Japanese encephalitis – a recent rise in Australian cases

Japanese encephalitis is a potentially fatal form of viral encephalitis that is found predominantly in South-East Asia; however, there has been a recent rise in case numbers in Australia. Key aspects of prevention and management include risk reduction strategies at the individual and public health levels, as well as rapid and effective diagnosis with timely involvement of local infectious disease services.
Japanese encephalitis (JE) virus is a mosquito-borne flavivirus that is found predominantly in South-East Asia and is the leading cause of childhood viral encephalitis in many Asian countries.1 It has not been known to be endemic in Australia, and a recent rise in Australian cases is of concern. There is a 30% mortality rate in those that do develop encephalitis, as well as a high incidence of neurological deficits in survivors.2 Simple and effective preventive strategies are available that should be recommended to those at risk.
The virus
JE is caused by a single-stranded RNA flavivirus virus related to dengue, zika and yellow fever viruses.1,2 Four genotypes have been identified. Genotypes I and III tend to cause summer epidemics in northern temperate areas, whereas genotypes II and IV result in endemics in southern tropical regions.3 After the initial mosquito bite, a viraemia develops in the host.2 This is usually cleared before it can reach the central nervous system; however, if it does cross the blood-brain barrier it can cause a severe neuroinvasive disease and encephalitis.2
History and epidemiology
The first case of JE was identified in 1871 in Japan.4 This was followed by a Japanese outbreak of over 6000 cases in 1924.4 Currently, more than three billion people live in epidemic or endemic countries across Asia, the West Pacific and Northern Australia.5 In 2019, India had the highest prevalence of JE, followed by Bangladesh and China.6 Widespread vaccination campaigns have successfully controlled the disease in several countries, including Japan, Korea and Taiwan.
In Australia, the first reported cases were in 1995, across several islands in the Torres Strait.7 Before the recent events, the last locally acquired Australian case was in 1998 at the Cape York Peninsula, on the mainland of Australia, with seroconversion seen among sentinel pigs.8 The distribution of JE virus is shown in Figure 1.9
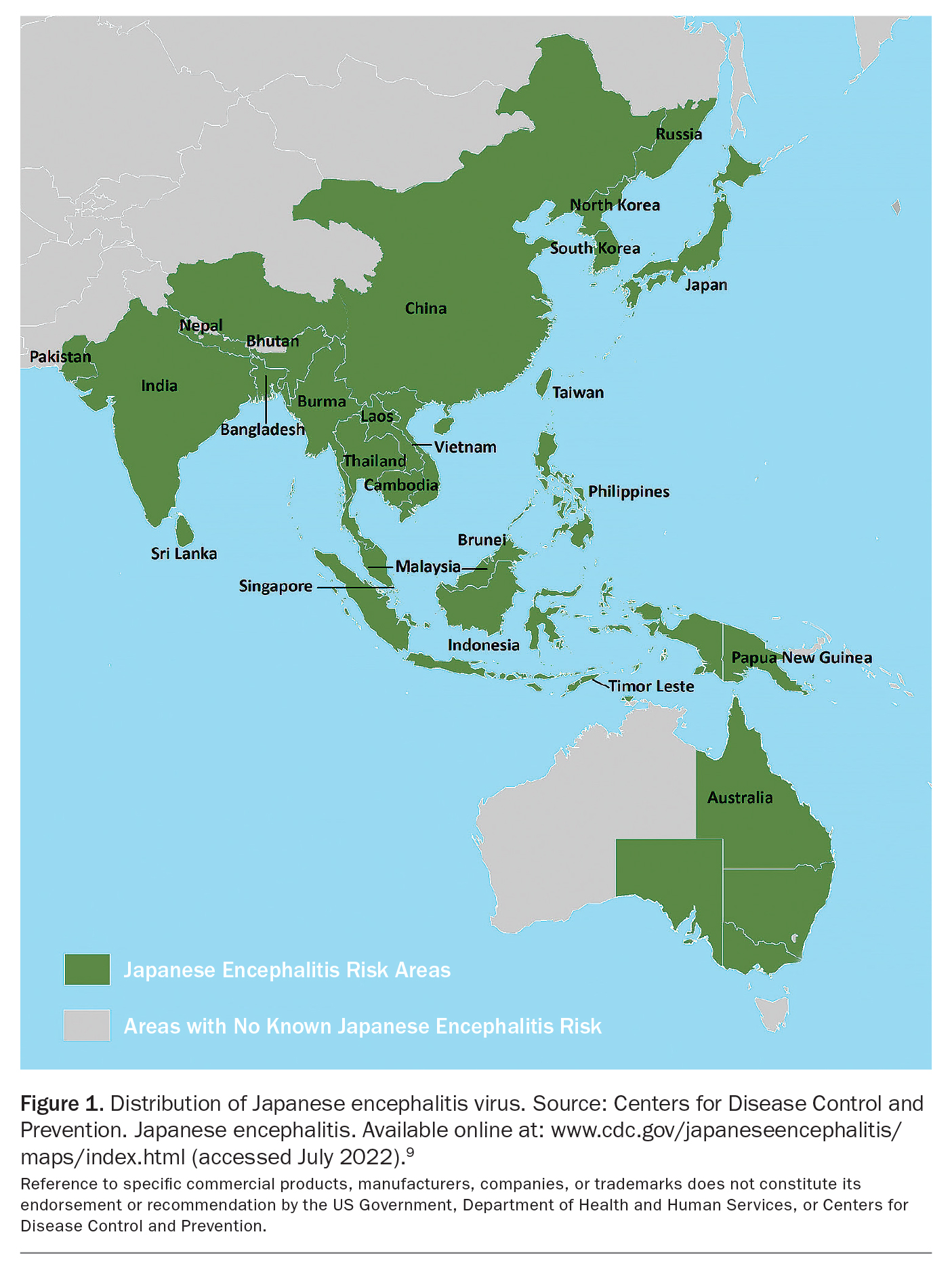{kind=link}
Life cycle and transmission
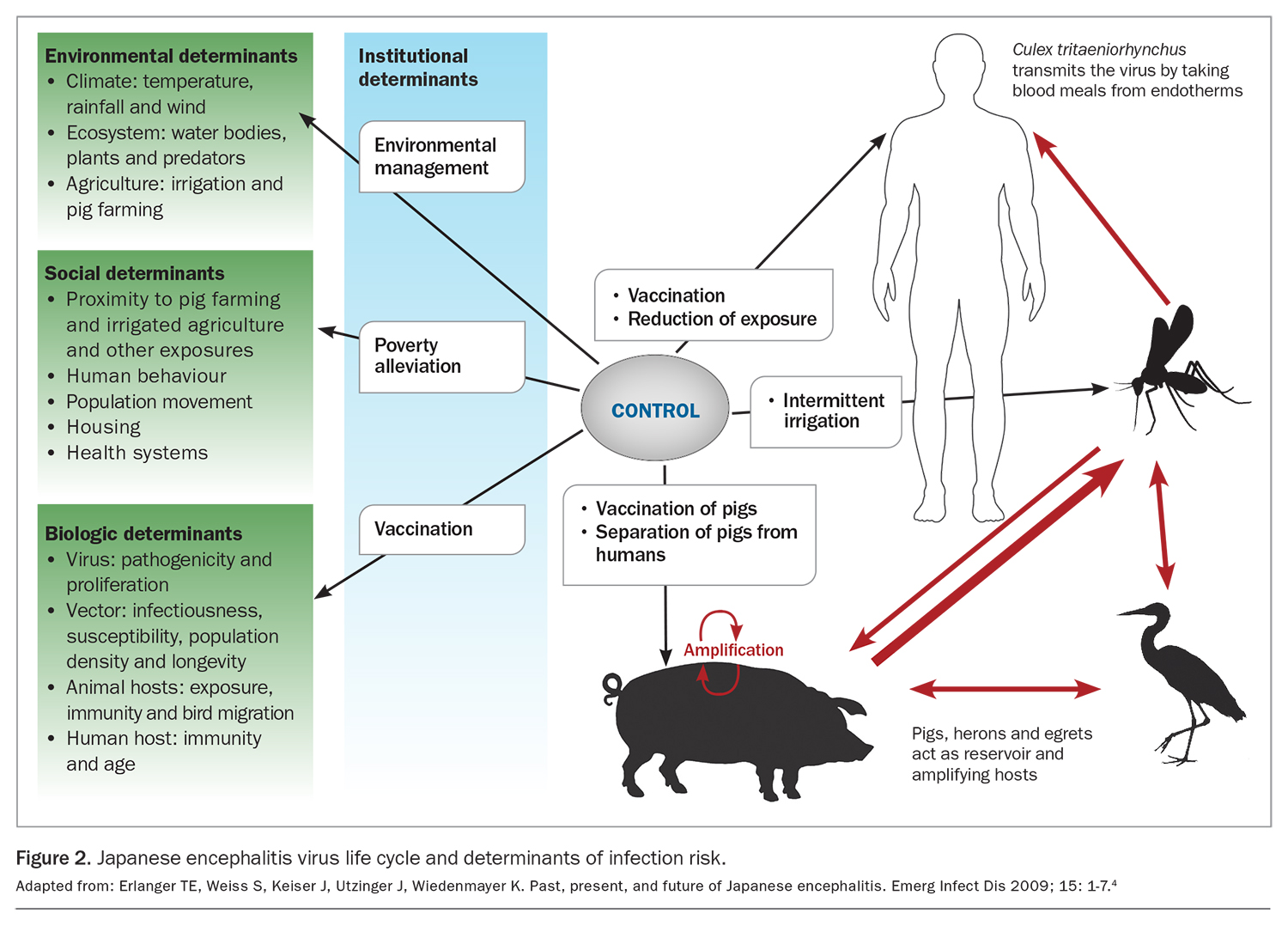
JE virus has an enzootic life cycle, affecting animals in a particular district or season (Figure 2). Its vector, female mosquitoes mostly of the Culex genus, together with the main reservoir and amplifying hosts, wading birds and pigs, were identified in 1938.4 JE virus has been isolated from 30 species of mosquitoes; Culex tritaeniorhynchus is the primary vector globally.1 This species has a predilection for breeding in rice fields and areas where standing water accumulates, for example during flooding or through irrigation.1 It tends to have an outdoor natural feeding pattern in these areas.10
{kind=link}
Human transmission occurs after bites from an infected female mosquito. Although the virus can be detected in humans, horses and cattle, they are ‘dead-end’ hosts because the levels of viraemia reached are insufficient to enable ongoing transmission to mosquitoes.1 Pigs and wading birds, such as herons and egrets, are the most common hosts that are capable of sustaining transmission (amplifying hosts), as they generate the high level viraemia required for ongoing transmission back to mosquitoes.1 Although these hosts do develop immunity shortly after initial infection, the commercial slaughtering of pigs enables this susceptible population to be regularly replenished.11
Adult pigs typically do not show signs of disease, except infected sows may have stillbirths. The mosquito usually only flies up to 3.2 km and thus it is humans living close to rice fields, water sources and piggeries who are at greater risk of infection.
After periods of heavy rainfall and higher temperatures, mosquito breeding increases with a resulting rise in JE cases.12 JE virus has also been isolated from bats, which may result in overwintering of the virus in epidemic regions.1 In Australia, Culex annulirostris has been determined to be the primary vector, with investigations showing that this species takes blood meals from pigs.13
Why has it returned to Australia?
Climate change has likely played a role in the current re-emergence of JE in mainland Australia. Factors such as the La Niña weather phenomenon have resulted in heavier rainfall than usual, and migratory water birds have subsequently travelled further south, accompanied by increased mosquito breeding. The Australian Government Bureau of Meteorology has listed a strong La Niña event for 2021 to 2022.14 Further to this, longer-term climate change may enable mosquitoes to inhabit areas of higher elevation and latitudes.
Preventing the impact of JE virus
The risk of JE can be reduced with measures undertaken by individuals and public health interventions that aim for vector control or reduced disease impact. On an individual basis, vector avoidance using chemical insect repellents (such as N,N-diethyl-meta-toluamide [DEET]) applied to the skin or insecticide vapour dispensing units can help reduce mosquito bites. In addition, physical barriers, such as insect screens on buildings and wearing long-sleeved, light-coloured clothing, can help.
Public health measures include vector control with outdoor insecticide spraying and minimising open water sources available for breeding. This is especially important for at-risk locations, such as piggeries. Early detection and reporting of suspected cases is essential to inform a rapid and effective public health response.
Targeted vaccination of people with direct exposure or proximity to pigs and mosquitoes is an effective way of reducing the JE disease burden. Current recommendations for vaccination have been expanded (from the previous recommendation for travellers) to include piggery workers, pork abattoir workers, laboratory workers who may be exposed to the virus, environmental health officers and entomologists working with mosquitoes, and people who live or work on the outer islands of the Torres Strait.15 Recommendations may change based on emerging data. Australia has two safe and effective licensed vaccine options against JE virus; a brief overview of these vaccines is provided in the Table. The latest recommendations for JE vaccination can be found in the Australian Immunisation Handbook, which should be referred to before administration of any of the vaccines (https://immunisationhandbook.health.gov.au/contents/vaccine-preventable-diseases/japanese-encephalitis).
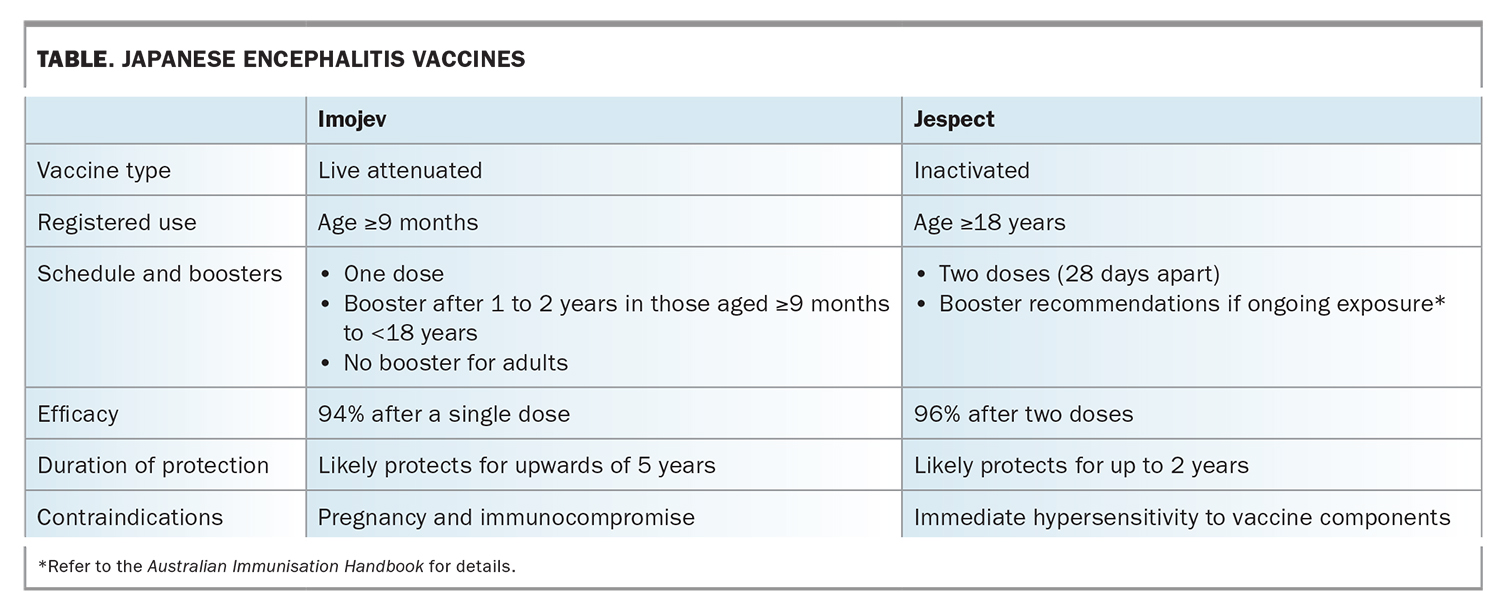{kind=link}
JE is a notifiable disease and cases are monitored using the National Notifiable Diseases Surveillance System (NNDSS). Sentinel pigs and chickens have been replaced with mosquito surveillance, which is faster to implement and more flexible. Further, more intensive ('enhanced') surveillance may be needed based on newly detected cases when intervention for disease control can be readily implemented.16 Although effective, this approach is resource-intensive and requires significant co-ordination.
Current situation in Australia
JE was declared a communicable disease incident of national significance on 4 March 2022.17 As of 19 July 2022, there have been a total of 40 human cases of JE in Australia, 29 of which had definitive laboratory evidence (NSW 13, Victoria 9, South Australia 5, Queensland 2). Eleven were probable cases, defined as having an epidemiological link and/or symptoms and laboratory suggestive evidence (South Australia 4, Victoria 3, Queensland 4). Unfortunately, five deaths have been reported nationwide.18 More than 70 piggeries across Victoria, Queensland, New South Wales and South Australia are known to be infected with JE virus.19
Financial support of $69 million was announced on 11 March 2022, including $28 million for additional vaccines.20 A national working group has been convened, consisting of communicable disease, vaccine and arbovirus experts. This group will advise of surveillance measures, vector control and identification of populations at risk and help inform the vaccine rollout. Further public health communications will help inform the ongoing response to JE.
Clinical manifestations of JE
JE has an incubation period of four to 14 days. Most infections are mild, with either no apparent symptoms or mild fever and headache. Gastrointestinal symptoms can be prominent in children. Severe disease occurs in about one in 100 to one in 250 infections, with children and older people being at higher risk. In endemic countries, most adults have developed natural immunity after childhood infection.
Severe disease is characterised by rapid onset of high fevers and severe headache with associated neck stiffness. This can progress to neurological deficits, including disorientation, seizures and paralysis. Onset of coma is often a terminal phase of the illness, with case fatality rates as high as 30%. Of those who survive, 20 to 30% suffer permanent intellectual, behavioural or neurological sequelae.
As the initial symptoms of JE are nonspecific, a high degree of clinical suspicion needs to be maintained. Attention needs to be paid to possible risk factors, such as working at a piggery or exposure to mosquitoes. Vaccination status should be determined. Differential diagnoses to consider include bacterial causes of meningitis (such as Neisseria meningitidis), other viral causes of meningitis and encephalitis (such as herpes simplex virus and other flaviviruses), along with non-infectious causes of encephalopathy (such as vascular insults, toxic and metabolic causes, epilepsy and trauma).
Management
The initial assessment of someone presenting with fevers, headache and confusion is to stabilise the patient and determine whether immediate transfer to hospital is indicated. If possible, epidemiological risk factors for JE should be confirmed. Life-threatening differential diagnoses, such as bacterial meningitis, need to be considered and treatment initiated if appropriate. Clinical examination findings such as a reduced Glasgow Coma Scale (GCS) score, hypotension, neck stiffness or a non-blanching rash (more in keeping with severe bacterial sepsis) should prompt emergency department referral. Investigations to assess for infective causes and complications should be done, including a full blood count measurement of electrolytes, creatinine and
C-reactive protein and blood cultures.
Diagnosis
Diagnosis of JE can be made by serology but usually involves sampling of cerebrospinal fluid (CSF) via a lumbar puncture. Many laboratories list JE virus serology as ‘arbovirus’ or ‘flavivirus’ serology. Cross-reactivity is high, so confirmatory testing in a reference laboratory is often performed. Serum collected within 10 days of illness may not have detectable IgM levels, highlighting the need to repeat a convalescent sample 10 to 14 days later. PCR testing can be done on serum and urine samples (2 to 5 mL from a sterile container) but has relatively poor sensitivity.
CSF is the preferred sample for diagnosis; JE virus IgM antibodies are usually detectable three to eight days after the onset of illness. Antibodies can persist for 30 to 90 days, and sometimes longer, so occasionally may represent past infection or recent vaccination. PCR testing of CSF is highly specific but unfortunately less sensitive (with only about 25% of cases being positive). PCR testing needs to be requested early in the disease course, in the first three to five days, to increase diagnostic yield.
Other investigations to help support or exclude the diagnosis of JE include CSF glucose, protein, microscopy, culture and sensitivity; PCR testing for specific pathogens (or multiplex assays); and brain imaging, such as MRI. It is also important to indicate that JE is suspected as this will help guide the diagnostic work-up for the laboratory. JE virus is not a target in most multiplex PCR assays.
Treatment
There is no specific therapy for JE; however, supportive therapy includes intravenous fluids and antipyretics. It is reasonable to offer therapy for viral and bacterial causes of central nervous system infection; aciclovir will treat herpes simplex virus encephalitis and empiric antibiotics for bacterial meningitis can be administered (as per local guidelines or Australian Therapeutic Guidelines), while awaiting investigation results.
When to refer
A patient with suspected JE and no clear alternative cause for their symptoms should be discussed with an infectious diseases physician. Any patient with a reduced GCS score, focal neurological signs, unstable observations or who cannot be adequately monitored for deterioration should be referred immediately to hospital for assessment.
Conclusion
JE is a rare but potentially fatal cause of viral encephalitis. The recent rise in cases in Australia is likely a result of climate change as well as the La Niña phenomenon. It is important to understand the complex JE virus life cycle to provide appropriate counselling on avoiding vector exposure, as well as to offer vaccination to high-risk individuals. Furthermore, increased awareness is important to ensure rapid and effective diagnosis with timely involvement of the local infectious diseases service. Local public health units should be immediately notified of any suspected or confirmed cases of JE. MT
COMPETING INTERESTS: None.