Chronic hypertension and pregnancy – emphasising longitudinal care to improve maternal and fetal health

Dr Brumby is a Nephrologist at Eastern Health, Melbourne; and Adjunct Senior Lecturer, Eastern Health Clinical School, Monash University, Melbourne.
Professor McMahon is a Nephrologist and Obstetric Medicine Physician at Eastern Health; and Professor at Eastern Health Clinical School, Monash University, Melbourne, Vic.
Hypertension in pregnancy
Health problems in pregnancy

Pregnant women with chronic hypertension are at high risk of adverse outcomes, many of which are potentially preventable. GPs play a crucial role in ensuring women with chronic hypertension are appropriately managed before, during and after pregnancy to minimise complications to mother and baby.
- Common risk factors for chronic hypertension in young women include obesity, family history, kidney disease and a past history of hypertension in pregnancy or pre-eclampsia.
- Chronic hypertension affects around 0.6 to 3% of pregnancies in Australia; a quarter of these women will experience superimposed pre-eclampsia.
- Chronic maternal hypertension is defined as either a previous documented history of or treatment for hypertension outside pregnancy or, alternatively, a blood pressure of 140/90mmHg or higher on at least two occasions before 20 weeks’ gestation.
- Screening for secondary causes of hypertension is indicated in women of childbearing age with chronic hypertension. In pregnancy, screening can usually be deferred until postpartum.
- Blood pressure targets in pregnancy are now similar to those in the general population, and home blood pressure monitoring can be a valuable tool to enhance control and improve patient engagement.
- Methyldopa and labetalol continue to be the cornerstones of safe and effective blood pressure management in pregnancy.
Chronic maternal hypertension affects about 0.6 to 3% of pregnancies in Australia, although this is likely an underestimate.1,2 Globally, the incidence of chronic hypertension in pregnant women is rising, with increasing maternal age at delivery and obesity rates likely contributing factors. Chronic maternal hypertension is a risk factor for significant maternal and perinatal morbidity, including preterm birth, pre-eclampsia, caesarean section, low birthweight and perinatal death. The incidence of superimposed pre-eclampsia in particular is 25.9% compared with significantly lower rates (3 to 5%) in normotensive women.3
For some women, the diagnosis of chronic hypertension is made preconception. This allows for timely pre-pregnancy counselling and planning to improve antenatal care and optimise outcomes. However, many women are initially identified as hypertensive in the first half of pregnancy (before 20 weeks’ gestation), highlighting the importance of blood pressure screening in early pregnancy consultations. Essential hypertension remains the most common cause of hypertension in younger women. By definition, essential hypertension requires investigation and exclusion of secondary causes that may be done preconception but, in most cases, can be safely delayed until postpartum. Secondary causes are disproportionately represented in women of childbearing age and are estimated to account for more than 15% of cases.4
Most preconception, first-trimester and postpartum healthcare interactions in women with chronic hypertension who are pregnant or planning pregnancy are with their GP. Thus, GPs play a crucial role in longitudinal care and ensuring that opportunities for improving pregnancy outcomes and long-term health in young mothers are not missed. This review highlights important issues and provides guidance for GPs on optimal management of this important group of patients.
Chronic maternal hypertension and adverse pregnancy outcomes
Pregnancies affected by chronic maternal hypertension have increased rates of maternal and fetal morbidity. Although much of the morbidity such as preterm birth is attributable to high rates of superimposed pre-eclampsia, other adverse outcomes, such as placental abruption or low birthweight, appear to be independently linked to chronic maternal hypertension.5 Chronic hypertension often also coexists with other common comorbid conditions or lifestyle risk factors in the pregnant population including diabetes, obesity, kidney disease and smoking. These additional factors may further increase risk of pregnancy complications. Importantly, many of these factors are potentially modifiable, and so pregnancy-related complications can be minimised with good preconception management of chronic disease, together with optimisation of lifestyle factors.
There is now emerging evidence that good blood pressure control in women with chronic hypertension, either preconception or in the first trimester, is associated with improved pregnancy outcomes such as higher birthweight and lower risk of pre-eclampsia.6 Good quality randomised trials show that low-dose aspirin therapy initiated at the end of the first trimester, and calcium supplementation in those with a low-calcium diet, lower pre-eclampsia risk and are regarded as the standard of care.7
Causes of chronic hypertension in young women
A number of chronic health conditions, including obesity, lifestyle factors and secondary causes of hypertension such as endocrine disorders and renal disease, contribute to hypertension among women of childbearing age. Importantly, many of these conditions are potentially modifiable to improve blood pressure control before, during or after pregnancy.
As discussed, screening for secondary causes of hypertension can occur preconception or be safely be delayed until postpartum in most cases. Important clinical indicators requiring investigation for secondary causes during pregnancy include:
- difficult-to-control blood pressure requiring multiple antihypertensive agents in the first half of pregnancy
- new-onset moderate to severe hypertension (150/100 to above 160/110 mmHg), or persistent severe hypertension (above 160/110 mmHg) if concurrent pre-eclampsia has been excluded
- evidence of new or worsening renal dysfunction or other end-organ involvement.
Secondary causes of hypertension
Chronic kidney disease
Kidney disease is the most common cause of secondary hypertension in young women.8 Common renal conditions in this population include reflux nephropathy and other congenital abnormalities, glomerulonephritis and autosomal dominant polycystic kidney disease. Clinical indicators include an elevated serum creatinine level or reduced estimated glomerular filtration rate, proteinuria, albuminuria or haematuria on urine microscopy, and abnormal renal imaging. Importantly, the combination of renal disease with chronic hypertension compounds the risk of adverse pregnancy outcomes such as preterm birth and pre-eclampsia.
Renal artery stenosis
Renal artery stenosis is relatively uncommon and usually due to fibromuscular dysplasia. Screening investigations could include a Doppler kidney ultrasound examination. Diagnostic tests such as angiography, CT renal angiography or MRI can usually be deferred until postpartum.
Obstructive sleep apnoea
Obstructive sleep apnoea (OSA) is increasingly recognised as an important additional risk factor for pre-eclampsia and can occur with or without obesity being present. A history of snoring or disrupted night-time breathing is suggestive of OSA. Referral for sleep studies and continuous positive airway pressure therapy is advisable, urgently if OSA is diagnosed antenatally.
Endocrine disorders
Possible endocrine causes of hypertension include hypo- or hyperthyroidism, hyperaldosteronism, Cushing’s syndrome and phaeochromocytoma. Thyroid function tests can easily be preformed during pregnancy; however, measurement of serum aldosterone and renin levels should be delayed until postpartum because of physiological hormonal changes in pregnancy.
Phaeochromocytoma is rare. Nonetheless, it is a potentially lethal condition for both mother and fetus during pregnancy, especially if it is not considered, diagnosed and appropriately managed. Clinical features include severe, resistant or very labile hypertension associated with tachycardia. Plasma-free metanephrine and 24-hour urinary catecholamine levels can be helpful. If clinically suspected, early expert consultation is advised.
Other systemic diseases associated with hypertension
Pre-existing chronic conditions such as type 1 and type 2 diabetes mellitus, or autoimmune conditions such as rheumatoid arthritis or systemic lupus erythematosus (SLE) may also be associated with chronic hypertension. Aetiology of hypertension in these conditions may be due to renal involvement or other mechanisms such as pharmacotherapy (e.g. prednisolone).
Other important causes of hypertension
Obesity
Obesity is a common and potentially modifiable cause of hypertension in young women. Currently, 37% of Australian women aged 25 to 44 years have obesity, and the risk of hypertension is two- to six-fold higher in women who are overweight or obese compared with those of normal body weight.9-11 Lifestyle modification to lower body mass or limit gestational weight gain have been shown to improve blood pressure control and lower the risk of pregnancy-related complications, including pre-eclampsia.12
White coat hypertension
‘White coat’ hypertension is defined as a blood pressure above 140/90 mmHg in healthcare settings, but a normal blood pressure when measured elsewhere, such as at home. Diagnosis requires either a 24-hour ambulatory blood pressure test or home blood pressure monitoring. Although not technically a cause of chronic hypertension, white coat hypertension is often encountered in clinical practice among younger women and is highly relevant to pregnancy. White coat hypertension either before or during pregnancy is a known risk factor for developing pre-eclampsia or sustained gestational hypertension, and affected women should receive closer monitoring accordingly.13
Medications and other drugs
Some medications, such as antidepressants, prednisolone and tacrolimus, can contribute to hypertension. Additionally, over-the-counter supplements, including nicotine replacement, Ginseng, liquorice and St John’s wort, and illicit drugs such as amphetamines and cocaine can also increase blood pressure.14
Preconception counselling and pregnancy planning
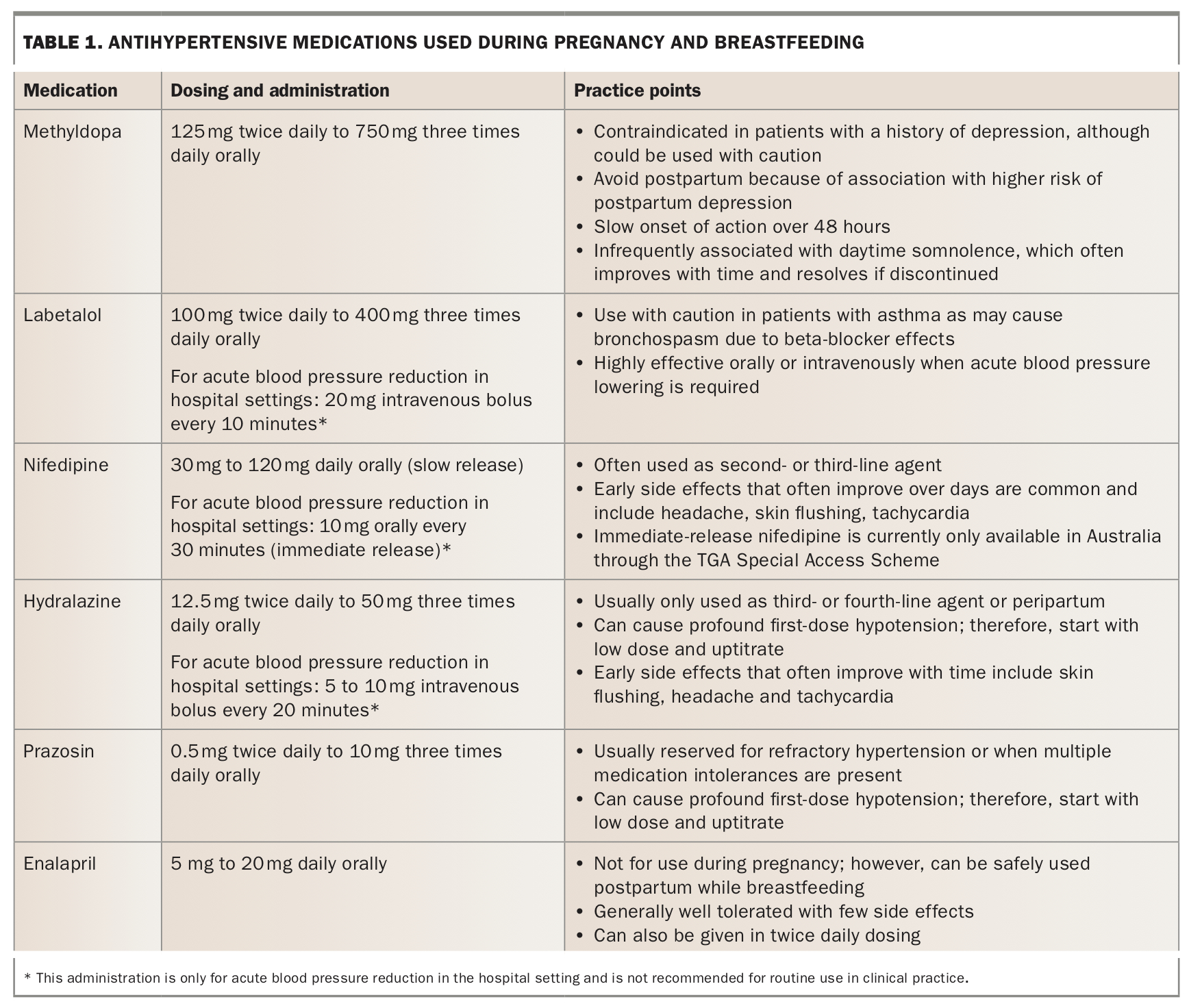
Management of women with chronic hypertension who are planning pregnancy begins preconception. Blood pressure management should be optimised using pregnancy-safe antihypertensives, aiming for an office blood pressure below 140/90 mmHg or an average home blood pressure below 135/85 mmHg (Table 1). Preconception counselling should involve a discussion about pregnancy risks, planning blood pressure monitoring and management in early pregnancy, and discussion about using aspirin and other therapies to reduce the risk of pre-eclampsia. Investigation for secondary causes of hypertension may also occur at this time.
{kind=link}
Women whose blood pressure is controlled with nonpregnancy-safe antihypertensives (such as ACE inhibitors or diuretics) or who need them specifically for additional indications (such as proteinuria or cardiac issues) can often be given an individualised plan to continue these medications until conception. These medications are best stopped by six weeks of pregnancy (i.e. four weeks after conception or two weeks after a missed period) to avoid harmful fetal exposure. A regular menstrual cycle is highly advantageous in these circumstances.
Pregnant women with chronic hypertension have a number of risk factors for a poorer prognosis. These include:
- a history of longstanding (e.g. more than five years) or difficult-to-control hypertension requiring multiple antihypertensive medications
- secondary hypertension
- a history of pre-eclampsia, particularly preterm pre-eclampsia
- pre-existing chronic kidney disease.
Women with one or more poor prognostic factors may benefit from preconception counselling and optimisation, or early pregnancy assessment by either an obstetric medicine physician or maternal fetal medicine specialist. Women with underlying renal disease should consult a nephrologist to discuss the additional potential for permanent deterioration in renal function during or after pregnancy.
Management of chronic hypertension diagnosed in early pregnancy
Chronic hypertension is identified in some women for the first time in pregnancy. Criteria for a diagnosis are an elevated blood pressure of 140/90 mmHg or above on at least two separate occasions before 20 weeks’ gestation. Often, clinical indicators are present to suggest undiagnosed chronic hypertension. These include previous ‘borderline’ or oestrogen-sensitive hypertension, a history of remote antihypertensive use, chronic kidney disease, a history of gestational hypertension or pre-eclampsia and having a low birthweight baby. For women with clinical indicators or risk factors for hypertension, it is usually appropriate to start antihypertensive medication and pre-eclampsia prophylaxis (low-dose aspirin) when hypertension is detected. For women without risk factors, promptly excluding white coat hypertension by either 24-hour ambulatory blood pressure assessment or home blood pressure monitoring before initiating therapy is suggested.
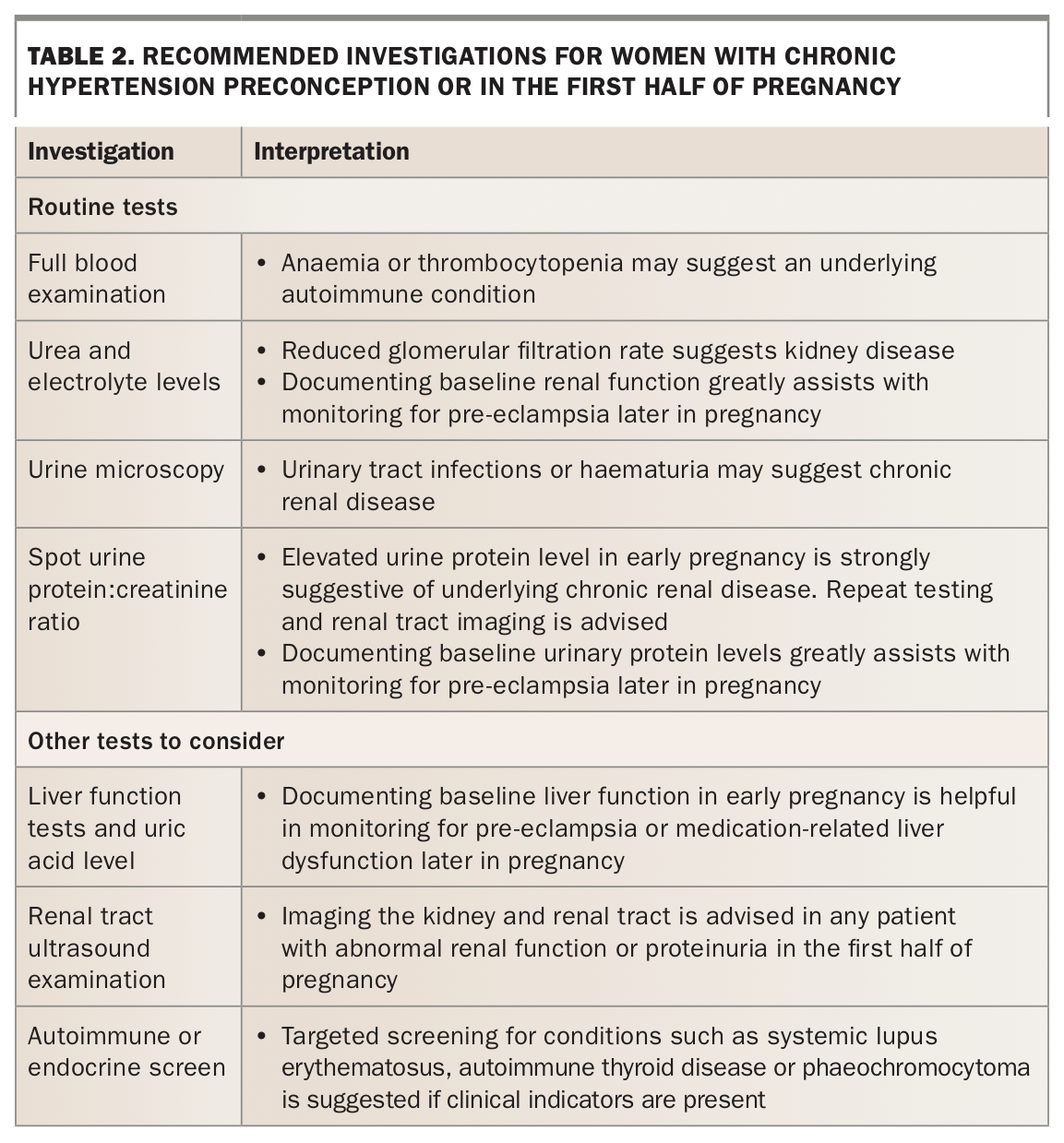
In addition to considering antihypertensive therapy, a detailed history, examination and baseline investigations are recommended. Determining any factors on history or examination to suggest secondary hypertension is important and frequently fruitful. Even for women without features of secondary hypertension, it is advisable to obtain a number of simple baseline investigations to help guide management for the remainder of their pregnancy (Table 2).
{kind=link}
Antenatal care and antihypertensive therapy
Care pathways
Women with chronic hypertension should be flagged as a ‘higher risk’ pregnancy. Depending on local service availability and expertise, these women may benefit from both multidisciplinary care and care by clinicians experienced in managing hypertension in pregnancy.
Pre-eclampsia prophylaxis
Women with chronic hypertension are at high risk of pre-eclampsia, and both local and international guidelines recommend prophylaxis unless contraindications are present. Both low-dose aspirin and oral calcium supplementation for women with a low dietary intake of calcium are considered safe and effective. Aspirin 100 to 150 mg orally at night and calcium 1500 mg daily are recommended to be commenced, ideally before 14 weeks’ gestation; however, starting before 20 weeks’ gestation also likely has benefit. Aspirin is typically stopped at around 36 weeks’ gestation as it is most beneficial in preventing preterm pre-eclampsia and has a limited role beyond this gestation.
Blood pressure management
Blood pressure measurement can be difficult in all three trimesters for different reasons, and it is important to understand the normal pattern of blood pressure changes throughout pregnancy. In the first trimester, blood pressure often rapidly falls to below pre-pregnancy levels due to pregnancy-related hormones, such as relaxin and progesterone, and an associated reduction in peripheral vascular resistance. This often means women need to discontinue or reduce their regular antihypertensives to maintain a normal blood pressure and avoid overtreatment. Overtreatment of blood pressure in pregnancy can cause maternal fatigue and an increased risk of syncope, and has additionally been associated with risk of fetal growth restriction.15
Blood pressure in pregnancy is often lowest at around 20 weeks’ gestation and continues to rise to pre-pregnancy levels by the end of the second trimester. Antihypertensive medication will often need to be restarted or the dose increased in this context. In the third trimester, blood pressure may rise higher than pre-pregnancy levels. A sudden sustained rise in blood pressure (above 160/100 mmHg or above 140/90 mmHg with symptoms of pre-eclampsia or new proteinuria), or an increasing antihypertensive requirement at any point in pregnancy but particularly after 20 weeks’ gestation, warrants assessment for superimposed pre-eclampsia.
There is currently limited high-quality evidence guiding blood pressure targets in the first half of pregnancy; however, expert advice is to target similar levels as for nonpregnant women: initiate therapy when blood pressure is above 140/90 mmHg, titrating to a target of 110 to 140/<90 mmHg in office settings and 110 to 135/<85 mmHg in home settings. Randomised trials such as the CHAP (Chronic Hypertension and Pregnancy) study are nearing completion to confirm these recommendations.16
The CHIPS study (Control of Hypertension in Pregnancy Study) showed that reasonably tight control of diastolic blood pressure (below 85 mmHg) in the second half of pregnancy was associated with a reduced chance of severe maternal hypertension and was not associated with adverse fetal outcomes (such as fetal growth restriction) when compared with less tight blood pressure control.17 Using these data in addition to recent meta-analyses, most guidelines now suggest initiating antihypertensive therapy when blood pressure is 140/90 mmHg or higher, and titrating to a target of 110 to 140/<85 mm Hg in the second half of pregnancy.18,19
The choice of antihypertensive medication depends on individual patient factors. However, either methyldopa or labetalol remain the mainstay of therapy (Table 1).
Routine monitoring
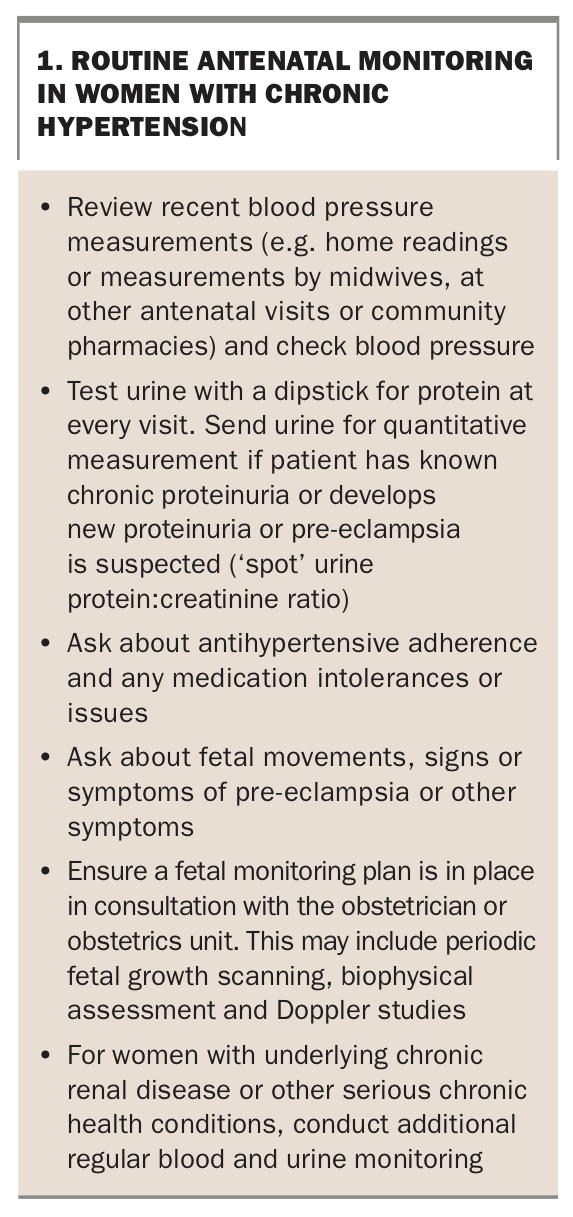
Antenatal monitoring in women with chronic hypertension involves frequent evaluation of maternal symptoms (including symptoms of pre-eclampsia), blood pressure measurement and any relevant biochemical or other tests, as well as monitoring fetal growth and wellbeing (Box 1).
{kind=link}
If not performed before pregnancy, baseline assessment of renal function and evaluation for proteinuria should be performed in all women with chronic hypertension early in the gestation. This both screens for underlying kidney disease and provides a reference point should pre-eclampsia be suspected later in pregnancy. Additional suggested baseline tests are listed in Table 2.
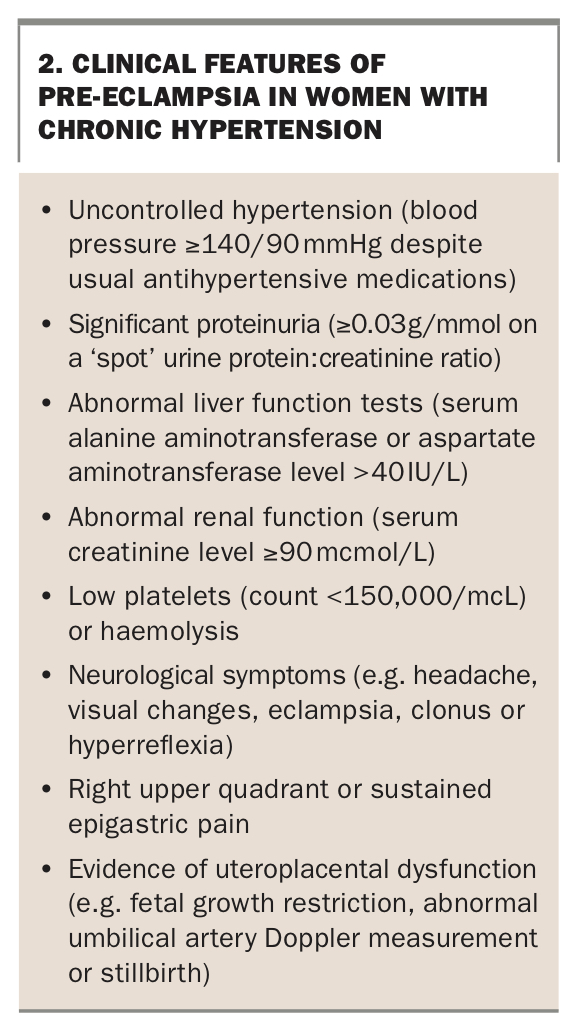
In addition to standard antenatal care, women with chronic hypertension should be asked about symptoms of pre-eclampsia at each visit after 20 weeks’ gestation. Admission to hospital or a day assessment unit is advised for women with worsening hypertension or proteinuria, or other clinical features suggesting pre-eclampsia. This enables timely assessment and management of mother and baby in an equipped facility, and allows for further discussion and planning by their care team in a safe environment. Distinctive features of pre-eclampsia in women with chronic hypertension are outlined in Box 2.
{kind=link}
The frequency and method of blood pressure monitoring requires individualisation and adjustment throughout pregnancy. Women with unstable blood pressure control and taking multiple antihypertensive medications, who are suspected of having secondary hypertension or have multiple comorbid conditions will likely need much closer monitoring than women not taking medications. Many women are able to monitor their own blood pressure at home between face-to-face appointments using a personal device. Use of an upper-arm home blood pressure device that has been validated for use in pregnancy is preferred. Periodic correlation of home blood pressure readings with doctors’ office blood pressure measurement is advised where possible. Telehealth appointments can also be an option for certain patients who are able to monitor their blood pressure at home.
Intrapartum care
Delivery should be planned at a location with adequate facilities and appropriate expertise in caring for women with hypertensive disorders. The timing and mode of delivery is determined on fetal and maternal grounds. Pregnancy should be allowed to continue to term (39 to 40 weeks’ gestation) provided maternal and fetal wellbeing is maintained. However, with singleton pregnancies, perinatal morbidity in women with chronic hypertension increases considerably from 39 weeks’ gestation compared with normotensive women. Indications for delivery in women with chronic hypertension may include superimposed pre-eclampsia, uncontrolled hypertension (with or without pre-eclampsia) or concern over fetal wellbeing. Uncontrolled hypertension typically includes repeated episodes of severe or sustained hypertension despite adequate therapy from at least three different classes of antihypertensive medications. Options for acute lowering of blood pressure are listed in Table 1.
Mode of delivery is generally pre-planned for women with chronic hypertension. In most cases, vaginal delivery is favoured unless urgent delivery via caesarean section is required because of fetal or maternal complications, including fetal distress, antepartum haemorrhage/abruption and pre-eclampsia with severe features. Regional anaesthesia is generally preferred in these situations, and can improve blood pressure control. Maternal thrombocytopaenia or the need for very urgent delivery may preclude this, necessitating general anaesthesia.
Postpartum care
Women with underlying chronic hypertension often have a stormy postpartum course. Blood pressure can be highly unstable, especially in the first few weeks after delivery. This is a normal and expected occurrence in women with chronic hypertension, either with or without superimposed pre-eclampsia. In this context, women sometimes need readmission to hospital within the first few weeks after delivery for blood pressure stabilisation or pre-eclampsia management. Importantly, red flag signs and symptoms such as elevated blood pressure with headache should raise strong suspicion of superimposed pre-eclampsia, and urgent evaluation is advised. Postepidural headaches and headache related to lactation or medications such as nifedipine are diagnoses of exclusion in this high-risk cohort.
Blood pressure management in the early postpartum period is usually initiated in hospital but often needs adjustment in the outpatient setting. An attentive and aggressive approach to treating postpartum hypertension is of particular importance to avoid serious maternal complications such as stroke and intracerebral haemorrhage. Of note, risks from overtreatment of maternal blood pressure are less serious postpartum as fetal wellbeing is no longer a consideration. Some women will need frequent clinical assessment for the first few weeks after delivery to review symptoms and adjust medications. Telehealth with home blood pressure monitoring can be a valuable tool to facilitate frequent and more timely review for suitable patients.
Enalapril is often used first-line postpartum as it is well tolerated and safe during breast-feeding. Other options include labetalol and long-acting nifedipine. Methyldopa is generally avoided postpartum because of the risk of postpartum depression as outlined in Table 1. Women who are not breastfeeding can return to their preconception antihypertensive regimen.
Postpartum women with chronic hypertension will need close follow up for at least the first year after birth as blood pressure control can change throughout the year. Previously well-controlled blood pressure can change when breastfeeding is stopped, hormonal contraceptives are restarted, weight is lost or gained, or on return to employment. Masked hypertension or secondary hypertension are important not to be missed given the long-term implications for cardiovascular health and any future pregnancies. It is also prudent to counsel about the risk of complications in any future pregnancies and the long-term cardiovascular risks related to chronic hypertension or pre-eclampsia if present. A long-term plan for blood pressure monitoring and cardiovascular risk factor screening is helpful to set patient expectations and is an almost universal guideline recommendation.
Conclusion
The prevalence of chronic hypertension in pregnancy is increasing, necessitating a good understanding of the implications for management and risk of pregnancy complications. Many of the crucial health interactions for women with chronic hypertension are provided by GPs and include preconception counselling, first trimester management and postpartum follow up.
Diagnosis and management of hypertension in young women has many important considerations. It is not uncommon for the diagnosis of hypertension to be incidental as many young women tend not to have their blood pressure routinely measured. Whether hypertension is identified before pregnancy or early in gestation, appropriate management of blood pressure and pre-eclampsia prophylaxis is indicated to reduce potential maternal and fetal morbidity. A multidisciplinary approach to antenatal care is essential to ensure the best maternal and fetal outcomes. Attentive follow up of women postpartum for 12 months by their GP will help ensure long-term maternal health and, in turn, the health of their family. MT
COMPETING INTERESTS: None.