Children with autism spectrum disorder – consultation tips for GPs

Managing children with autism spectrum disorder can be challenging, as there is a broad range of presentations and each child has a unique set of strengths and difficulties. GPs play an important role in supporting these children and their families, from identifying early red flag signs to providing ongoing care into adulthood. Building rapport and trust with patients and families using a gentle and sometimes creative approach will help to optimise care for these children.
Consulting with children is enjoyable but can be challenging. One particularly challenging group is children with autism spectrum disorder (ASD). The prevalence of ASD has increased significantly in the past 20 years, from one in 150 children in 2000 to one in 44 in 2018, according to data collected by the US-based Autism and Developmental Disabilities Monitoring Network.1 Therefore, children with ASD are now more likely to present to general practice.
The ‘spectrum’ of autism covers more than just whether symptoms are mild or severe. Every child with ASD has his or her own unique set of strengths and difficulties, communication styles, fears, sensitivities and personality. There are therefore many factors to keep in mind when interacting with children with ASD, and some situations may require creative and thoughtful approaches to optimise care for these children.
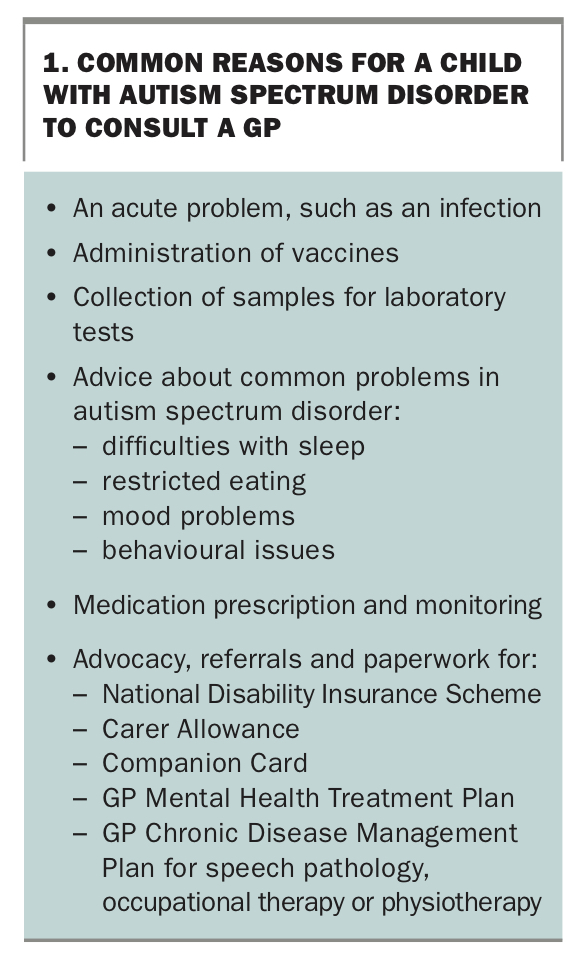
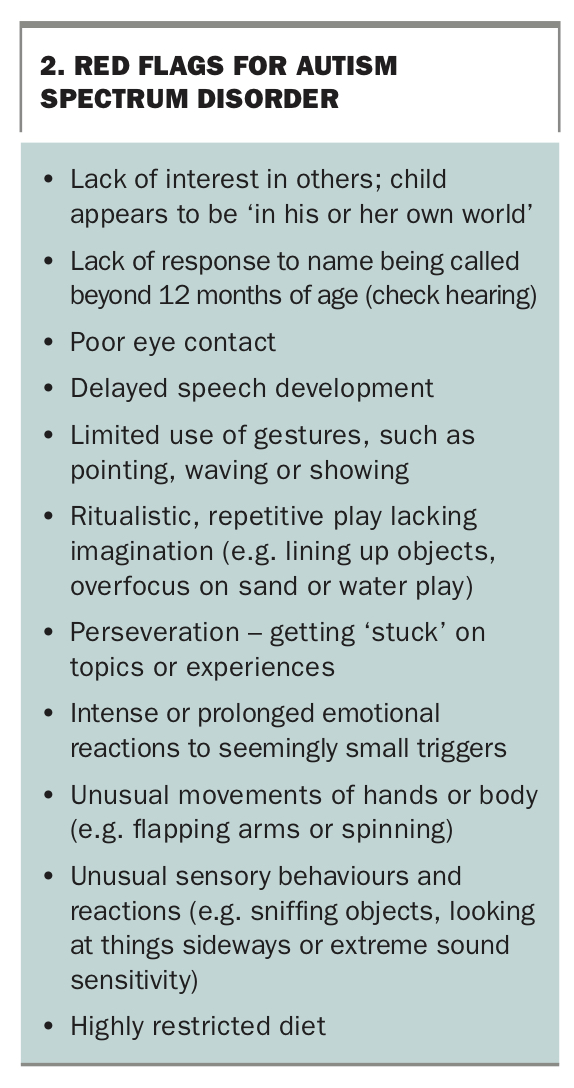
There is a broad range of reasons why a parent of a child with ASD might arrange an appointment with the GP (Box 1). If the reason for the consultation is known in advance, different approaches to planning and conducting the consultation may be considered for different problems. In the early years of a child’s journey with ASD, the diagnosis may still be evolving, and the GP’s role is key. A GP may be the first to identify a child who has red flags for ASD (Box 2). They may need to sensitively convey this information to the parents and refer the child for early paediatric assessment. GPs can also initiate a referral for early intervention services.
{kind=link}
{kind=link}
Gaining rapport
A core tenet of paediatric practice is the establishment of rapport and trust with both parents and children. In a consultation, spending some time initially interacting with the child in a nonthreatening way can start in the waiting room. For instance, instead of calling out the child’s name from the doorway, the doctor can approach the child gently and get down on their level by sitting or kneeling, without crowding them. Having the doctor introduce him- or herself, thank the child for coming to see them and inviting the child and parent into the consulting room for a chat and a play signals to both the child and the parent that the doctor is interested in the child’s perspective.
Once in the consulting room, the focus should initially be on the child. Paper and pencils or crayons can be a great way to engage preschoolers and early primary school-aged children by sharing a drawing task together while chatting. Older children may be engaged by asking about an area of interest (with the caveat that, for children on the autism spectrum, this may result in a lengthy monologue that takes up the entire consultation). To allow for rapport building, which is essential for long-term engagement with children with ASD, booking an extended appointment may remove some of the time pressure. Flexibility is often required – things may not go according to plan.
When examining a child, it is important to be aware of any sensory difficulties that may be present. Many children with ASD do not like to be touched, and some can be upset by sudden noises or unexpected movement. Depending on the child’s capacity, checking with the parent as well as the child before physical examination will help avoid any missteps in engagement that may be difficult to recover from. When treating the child, often the parents’ expectations and issues must also be managed, which can present an extra layer of complexity.
Given that genetics play a large role in the aetiology of ASD, it is not unusual to encounter a parent with similar traits when managing children on the spectrum. For example, when discussing the difficulties a child with ASD may face in regard to social interactions and rigidity, the parent may reflect on his or her own challenges in these areas. It is helpful to be alert to this possibility and, if ASD features are recognised in the parent, to provide relatively concrete information and advice.
Communication
Although children with ASD vary enormously, they often have deficits in nonverbal communicative behaviour, such as eye contact and use of gesture, and may have limited social reciprocity. Language delay is common in children with ASD; however, language capacity may not reflect cognitive capacity. Furthermore, expressive language delay does not necessarily mean that the child will also have receptive language delay, so a child with ASD may understand and remember more than they appear to.
Many children with ASD are highly anxious, and this may affect their comfort in speaking with unfamiliar people. Just because a child chooses not to speak in the consulting room does not mean they are nonverbal at home. The patient and parent should be reassured that it is OK if they do not want to speak. Often having the doctor acknowledge to the child that they are talking about them because they are interested to know more about them will help them feel more comfortable.
Conversely, in some children with ASD, expressive language may seem typical for their age, but higher-level receptive language concepts may not be well understood. It is important to check with both the child and parent regarding their comprehension. Interactions with the child should be based on their developmental level rather than chronological age – for example, a 10-year-old with a mild intellectual disability will think, act and communicate more like a 6- or 7-year-old. Children with ASD may have an IQ in the normal range, while their social and communication skills resemble those of a younger or older child.
This will also be important to consider if there is a need to undertake any minor procedures in general practice, as children under stress tend to function and react more like a younger child. In addition to pitching communication at the right level, planning ahead with enough staff members to ensure the procedure is safe and successful on the first attempt, keeping a calm environment and using tools for distraction (e.g. blowing bubbles, playing music, TV, smartphone or tablet) can all be useful strategies.
Behaviour
Some children and adolescents with ASD experience intense anxiety and sensory sensitivity, which can manifest as unpredictable behaviour. This can vary in expression from withdrawal and social avoidance to restlessness (e.g. pacing, jumping), loudness, defiance or aggression. The clinical situation can be difficult and even distressing for the patient, family, reception staff and doctor. Enabling children to have a positive experience and feel safe when coming to the clinic is even more crucial in the case of children with ASD, as, given the rigidity and perseverance these children often display, a negative experience may be difficult to shift in future appointments. It may have been a challenge for the parent to convince the child to attend an appointment, and there may be a limited window of opportunity for them to remain engaged.
Anticipation and preparation can help, including considering whether the child needs to be reviewed in person or if telehealth can be used. This will depend on the capacity of the child to engage online and the reason for the appointment (i.e. do they need to be examined?). If using telehealth, video consultation is preferable to telephone consultation. It is surprising how much useful clinical information can be gathered by observing and interacting with children online. For more challenging cases or complex scenarios, a hybrid model – where the history is first obtained from a parent by telehealth (particularly where there may be a need for prolonged discussion about a behaviour or issue), followed by an in-person review that can focus more on the child – could be considered.
For children with more severe ASD, it may be best to schedule appointments at times when there will be fewer other patients in the waiting room or when there will not be an extensive wait if there are delays in the day’s schedule, such as first thing in the morning or immediately after lunch. It is important to consider not only the interactions with the child but also how the physical environment in the clinic, from waiting room to consulting room, may affect a child with ASD. Waiting time should be minimised as much as possible, and patients would ideally be able to wait in a quiet area. Some families prefer to wait in the car until called by reception when the doctor is ready.
Despite all best efforts, a child may on occasion have a ‘meltdown’ in the waiting area or office, triggered by sensory overload in an unfamiliar environment or some other stimulus. Once this occurs, no intervention is likely to help. The best approach is to check with the parent or carer about what they think might help the patient to settle, then to give them space in a safe area and leave them until it resolves. If the appointment has already commenced, the only option may be to terminate the consultation and call the family later to check in and reschedule (perhaps via video conference next time).
Coprescribing
Children with ASD may present to a GP because they require a prescription for medication. Although paediatricians generally aim to see a child often enough to ensure a family has an adequate supply of medications, occasionally repeats get misplaced or appointments rescheduled or missed, resulting in a sudden need for a script.
Given that anxiety and attention deficit hyperactivity disorder are common comorbid conditions, it is not unusual for children with ASD to be prescribed selective serotonin reuptake inhibitors (SSRIs), stimulants (methylphenidate and dexamfetamine) and, in some cases, second-line (nonstimulant) agents for attention deficit hyperactivity disorder, such as clonidine, guanfacine or atomoxetine. Children with significant behavioural issues may be prescribed second-generation antipsychotics, such as risperidone or aripiprazole, or mood stabilisers such as sodium valproate. Melatonin is sometimes used to assist when there are difficulties with sleep onset, and sedatives such as clonidine or chloral hydrate may be prescribed to help with sleep maintenance.2
Despite being familiar with these medications and authorised to initiate all except the stimulants, some GPs may feel uncomfortable prescribing them for children. Each state and territory has its own laws about prescribing stimulant medications but, in most states, GPs can prescribe stimulants for continuing use after they have been initiated by a paediatrician, generally with specialist review every 12 months.3 If there are any concerns, GPs are encouraged to contact the child’s paediatrician regarding medication doses and the rationale for use. Paediatricians are happy to discuss shared care and shared prescribing for patients.
Interventions
The bedrock of ASD management is therapeutic intervention from allied health practitioners, such as speech pathologists, occupational therapists and psychologists, which can vary depending on the specific needs and developmental stage of each child. Speech pathology and occupational therapy are more often used for younger children, whereas older children may receive more benefit from psychological input to support their social interactions and anxieties as their social world becomes more complex and they develop the capacity to engage in therapy.
However, there is a bewildering array of interventions that families of children with ASD might try. Most have a limited evidence base, and none have been shown to influence the core difficulties in ASD, although some can be helpful for associated problems, such as poor social skills, anxiety, emotional dysregulation and inattention. Parents often do their own research and decide which interventions they wish to access, but they may ask GPs for advice on which interventions might best help their child. Goal setting for any therapy should incorporate both current symptoms and longer-term function.
Many therapists use social stories to help children with ASD learn alternative, appropriate ways of responding in social situations. Positive behaviour support and applied behaviour analysis approaches help children with ASD learn more prosocial interactions, communications and behaviours. These interventions are delivered in the child’s everyday environment (e.g. home, kindergarten) so the child can apply the learned skills outside of therapy sessions. They can lead to improved independence in daily living skills and reduced aggression.
Medications such as SSRIs and stimulants can often be helpful in enabling the child to settle and interact better with others, which in turn means they can access allied health interventions more usefully. Routine dietary supplements or exclusions do not usually make a difference to the child’s function. However, some children with ASD have highly restricted diets and are at risk of nutritional deficiencies (e.g. iron, vitamin B12 and vitamin C), which should be identified and addressed early.
Advocacy
Although a paediatrician’s primary focus is the child, they must also manage the child within the context of their family. Having a child with ASD can place significant strain on a family, and parents need to be supported so they can best support their child. A large component of supporting a family and child with ASD is to advocate and assist with linking them with services, and GPs play an important role in facilitating this. This might include:
- completing forms for supports, such as Carer Allowance and Companion Cards
- writing a letter to a school or kindergarten to support an application for special needs funding
- arranging a GP Management Plan or Team Care Arrangement to access allied health care
- arranging a GP Mental Health Treatment Plan for the child or other family members.
Many children with ASD will have National Disability Insurance Scheme plans, and a letter regarding the effect of the child’s ASD on social inclusion and participation for the patient and parents can go a long way to supporting an application for key services, such as support workers and respite care.
Paediatric practice often considers who is ‘holding the child’ throughout this journey – that is, who has responsibility for managing the child’s medical, emotional and psychological needs. In the same way, a trusted GP can become the essential person who ‘holds the family’ throughout this journey. The power of a well-written letter from a medical practitioner to influence an outcome for a family and child should never be underestimated.
Transition from paediatric care
Paediatricians generally manage patients until about the age of 18 years, or the completion of high school and the commencement of adult education, training and employment. Most patients with ASD have no related major medical issues, so there is no need for hospital specialist or physician care. In some cases, the paediatrician may refer the patient to an adult psychiatrist to continue management of mental health and behavioural problems, including the ongoing prescribing of medications, which GPs may continue to coprescribe.
However, it is more often the GP who will provide medical care for patients with ASD in their adult life. Involving the GP in planned shared care for some years before the cessation of paediatric care (e.g. alternating appointments with the paediatrician) can improve this transition. This enables the patient and family to get to know the GP and enables the GP to gain a good understanding of the patient’s needs, in partnership with the paediatrician, during the patient’s adolescence. This process results in a smoother transition in which the young person and family feel confident about ongoing care in adulthood. In many cases, GPs will have already developed a more proactive approach to building this relationship via routine general practice care throughout the primary school years.
Conclusion
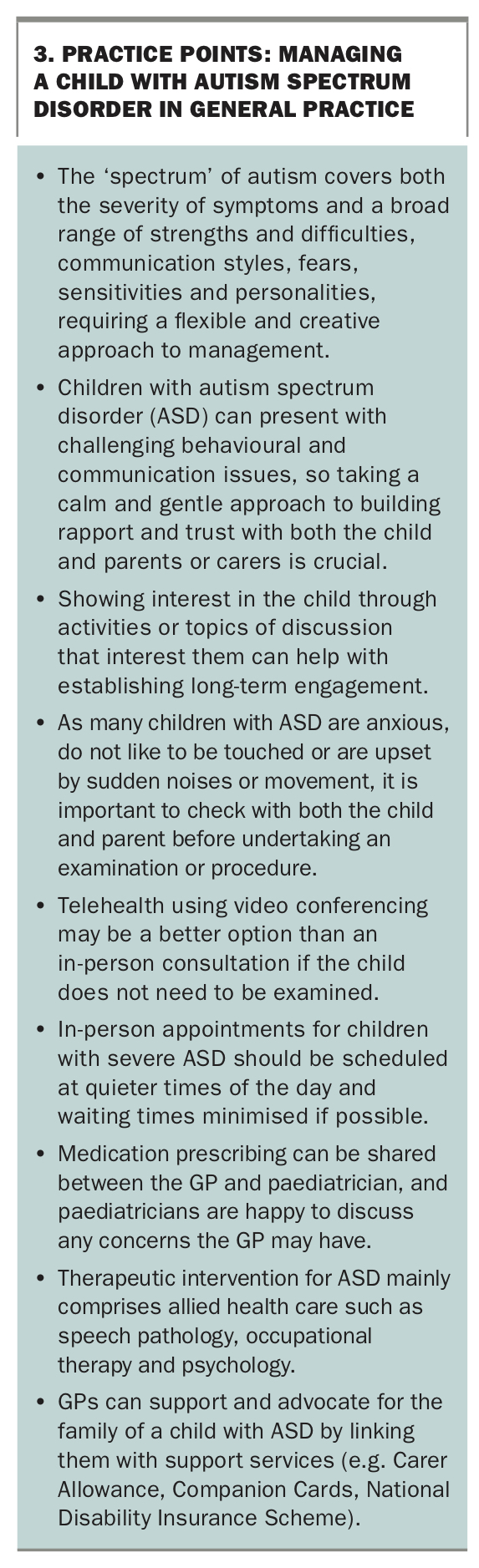
While the responsibility for many management decisions for children with ASD will lie with paediatricians, GPs play an important role in supporting children and families on their journey well beyond the paediatric timeframe. Children with autism can be challenging but also delightful, funny, quirky and uniquely individual. As the adage goes, if you’ve seen one child with autism – you’ve seen one child with autism. There is a broad range of presentations, so the relevance and effectiveness of management strategies will vary from patient to patient. As in any paediatric consultation, allowing time to gain rapport and trust and taking a warm, gentle and respectful approach will pay dividends for future medical care. Practice points for managing a child with ASD are shown in Box 3. MT
{kind=link}