Anxiety disorders in children and adolescents

Dr Sicouri is a Senior Research Associate and Clinical Psychologist at the Black Dog Institute, Faculty of Medicine and School of Psychology, UNSW, Sydney.
Dr Perkes is a Senior Lecturer in the School of Psychiatry, School of Women’s and Children’s Health and School of Psychology, UNSW, Sydney; and a Child and Adolescent Psychiatrist in the Department of Psychological Medicine, Sydney Children’s Hospital Network, Sydney.
Professor Hudson is Director of Research and Professor of Clinical Psychology at the Black Dog Institute, Faculty of Medicine and School of Psychology, UNSW, Sydney, NSW.
Child mental health
Adolescent mental health

Anxiety disorders are highly prevalent in children and adolescents and GPs play an important role in identifying and initiating management of such patients. Clinical presentations and the extent of anxiety can be successfully measured using reliable validated questionnaires, such as the Revised Child Anxiety and Depression Scale. Cognitive behavioural therapy is the first-line treatment, with the goal of remission and functional improvement.
- Anxiety disorders in children and adolescents are common and disabling, but often under-recognised and poorly treated.
- Fears and worries are common and developmentally normal in children.
- Duration, distress and impairment are the markers of clinical threshold.
- Anxiety disorders often co-occur with other conditions, and these should be routinely screened for.
- Self-reported or parent-reported measures of symptoms and function enable detection and monitoring.
- Cognitive behavioural therapy (CBT) is the first-line treatment for anxiety disorders, with the goal of sustained remission or functional improvement.
- Exposure is the active ingredient in CBT and referrals should be made to professionals who deliver exposure-based treatment.
Anxiety lies on a spectrum that runs from normal worry to transient anxiety, through to severe and disabling symptoms.1 Normal anxiety does not interfere in functioning and can be helpful, for example, by motivating a child to work towards a goal or avoiding a potential threat. The fears of children and adolescents with anxiety disorders differ from normative worries in that anxiety disorder symptoms are persistent and associated with marked distress in addition to avoidance of triggering situations. This all amounts to substantial disruption to everyday life. Fortunately, cognitive behavioural therapy (CBT) is effective in treating anxiety disorders. GPs are well placed to help with the early detection and management of anxiety disorders in children and adolescents.
Anxiety disorders are estimated to occur in 7% of children and adolescents in Australia within a 12-month period.2 Separation anxiety, specific phobia, social phobia and generalised anxiety are the most prevalent anxiety disorders. Typically, anxiety disorders are found to be more common in girls than boys.3 The presence of one anxiety disorder predicts the co-occurrence of other anxiety disorders, major depressive disorder, attention-deficit hyperactivity disorder and oppositional defiance disorder.2,4,5 Anxiety disorders are associated with significant emotional and financial cost to individuals, their families and wider society.2,6,7 This includes an average of three weeks of missed school per year, a sixfold increase in the likelihood of a suicide attempt and later substance and alcohol abuse.8,9 Anxiety disorders in childhood can persist into adulthood if left untreated.10
Assessment
Clinical presentation
Children and adolescents experience seven types of anxiety disorders: separation anxiety, specific phobia, social anxiety generalised anxiety, selective mutism, agoraphobia and panic disorder. Clinical features common to all these conditions involve excessive fear and related behavioural disturbances, particularly avoidance or safety behaviours (i.e. behaviours to prevent the feared situation from coming true). However, these diagnoses are differentiated by the content of the fear and developmental characteristics (Table 1). Obsessive compulsive disorder (OCD) and post-traumatic stress disorder (PTSD) are no longer technically classified as anxiety disorders.11
{kind=link}
Children may also express feelings of anxiety through crying, tantrums or freezing. Physical symptoms may also be present – particularly in anticipation of the feared situation – and include muscle tension, stomach ache, loss of appetite, headache, restlessness or insomnia. Young children will often report somatic symptoms rather than verbalising their worry, which can lead to challenges and delays in detecting an anxiety disorder.
Developmental considerations
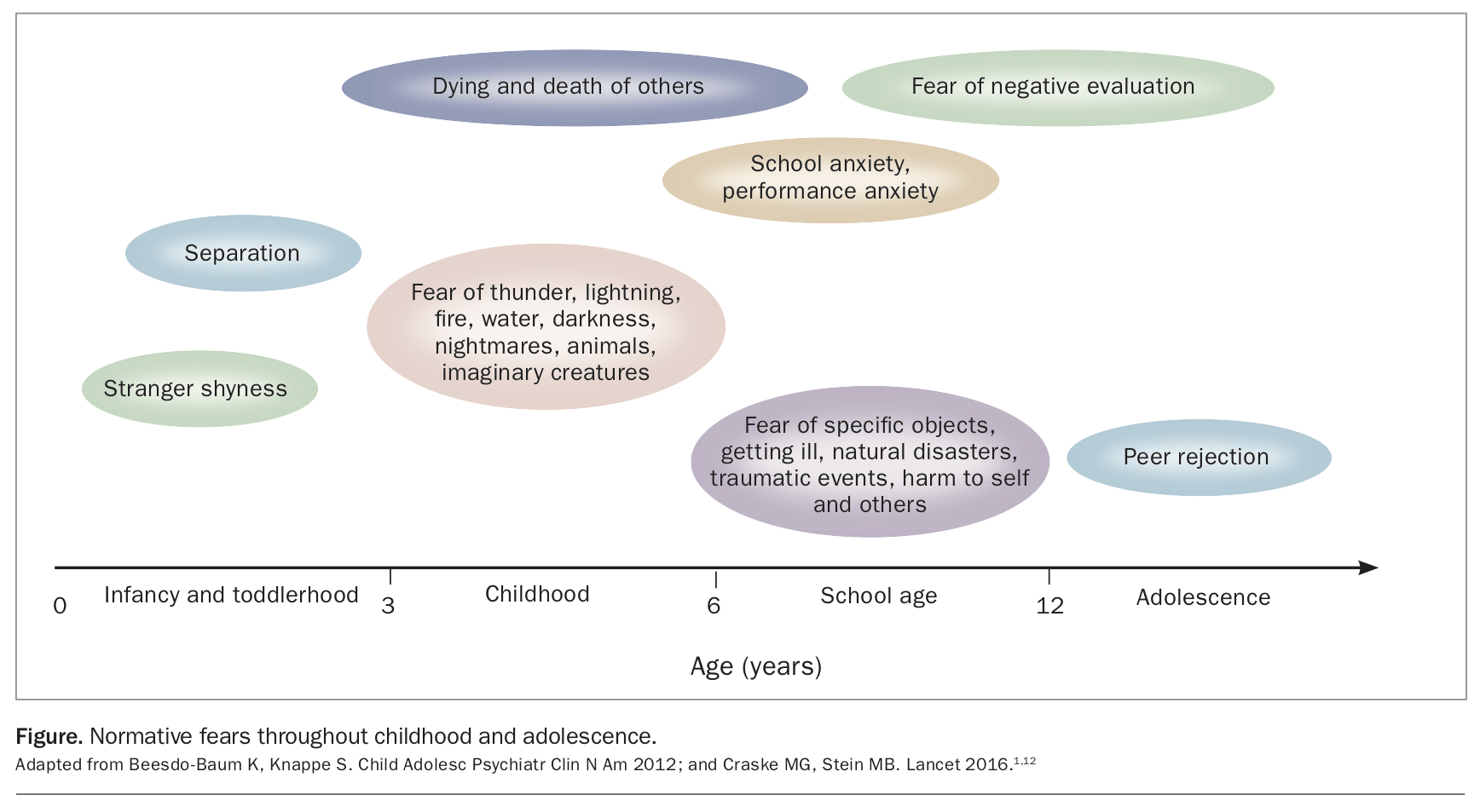
Fears and worries are developmentally normal (Figure), and the clinical threshold can be elusive.1,12 Separation anxiety typically begins in the preschool years, when many children are clingy when separating from caregivers as an adaptive formation of emotional bonds. Similarly, social anxiety often presents in late childhood or early adolescence alongside the typical increase in social awareness, independence and establishment of new peer groups. Generalised anxiety tends to emerge in later adolescence and into early adulthood as independence and general life pressures increase.
{kind=link}
Attending to the following transdiagnostic markers of pathology can help to identify an anxiety disorder (Table 2):
{kind=link}
- duration of anxiety – typically lasting at least six months
- level of distress – significantly greater than other children their own age or out of proportion to the fear
- level of impairment – interferes significantly in the child’s and/or family’s everyday functioning.
Obtaining an anxiety diagnosis has the benefit of guiding the child towards suitable treatment and may help to reduce stigma associated with anxiety symptoms.
Identification
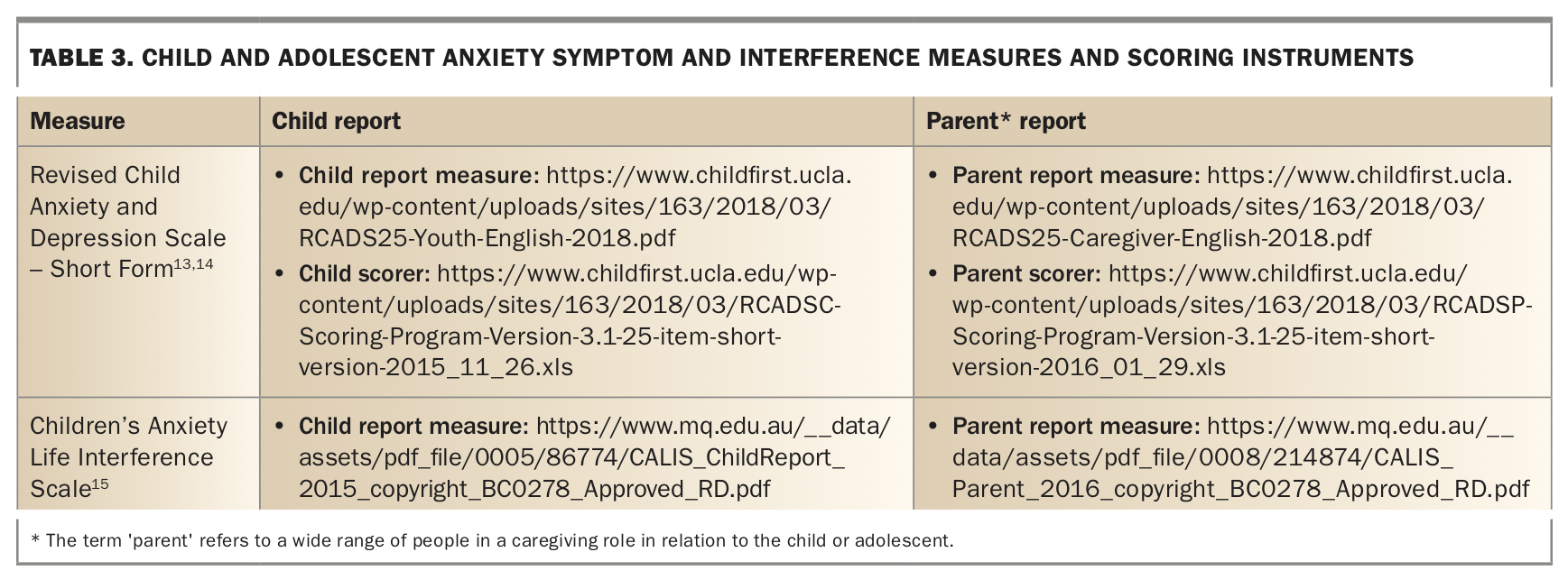
Psychometrically reliable and valid questionnaires that measure symptoms and impact on functioning can be used to screen for and assess treatment response in anxiety disorders. Use of both parent or caregiver and child report measures enables a comprehensive understanding of the child’s symptoms. Obtaining a self-report for older children and adolescents is essential given the internalising nature of symptoms.
The Revised Child Anxiety and Depression Scale – Short Version is a 25-item tool validated to assess for symptoms of both anxiety (15 items) and depression (10 items) in children and adolescents aged 8 to 18 years.13,14 Each item is scored a value between 0 and 3 (where 0 = never, 1 = sometimes, 2 = often and 3 = always). There are parent-report and self-report versions. The scores for the items measuring anxiety are summed and converted to T-scores using available online scoring programs (Table 3).13-15 A T-score of 65 or above (equivalent to 1.5 standard deviations above the mean) indicates the need for referral of the patient for a more detailed assessment.
{kind=link}
Diagnosis
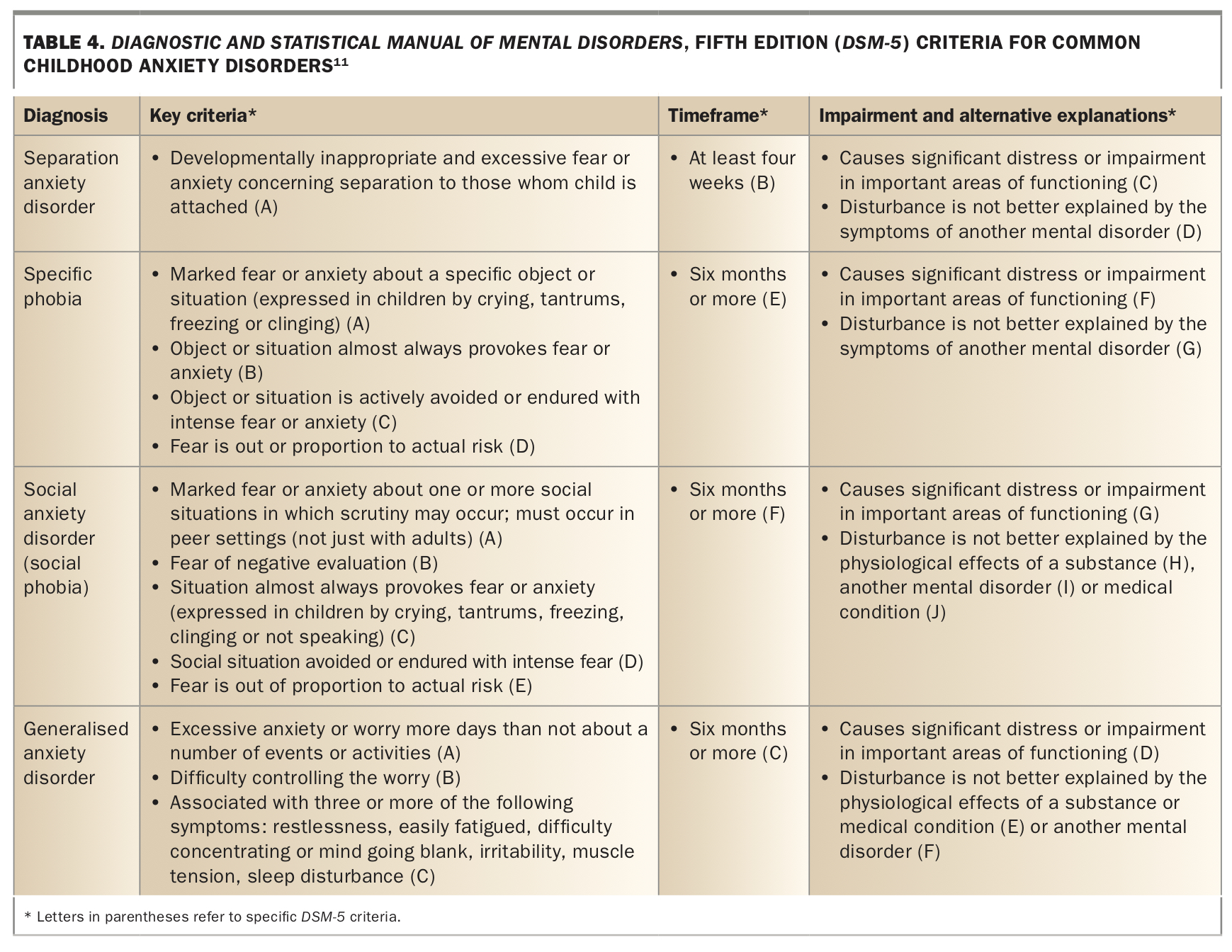
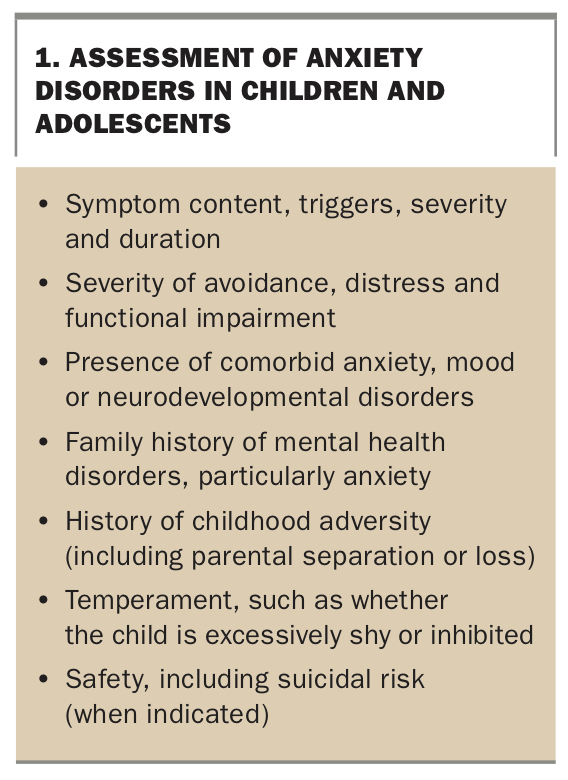
A standardised diagnostic interview, such as the Anxiety Disorders Interview Schedule for children and parents (ADIS-C/P), is the gold-standard method for assessing anxiety disorders in children and adolescents. However, although standardised assessments are commonly used in research trials, they are rarely used in clinical settings. Pragmatically, a diagnosis is usually made by clinical history and assessment to screen for symptoms aligning with the Diagnostic and Statistical Manual of Mental Disorders, 5th ed (DSM-5) criteria (Table 4), while ruling out differential diagnoses (Table 1).11 For diagnosis under a Mental Health Treatment Plan (MHTP), International Classification of Primary Care (ICPC) codes are used. Assessment of suicidal and self-harm risk might also be warranted, particularly for adolescents. Factors to consider as part of a comprehensive assessment of anxiety disorders in children and adolescents are listed in Box 1. Making time to listen to the young person and their parents is important to provide them with insight into their experiences and differentiate between symptoms.
{kind=link}
{kind=link}
It can sometimes be helpful to normalise symptoms and screen for anxiety subtypes before probing further, by asking questions such as ‘Some kids (teenagers) feel really scared and uncomfortable in situations with other people, so scared and uncomfortable that they might want to stay away from these places. Is this something that happens to you?’. The assessment should be conducted with both the child and the parents to give a richer understanding of the child’s symptoms. Offering to conduct some of the assessment with the child separately from the parents may also be important, particularly for older children and adolescents, to provide them with the opportunity to disclose symptoms that they may be reluctant to share in front of their parents, such as worries about their family.
Comorbidity
Comorbidities are common in people with anxiety disorders and should routinely be screened for. Major depressive disorder often co-occurs with anxiety disorders, particularly in adolescents.16 Anxiety disorders also commonly co-occur with neurodevelopmental conditions such as attention deficit hyperactivity disorder, OCD and autism spectrum disorder.17 PTSD symptoms, such as avoidance, can appear quite similar to anxiety symptoms. Children who experience a significant adverse life event (e.g. child maltreatment) are at greater risk of developing both PTSD and an anxiety disorder.18
Family history
Anxiety runs in families. Getting a family history informs the genetic risk of anxiety – which is increased by having a parent with an anxiety disorder – and psychosocial context, such as parenting behaviours that accommodate avoidance or anxious modelling.18,19
Management
Cognitive behavioural therapy
CBT is the recommended first-line treatment for children and adolescents with anxiety disorders.20 It is the only evidence-based nonpharmacological treatment that has been found to be effective, with low attrition rates and high rates of response and remission (50%) when compared with patients on waiting lists for CBT and those on no treatment.21 Comorbidity only accounts for modest variability on remission in anxiety diagnoses across CBT studies.22
CBT helps children and young people with anxiety disorders to recognise and modify unhelpful thoughts, emotions and behaviours associated with their anxiety, and helps to maintain these changes. CBT is typically applied across a range of anxiety disorders, rather than being disorder-specific, targeting psychological processes that are shared across different anxiety problems, such as cognitive bias and avoidance. It is a skills-based approach and includes psychoeducation, cognitive restructuring, exposure, problem solving and relapse prevention. Benefiting from CBT requires the young person to practice their skills regularly.
Exposure (i.e. facing anxiety-provoking situations) is the active ingredient of CBT and should be included in all standard CBT practices for young people with anxiety disorders.23 The goal of exposure is to overcome avoidance. Avoidance maintains the child’s anxiety because the child is prevented from learning accurate information about the likelihood of something bad or dangerous happening and their ability to cope. Exposure serves to strengthen new memories about the feared event and weaken old memories. Exposure in CBT typically involves:
- understanding that avoidance serves to maintain anxiety and that exposure serves to reduce avoidance
- developing a hierarchy of fears rated from the least to the most fear-inducing
- conducting exposure tasks (in vivo, imaginal or parent-led) within and between sessions
- reducing family accommodation of avoidance.
Cognitive restructuring, which involves identifying and modifying anxious thoughts, can support exposure effectively.24 There is less evidence for the efficacy of other anxiety management techniques, such as relaxation and problem-solving.25,26 There is no evidence to suggest that other nonpharmacological treatments for youth anxiety, such as mindfulness-based interventions, are beneficial for anxiety remission.27
Parents are usually included in CBT sessions for children. They may also be involved in treatment for adolescents, depending on their role in the child’s anxiety and the young person’s preference. If parents play a role in maintaining anxiety, such as through accommodating avoidance or modelling, then involving parents ensures that these factors can be addressed and monitored to avoid impacting on the child’s treatment success.
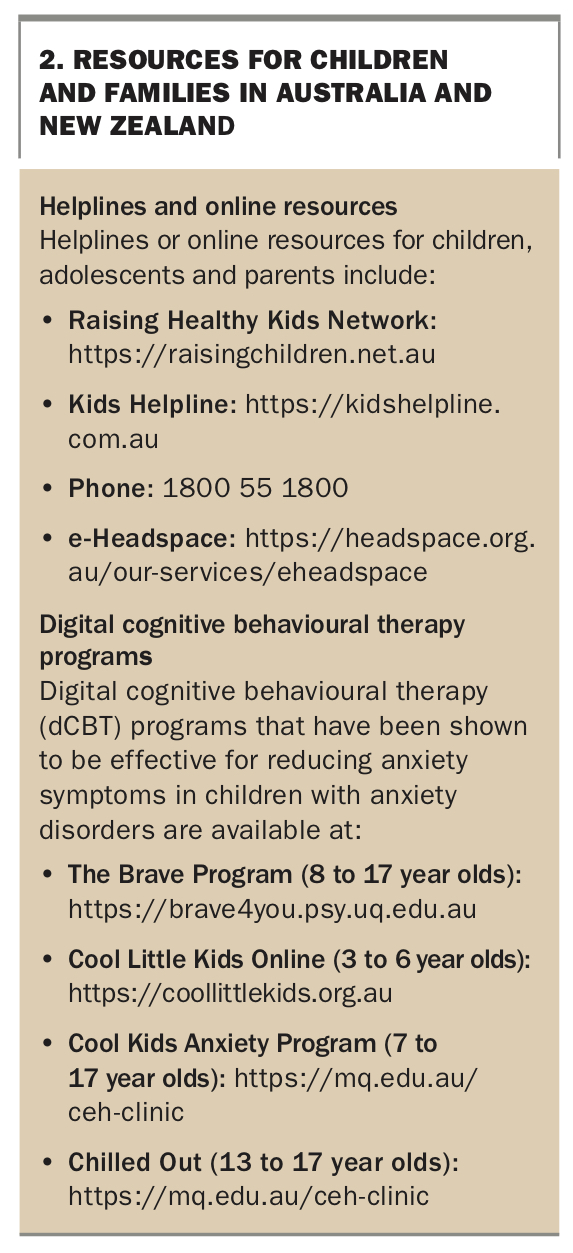
CBT is typically delivered in around 10 weekly face-to-face (individual or group) one-hour sessions with a mental health professional, such as a psychologist. However, given the difficulties in accessing face-to-face treatment, including long waitlists and financial and time barriers, more accessible modes of treatment could be considered. Emerging evidence supports the efficacy of low-intensity CBT options, such as digital CBT, in preventing and treating anxiety disorders in young people.28-30 These options do not need a referral to a psychologist and can be accessed directly by families. However, to date, no digital CBT program has led to remission of anxiety disorders in a youth population. Selecting the appropriate treatment format to deliver CBT needs to be based on a balance between evidence of efficacy, accessibility, patient preference, cost, symptom severity and comorbidity. Useful resources for children with anxiety and their family, including digital CBT programs, are listed in Box 2.
{kind=link}
Relevant stakeholders
Anxiety symptoms are increasing in children and adolescents in Australia.31 The approach to treatment is a shared community responsibility, and an integrated response from school, family and medical professionals that encourages the child to approach their feared situations is a crucial part of intervention. Yet the likelihood of children with anxiety receiving evidence-based care, particularly exposure-based therapy, in the community is low.32 Choosing professionals who deliver evidence- and exposure-based care is important.
Children may exhibit anxiety symptoms close to the start of exams, and special provisions are often needed. Children or families needing a request for special provisions often seek input from a GP. This represents a critical point for intervention. However, if the anxiety emerges earlier then this provides an opportunity to ensure that the child receives evidence-based care that could remove the need for the provisions. In contrast to the goals of treatment, granting special provisions can send the message to the child that they are unable to cope, that anxiety cannot be managed and avoidance of the situation is the best option. However, if special provisions are the only option that allow the child to sit the exam, this is an important step as they move towards approach behaviours.
Pharmacotherapy
There is evidence for the use of selective serotonin reuptake inhibitors (SSRIs) in treating anxiety disorders in children and adolescents.33 However, this evidence is limited in strength relative to similar conditions such as paediatric OCD.34 Given this limited evidence, there is a concerning trend of psychotropics being prescribed to children and adolescents with anxiety disorders. Antipsychotic medications, such as quetiapine in particular, carry substantive cardiometabolic risks relative to the lack of proven benefit. Use of SSRIs is associated with osteoporosis, a key concern in young women during their years of bone density accrual, although this is an uncommon adverse effect.35 Therefore, we suggest that, if CBT has achieved only a limited response, the patient be referred to a specialist, such as a developmental paediatrician or child and adolescent psychiatrist, for pharmacotherapy considerations.
Referral
Referrals to a mental health professional can be made via public services, such as state-funded child and youth mental health service, or private services. If referring to a private service, children and adolescents are eligible for a MHTP and 10 sessions per calendar year with a psychologist or mental health clinician (telehealth or face-to-face) subsidised by Medicare. GPs are required to conduct a review after six sessions. The Medicare Benefit Schedule criteria for a MHTP is available online (http://www9.health.gov.au/mbs/fullDisplay.cfm?type=item&q=2715). A suggested template for a MHTP for children and adolescents is also available online (https://gplearning.racgp.org.au/content/Headspace/Part1/GPMHTP_child_adol.pdf).
When referring a patient to a specialist mental health professional, encourage the use of evidence-based care with a particular focus on exposure. Specify the content of the child’s anxiety and provide information about avoidance, impact and suspected diagnoses. If known, provide additional information about the family context (e.g. parental mental health), adverse life events (e.g. parental separation) or child trauma history.
Follow up
The effectiveness of CBT should be reviewed after six sessions of regular (preferably weekly) CBT or four to six weeks of pharmacotherapy. Information about graded exposure to feared situations should be checked. Self- or parent-report measures can be used to monitor change and are often helpful for both patients (including parents) and GPs (Table 3).
Education
It can be helpful to let the child and family know that fear and worries are a normal part of development. This information is beneficial because the child and family often feel that what they are experiencing is unique to them. If you suspect a diagnosis of anxiety, let the child and parent know that in most cases, anxiety is adaptive and comes and goes; however, can be problematic when it stops the child doing things they want to do, interferes in their friendships, school or family life or causes significant distress. Basic education about the role of avoidance in reinforcing the anxiety cycle might also be helpful. Promoting healthy lifestyle behaviours, such as good sleep, regular exercise and healthy eating, is also important. Reliable, plain language resources for patients on anxiety and healthy development are listed in Box 2.
Conclusion
Anxiety is a normal developmental response throughout childhood and adolescence; however, recognising the threshold at which it interferes with daily life is challenging. Fortunately, there are reliable ways to assess for and manage anxiety disorders. Duration, level of distress and extent of impairment induced by anxiety are key transdiagnostic markers that can help identify anxiety disorders, and diagnosis is typically made via a clinical history and differential diagnoses against standard criteria. CBT, with a focus on exposure, is an effective first-line treatment option. Patient follow up and education, including the role of accommodating avoidance or modelling in reinforcing anxiety behaviours, are mainstays of long-term management. MT
COMPETING INTERESTS: None.