) is an otological condition that requires urgent assessment and treatment in consultation with an ENT surgeon. A structured approach to the assessment of patients presenting with sudden hearing loss can help differentiate between SSNHL and other causes of hearing loss.
- Sudden sensorineural hearing loss can be a debilitating condition; however, overall it has a good prognosis.
- History, examination, tuning fork tests and pure tone audiometry can help differentiate between sensorineural and other causes of hearing loss.
- Quality evidence for treatment regimens for sudden sensorineural hearing loss is limited, but the best recommended treatment is timely oral or intratympanic steroids.
- Early referral to an ENT specialist is important.
A sudden and dramatic drop in hearing is a reasonably common presentation to public hospital emergency departments, GP practices and ENT departments. It can be a frightening symptom for patients and requires urgent assessment when caused by sudden inner ear or sensorineural loss. This article focuses on sudden sensorineural hearing loss (SSNHL), including recognising symptoms to distinguish SSNHL from other forms of sudden onset hearing loss and the options for treatment. Management of SSNHL is controversial because the evidence for some treatments is limited and mild SSNHL has a high spontaneous recovery rate. Although no treatment is proven, there are guidelines for initial management. There is much still to learn about SSNHL and more clinical trials are needed to establish evidence-based management.
Mechanism of hearing
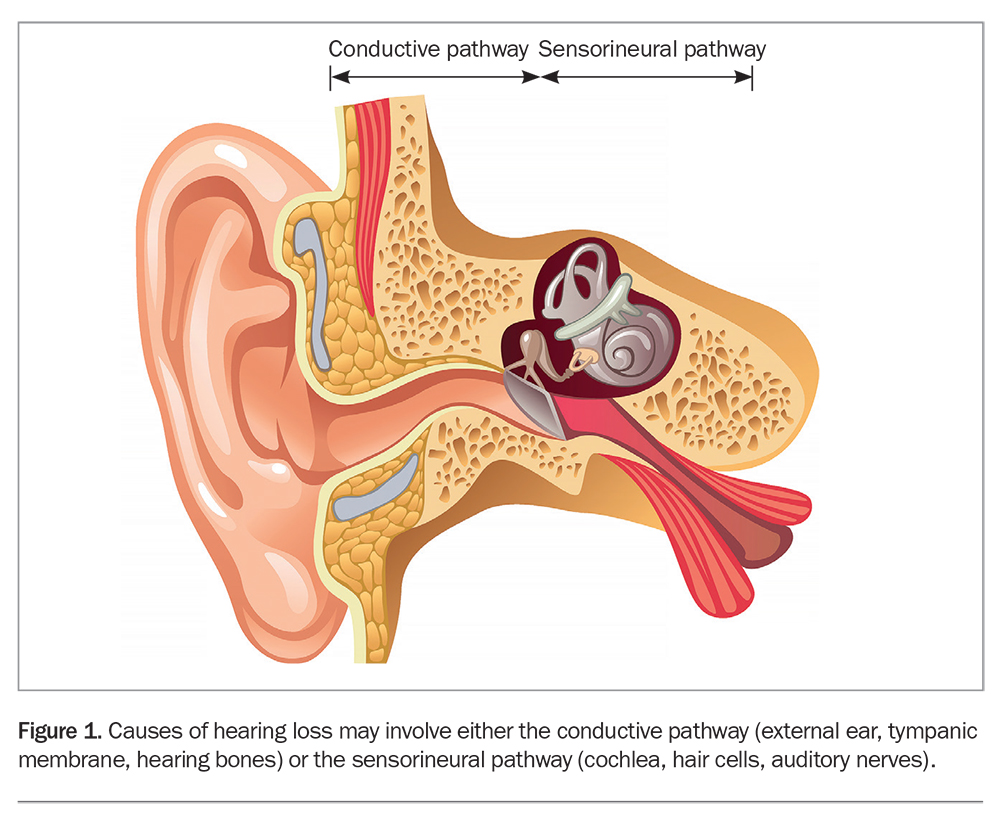
Normal hearing is dependent on an intact and functioning auditory pathway. The anatomy of the ear can be divided into the outer, middle and inner ear. The outer ear is composed of the pinna and external ear canal, which capture and focus the sound towards the tympanic membrane. Sound energy then vibrates the tympanic membrane, which transmits this energy to the middle ear space and hearing bones (ossicles). The ossicles connect via the stapes to the round window of the cochlear (inner ear), where this energy is transmitted to the fluid within the cochlear, and the hair cells are activated by the movement of fluid. Action potentials are created by hair cell movement in the adjacent auditory nerve fibres, producing electrical signals that travel to the auditory processing centres of the cerebral cortex. Thus, sound energy is converted into electrical energy via the conductive and sensorineural pathways of hearing. Disturbance of these pathways leads to hearing loss (Figure 1).
{kind=link}
What is SSNHL?
Sudden hearing loss is a rapid onset of subjective impairment of hearing in one or both ears. This can be conductive, sensorineural, or mixed in nature, with a wide differential diagnosis. Physical examination, tuning fork testing and pure tone audiometry can help to distinguish SSNHL from other differential diagnoses.
SSNHL has been defined as hearing loss that is sensorineural in nature of at least 30 dB over at least three consecutive frequencies within a 72-hour window. The definition assumes premorbid hearing in the affected ear is similar or identical to hearing in the unaffected ear. SSNHL is considered idiopathic when no identifiable cause for hearing loss can be identified, and is the case in more than 90% of presentations.
Presentation
History and examination are important in the diagnosis of SSNHL to differentiate sensorineural hearing loss from conductive hearing loss and to ascertain which ear is affected.
Patients with idiopathic SSNHL usually experience immediate or rapid hearing loss, often reported upon awakening. Hearing loss can involve any frequency range and severity can be mild, moderate or severe to profound. Other common associated symptoms include tinnitus, vertigo or dizziness and, less often otalgia and paraesthesia. However, associated symptoms are nonspecific and may not differentiate between conductive and sensorineural hearing loss.
Many patients experience a sensation of a blocked ear or aural fullness initially and do not attribute this to hearing loss, given it is common for wax impaction, otitis media or eustachian tube dysfunction to cause a similar sensation. For this reason, patients may not seek attention immediately or can be inappropriately reassured without investigation and treatment.
Most cases of SSNHL are unilateral with an equal distribution of right- and left-sided hearing loss. Bilateral SSNHL is rare (3%). However, an underlying cause is far more likely to be identified in bilateral cases, such as systemic autoimmune disorders or hypercoagulation disorders. There should be a high suspicion for SSNHL if a patient with a history of unilateral SSNHL presents with similar symptoms on the contralateral side.
Natural history
Spontaneous recovery occurs in 30 to 60% of patients with idiopathic SSNHL, generally within the first few weeks. If symptoms persist longer than three months, spontaneous recovery is unlikely.
Epidemiology
The incidence of SSNHL is estimated to be between five and 20 cases per 100,000 per year.2 However, estimates vary due to spontaneous recovery and failure to seek medical attention. Idiopathic SSNHL can occur at any age but most commonly affects individuals in their 40s to 60s. Incidence varies from 11 per 100,000 in those younger than 18 years to 77 per 100,000 for people 65 years and older.3,4 In general, similar numbers of men and women are affected.5
Risk factors
Most reported risk factors for SSNHL are related to the cardiovascular system, as the inner ear may be vulnerable to cardio- vascular insults, as well as hypercholesterolaemia, smoking, increased alcohol consumption and low serum folate, but no definitive associations have been made. Other risk factors include mutations in factor V Leiden and the methylenetetrahydrofolate reductase (MTHFR) genes, hyperhomocysteinaemia, elevated factor VIII (essential blood-clotting protein) and deficiencies of antithrombin and protein C and S, but screening for these is not cost effective.
Pathophysiology
The complete pathophysiology of SSNHL remains unknown and is likely to be multifactorial. The following theories have been proposed.6
The labyrinthine viral infection theory
Although the evidence that implicates viral infection in SSNHL is circumstantial, proposed mechanisms include:
- direct viral invasion of the fluid spaces of the cochlea (cochleitis)
- direct invasion of the cochlear nerve (neuritis)
- reactivation of a virus that is latent within the tissues of the inner ear.
Viruses that have been implicated include mumps, measles, rubella, herpes and varicella zoster. However, there are significant challenges in investigating the viral theory and such cases likely only account for a small fraction of idiopathic SSNHL.
The labyrinthine vascular compromise theory
Vascular occlusion, or ischaemia, is a possible mechanism for SSNHL because the cochlea is an end organ with respect to its blood supply. The labyrinthine artery branches into a cochlear and vestibular artery, both end vessels, which makes them more susceptible to thromboembolic events, reduced blood flow or vasospasm.
The intracochlear membrane rupture theory
Rupture of the thin membranes that separate the middle ear from the inner ear at the oval and round windows, as well as inside the cochlea between the perilymphatic and endolymphatic spaces, could theoretically produce hearing loss. Mixing of the the perilymph and endolymph may alter electrolyte homeostasis, endocochlear potential and hair cell function.
When the membranes repair and recover spontaneously, and if hair cells are still viable, hearing loss may be partial or fluctuating, which makes this an attractive theory, fitting with the clinical presentation.
The immune-mediated inner ear disease theory
Immune-mediated inner-ear disorders, including both organ-specific inner ear disease (Cogan’s syndrome) and systemic autoimmune disorders, may be a cause for SSNHL.
A distant viral infection may act as a trigger for an autoimmune response, which produces antibodies that cross-react with an inner ear antigen, activating cellular stress pathways within the cochlea.
Diagnosis
The diagnosis of SSNHL can be made based on findings from the patient’s history, otoscopy, tuning fork tests (Weber and Rinne) and pure tone audiometry, followed by imaging. It is important to exclude causes of conductive hearing loss, which may present similarly with reduced hearing or a blocked ear. A suggested approach to the assessment of sudden hearing loss in general practice is outlined in Flowchart 1.
Otoscopy
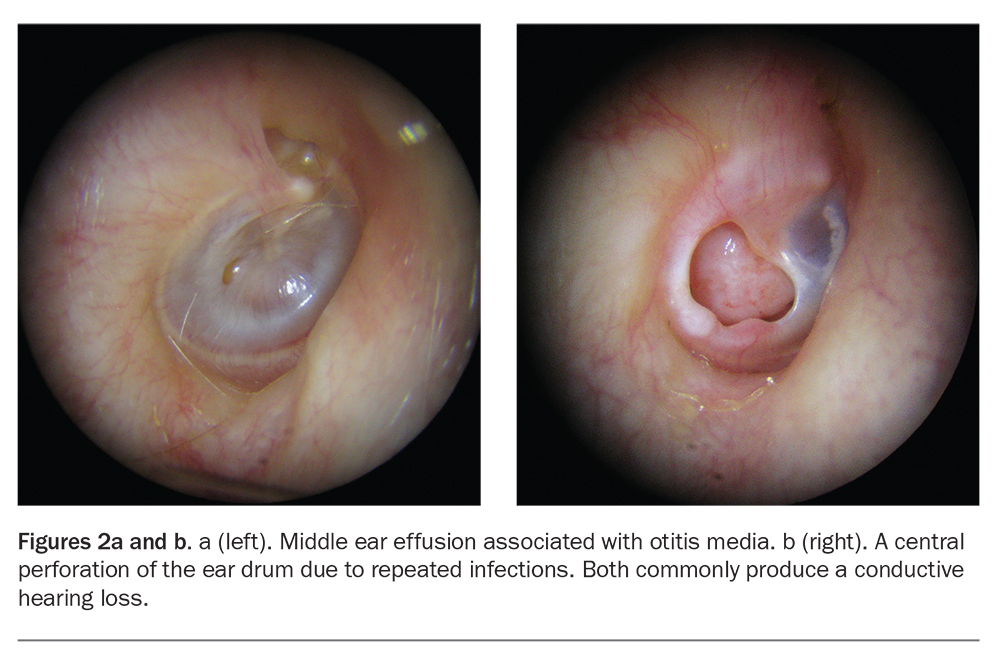
Otoscopic examination of the external ear canal and tympanic membrane can diagnose or exclude many causes of conductive hearing loss. A patent ear canal with no occluding mass excludes wax impaction, foreign bodies, tumours, exostoses and stenosis. Visualisation of a healthy intact drum that is mobile on pneumatic insufflation excludes cholesteatoma, otitis media and middle ear effusions (Figure 2). In patients with SSNHL, the otoscopic examination is generally normal.
{kind=link}
Tuning fork tests
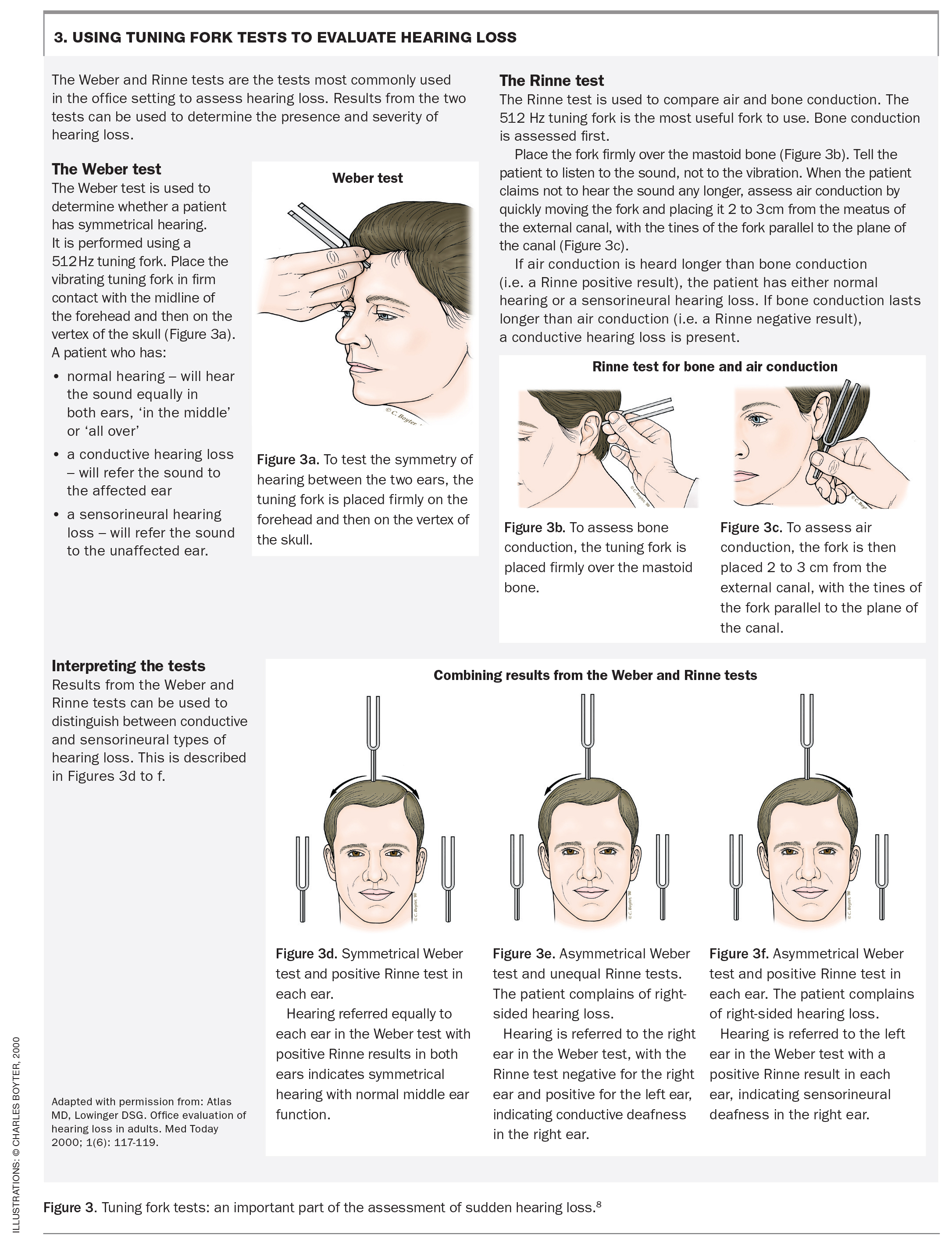
The Weber and Rinne tests distinguish between sensorineural and conductive hearing loss (Figure 3). They are performed with a 512 Hz tuning fork and compare symmetry between the two ears (Weber), as well as the efficiency of hearing via air conduction and bone conduction (Rinne). The technique for how to perform a tuning fork test is important and will improve with practice. Poor technique can lead to a false result.8
{kind=link}
Audiometry
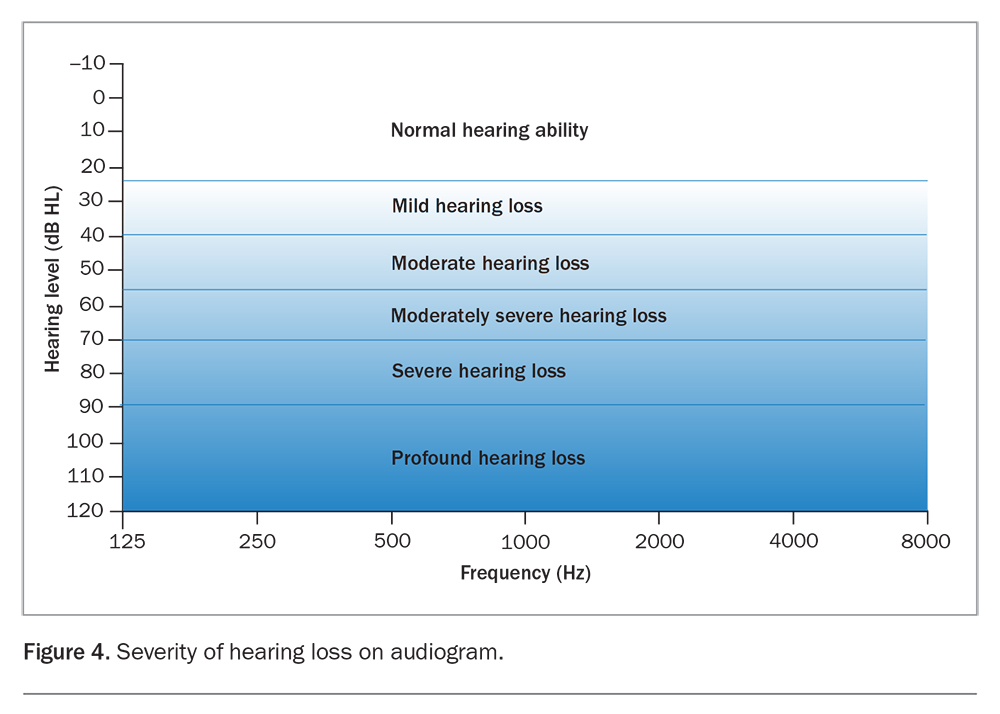
A pure tone audiogram and tympanometry are essential in the diagnosis of SSNHL. Air conduction thresholds and bone conduction thresholds recorded under calibrated conditions are needed to distinguish between sensorineural and conductive hearing loss. Air conduction thresholds are obtained using headphones and bone conduction by directly stimulating the cochlea with a vibratory stimulator on the mastoid. They are charted on an audiogram using symbols, measuring intensity (loudness) of sound heard in decibels against the frequency (pitch) of the sound (250 to 8000 Hz) (Figure 4).
{kind=link}
A basic understanding of how to interpret an audiogram is important. Figure 4 shows ranges of hearing loss severity on an audiogram chart. An audiogram can determine if the patient has normal hearing, sensorineural, conductive or a mixed loss and whether it is symmetrical or asymmetrical (Table 1, Figure 5).
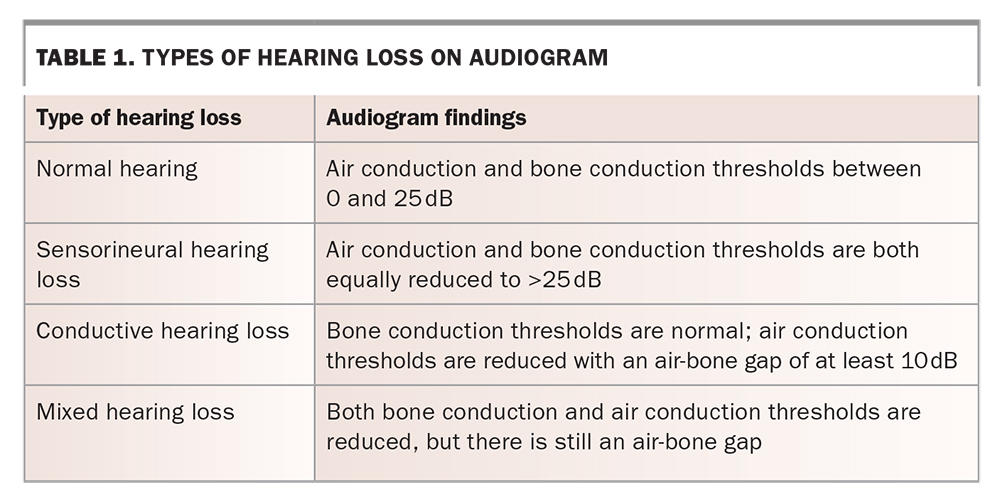{kind=link}
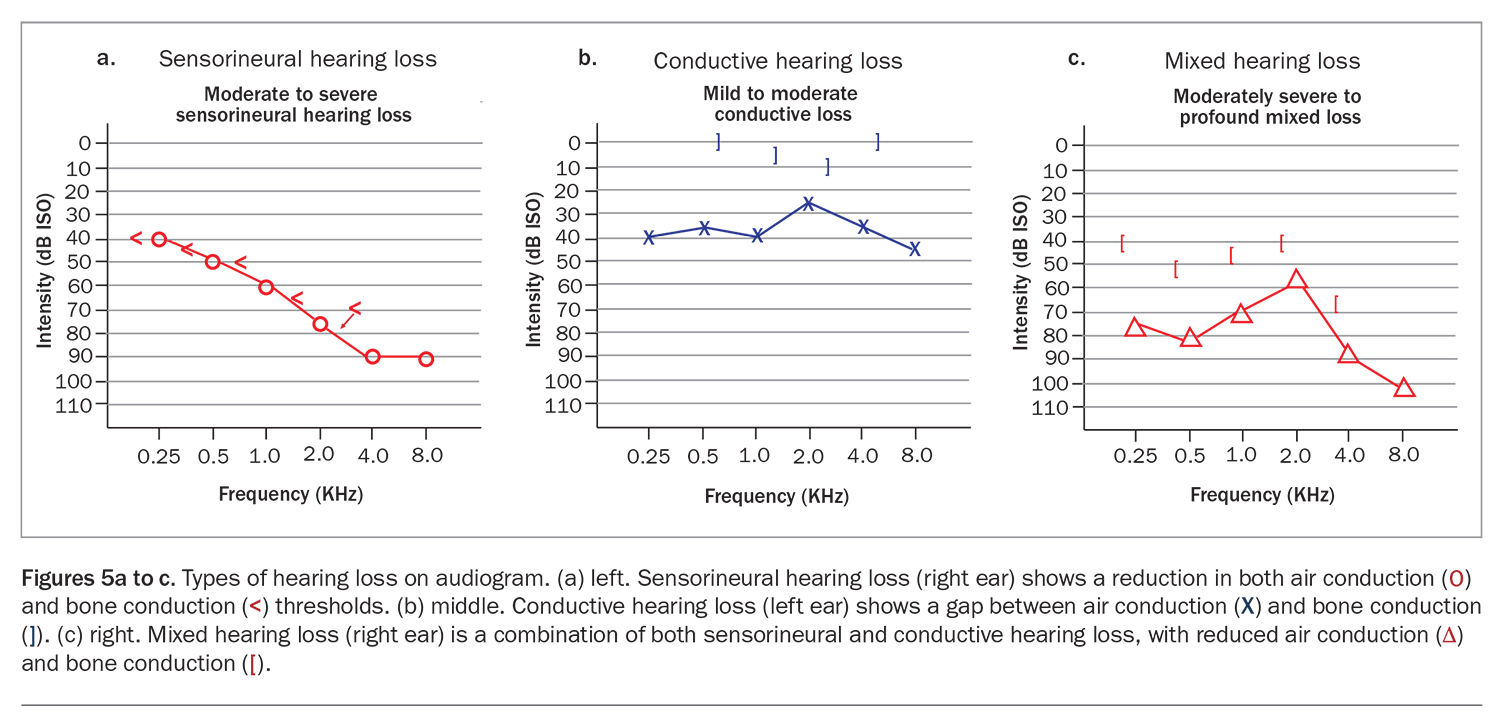{kind=link}
More complex tests of inner ear function and the central auditory pathways, such as otoacoustic emissions and auditory evoked brainstem potentials, require specialist interpretation.
Otoacoustic emissions
Otoacoustic emissions (OAEs) are relevant in the evaluation of sensorineural hearing loss. They are sounds given off by part of the cochlea, either spontaneously or when it is stimulated by soft clicking sounds (distortion product evoked OAEs). Present distortion product evoked OAEs indicate normal functioning of the outer hair cells. Absence of OAEs indicates a problem with the sensorineural pathway. The presence of OAEs in measurements early in idiopathic SSNHL shows a good prognosis for hearing recovery.9
Speech audiometry
Speech audiometry is important to assess functional deficit and determine which forms of auditory rehabilitation will be beneficial.
Imaging
MRI of the petrous temporal bone with contrast is the most important imaging study in sensorineural hearing loss. It is indicated in all patients with neuro-otological symptoms, particularly in patients with SSNHL that is unilateral or idiopathic. Special attention is paid to the inner ear, looking for potential causes of SSNHL, such as an acoustic neuroma.
CT scans are not recommended routinely for SSNHL. A CT scan may be indicated if there are focal neurological findings, a history of trauma or chronic ear disease or in patients in whom MRI is contraindicated (e.g. patients with pacemakers and cochlear implants).
Blood tests
Commonly performed blood tests include full blood count, coagulation studies, serum electrolytes, erythrocyte sedimentation rate, autoimmune screening, metabolic panel and thyroid function tests. However, the yield is generally low and blood tests are not recommended by the 2019 American Academy of Otolaryngology – Head and Neck Surgery Foundation Clinical Practice Guideline: Sudden Hearing Loss (Update) unless there is suggestion of an underlying systemic illness.7
Differential diagnosis
There is a large differential diagnosis for the symptom of acute unilateral sensorineural hearing loss (Box 1). Sudden hearing loss should only be termed idiopathic when no other cause can be identified or considered probable. Most of the causes listed in Box 1 can be excluded using a simple battery of tests that are available in general practice.
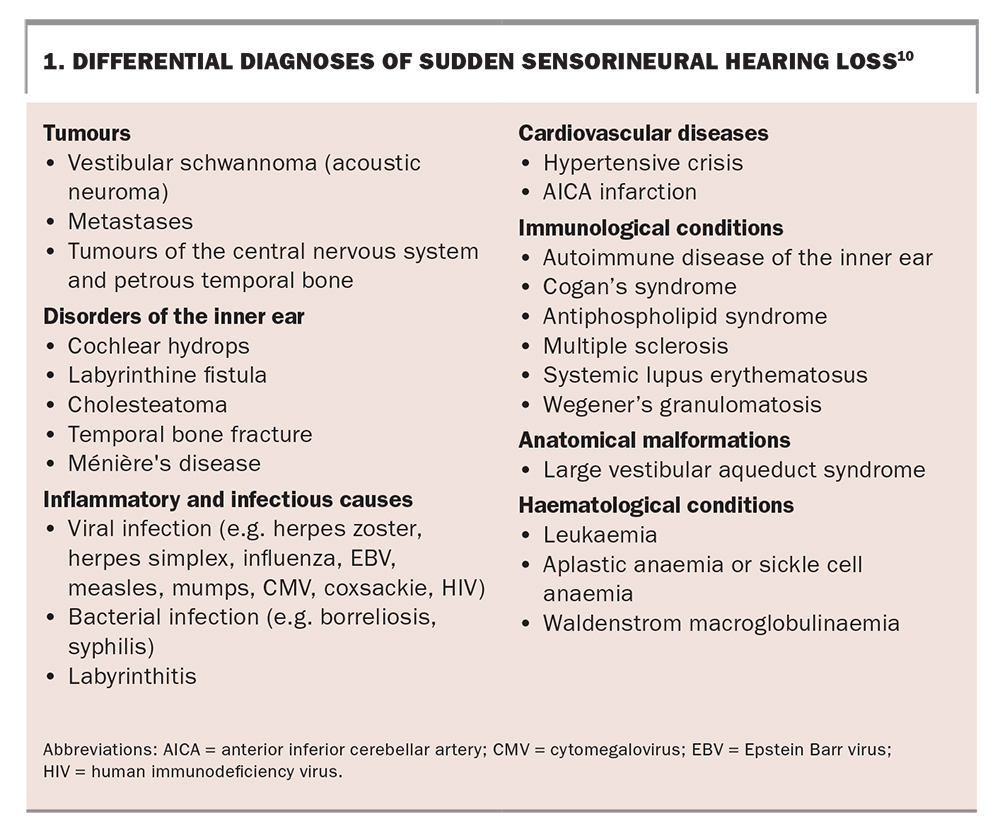{kind=link}
Management of idiopathic SSNHL
Patients with idiopathic SSNHL should be educated about the natural history of the condition and the risks and efficacy of available treatments to facilitate a joint decision-making process between the clinician and the patient. A suggested approach to management is outlined in Flowchart 2.
Systemic corticosteroids
Corticosteroids are currently the most widely accepted first-line therapy for SSNHL. However, the evidence-base for efficacy of corticosteroids remains unclear. The 2019 Clinical Practice Guideline: Sudden Hearing Loss (Update) recommends that the clinician may offer oral corticosteroids as a first-line therapy within two weeks of symptom onset after discussing the limited documented evidence for their efficacy, although corticosteroid therapy should be considered up to six weeks following onset of symptoms.7 Options for systemic corticosteroids include oral prednisolone or oral or intravenous methylprednisolone or dexamethasone.
The dose of corticosteroids, the effect of timings and method of systemic administration remain contentious. Intravenous administration of corticosteroids has not been shown to be any more efficacious than oral prednisolone. Dosage and duration recommendations can be found in Table 2. Generally, a high dose (e.g. prednisolone 1mg/kg/day) is used for seven to 14 days, followed by a weaning course over a similar timeframe.
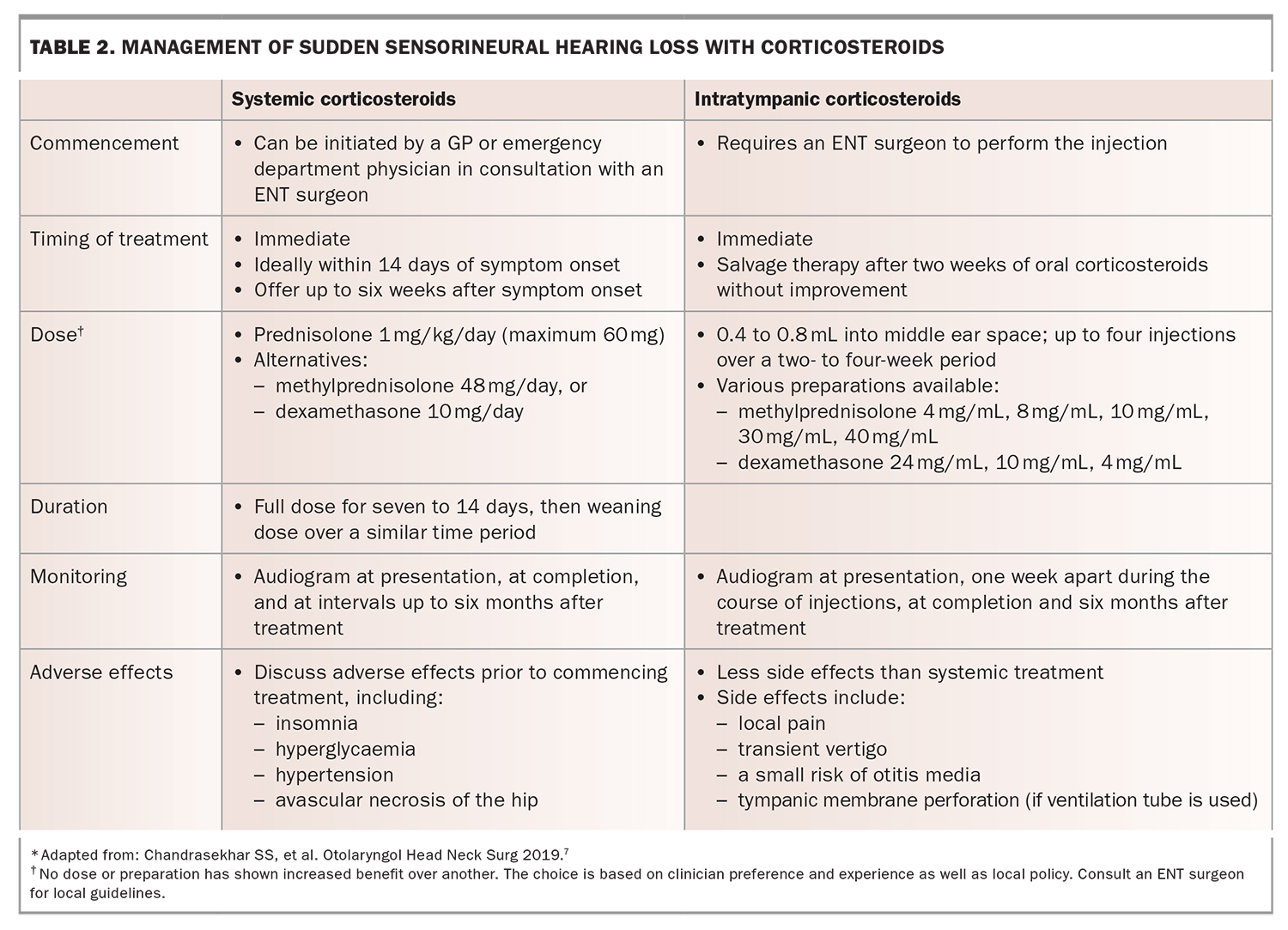{kind=link}
There are numerous side effects of systemic corticosteroid administration that need to be weighed with the potential benefits as they can occur even in short-term use (Box 2). Given deafness can be an extremely debilitating condition, however, if there is even a small possibility of restoring or improving hearing then it is a reasonable treatment to offer. As such, this has become standard practice. However, there is a large role for shared decision making with patients.
{kind=link}
When systemic corticosteroids are contraindicated, such as in pregnancy, severe psychiatric illness or extreme hypertension, an ENT surgeon should be consulted for consideration of intratympanic corticosteroids as a first-line treatment (Table 2).
Intratympanic corticosteroids
Intratympanic corticosteroids are administered either by direct injection through the tympanic membrane or insertion of a tympanostomy tube (grommet) for repeated administrations. The main indications for intratympanic corticosteroid injections are: salvage therapy after systemic corticosteroids or when systemic corticosteroids are contraindicated.
Intratympanic corticosteroid administration has several advantages over systemic corticosteroids, including targeted drug delivery resulting in possibly higher inner ear concentration, minimal systemic absorption or side effects and that they are a good option in patients in whom systemic corticosteroids are contraindicated (e.g. pregnancy, extreme hypertension, diabetes or psychiatric illness).11-13
Other therapies
Hyperbaric oxygen therapy (HBOT) has been proposed based on the theory of vascular compromise as the aetiology for SSNHL, with the purpose of increasing the oxygen supply to the possibly ischaemic cochlear structure. The 2019 Clinical Practice Guideline: Sudden Hearing Loss (Update) states that HBOT could be used as an optional therapy within two weeks of onset of symptoms or as salvage therapy in combination with corticosteroids therapy within one month of onset of SSNHL.7
The potential limited benefits of HBOT need to be weighed against the costs, availability and side effects, including barotrauma, oxygen toxicity, worsening of cataracts, fatigue and seizures. It is also costly, time consuming and usually requires travel on the patient’s part. Good patient selection is important if considering this therapy.
A number of other therapies have been proposed. Antiviral medications have been trialled based on a possible aetiological role of subclinical viral labyrinthitis. However, antiviral medications in combination with oral corticosteroids have not been shown to give any additional outcome benefit and so are not routinely recommended. If sudden hearing loss is accompanied by a facial nerve palsy, such as in Ramsay Hunt Syndrome, then antiviral medications are indicated. Other therapies that do not have a significant evidence-base include volume expanders, vasodilators, carbogen therapy, calcium channel blockers, pentoxifylline, prostaglandin E1, thrombolytics, antioxidants, histamines, magnesium, diuretics and other herbal remedies.
Auditory rehabilitation
An audiogram should be obtained three to six months after the onset of symptoms to quantify the extent of permanent hearing loss. There is unlikely to be any improvement in hearing after this time and it is reasonable to assume this will be the patient’s long-term level of hearing.
Patients with permanent hearing loss should be referred to an audiologist for fitting of a traditional in-ear hearing aid or Bilateral Contralateral Routing of Signals (BiCROS) hearing aid, which transmits the sound from the affected ear to the unaffected ear and is for people with single-sided deafness. The level of functional impairment depends on several factors, including the severity of hearing loss, the frequencies affected, whether the hearing in the contralateral ear is normal or whether the affected ear was the only hearing ear, and the patient’s age, occupation and social circumstances. Tinnitus and vertigo may also be bothersome symptoms that accompany hearing loss. Some audiologists can provide specialised tinnitus training and counselling.6
For patients with profound hearing loss that cannot be aided, a cochlear implant may be considered. A cochlear implant is an electronic prosthesis that works by bypassing the residual damaged hearing elements within the organ of Corti and directly stimulating the intact nerve endings in the auditory nerve.14
Prognostic factors
The overall prognosis of SSNHL is good; about two thirds of patients recover some degree of hearing, although not necessarily back to normal or the same as the unaffected side. Most patients with idiopathic SSNHL will recover within three months, with 30 to 60% of patients experiencing spontaneous recovery. This proportion may be improved by the timely use of corticosteroids, but we do not have good data to support the impact of this.1
The most important prognostic factor is the degree of hearing loss at presentation. The less severe at presentation, the greater the likelihood of recovery. Other factors indicating a poor prognosis for hearing recovery include associated vertigo, late recovery with or without treatment and associated systemic features (i.e. a high ESR or CRP).15
Features suggestive of a favourable prognosis of hearing recovery include:
- isolated high or low frequency loss (compared with a flat pattern); isolated low frequency has the greatest chance of recovery
- presence of tinnitus
- absence of vertigo
- absence of underlying systemic illness.16
Conclusion
SSNHL is an otological condition that requires urgent treatment and specialist referral. It is important for clinicians to have a high index of suspicion and an understanding of the diagnosis and need for prompt management. In the initial assessment, simple tuning fork tests and otoscopy can exclude conductive causes, such as middle ear effusion, wax impaction and infection, which might have similar presentations and do not require specialist referral. If there is uncertainty about the diagnosis, it is important to arrange an urgent audiogram with air and bone conduction, after clearing the ear canal of any obstruction.
There remains a lack of consistency in treatment regimens due to low efficacy evidence; however, the 2019 American Academy Clinical Practice Guideline: Sudden Hearing Loss (Update) should be followed. Once the sensorineural nature of the hearing loss is established and a diagnosis of SSNHL is suspected, patients require urgent referral to an ENT specialist for consideration of corticosteroid treatment. MT
COMPETING INTERESTS: None.