Genetic carrier screening: an update for GPs

Reproductive genetic carrier screening is an essential part of preconception and early pregnancy counselling. As the first point of contact for couples planning pregnancy or during early pregnancy, GPs are well placed to discuss genetic screening and recommend tests based on a couple’s risk factors, such as ethnicity, and personal preferences.
Genetic testing has rapidly expanded over the past decade, with a well-established genetic basis for more than 5000 conditions.1 The option of genetic carrier screening is an important part of preconception counselling and should be routinely discussed with all couples and individuals planning and in the early stages of pregnancy.2 However, many prospective parents are not offered reproductive genetic carrier screening. GPs are often the first point of contact for women planning pregnancy, and as such, are perfectly placed to discuss genetic carrier screening. As advances in technology allow genetic testing to be more easily accessible, an understanding of genetic carrier screening is increasingly relevant to GPs. Resources to help GPs and patients improve their understanding of genetic testing are listed in
Box 1.
{kind=link}
What is carrier screening?
Genetic mutations may occur spontaneously or they may be inherited. Common modes of inheritance include autosomal dominant, autosomal recessive, X-linked, Y-linked, codominant and mitochondrial patterns.3
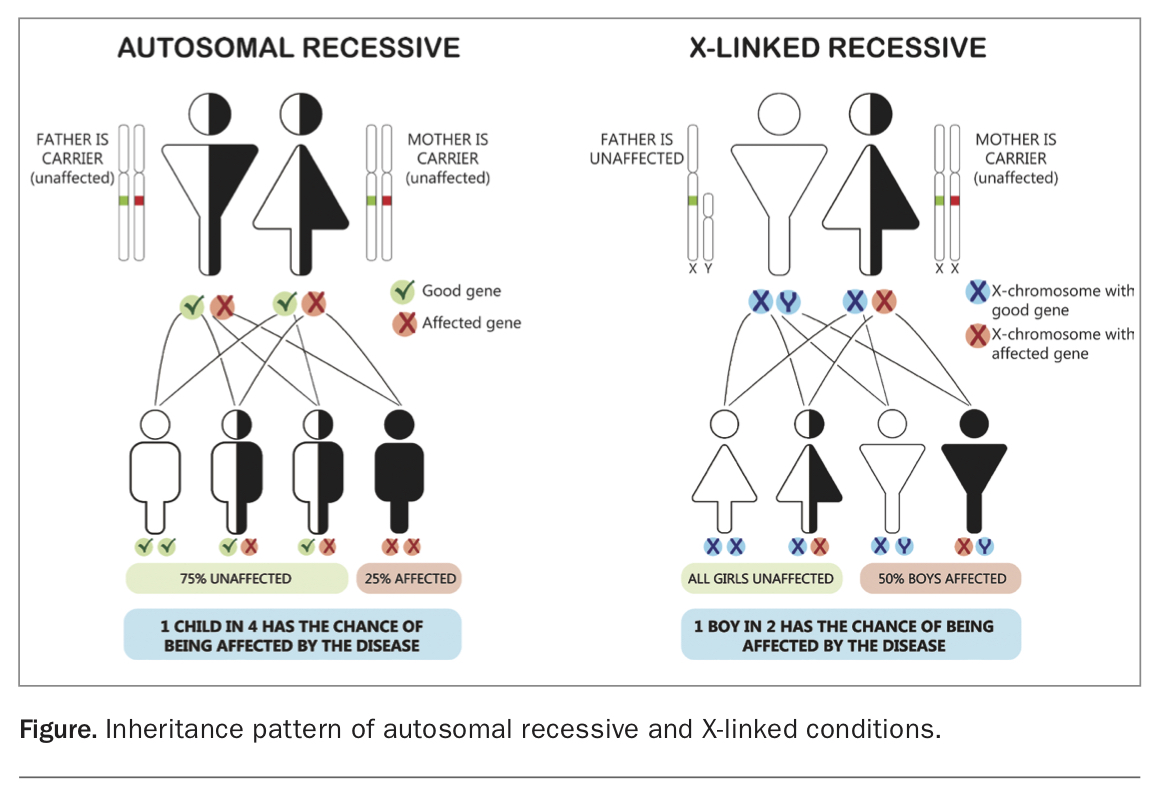
Reproductive genetic carrier screening assesses for autosomal recessive and X-linked mutations, which may go on to affect the health of a child. Examples of autosomal recessive diseases include cystic fibrosis, spinal muscular atrophy, Tay Sachs disease and sickle cell anaemia. If both partners are carriers for the same mutation, they have a one in four chance of having a child affected by the disease (Figure).
{kind=link}
X-linked conditions are those linked to a mutation on the X chromosome. Men are disproportionately affected by X-linked conditions as they receive only one copy of the X chromosome. As women receive two copies of the X chromosome, they are more often carriers or may have mild symptoms only of an X-linked condition. If a woman is a carrier for an X-linked disease, she has a 50% chance of having a son affected by the disease (Figure).4 Examples of X-linked conditions include fragile X syndrome, haemophilia A and B and Duchenne muscular dystrophy.
Why screen?
Although individually rare, the combined risk of autosomal recessive and X-linked conditions is comparatively common. One in 200 children is born with an autosomal recessive or X-linked condition. In comparison, one in 800 children is born with Down syndrome.2 Inherited rare genetic conditions account for 10% of infant mortality and 20% of paediatric inpatient admissions.5
On average, every individual is a carrier for two recessive genes known to be associated with severe disease.3 Around 1 to 2 % of non-consanguineous couples will share the same autosomal recessive mutation or carry an X-linked disease; such couples have a 25% chance of having an affected child.5 This risk is significantly higher in consanguineous couples.
Most parents who have a child affected by a genetic condition have no prior family history of the disease.5 Reproductive genetic carrier screening gives couples the opportunity to find out if they have an increased chance of having a child with a serious genetic condition and allows the opportunity to make informed reproductive choices.
When to screen
The best time to offer genetic carrier screening is before conception, to allow couples the greatest opportunity to make informed choices regarding reproductive options. Screening can also be offered in early pregnancy; however, reproductive choices are much more limited, and it is important to consider state and territory laws regarding pregnancy termination.
Types of screening
The Royal Australian and New Zealand College of Obstetricians and Gynaecologists (RANZCOG) and The Royal Australian College of General Practitioners (RACGP) guidelines state that all couples planning pregnancy should have a comprehensive family history recorded, and those with a relevant family history or who are known carriers for a genetic condition should be offered referral for specialised genetic counselling. RACGP guidelines recommend offering low-risk couples screening for the more common conditions (triple condition screening).6 RANZCOG also recommends that all women be offered basic haemoglobinopathy screening and genetic carrier screening via triple or expanded testing, regardless of ethnicity or family history.2
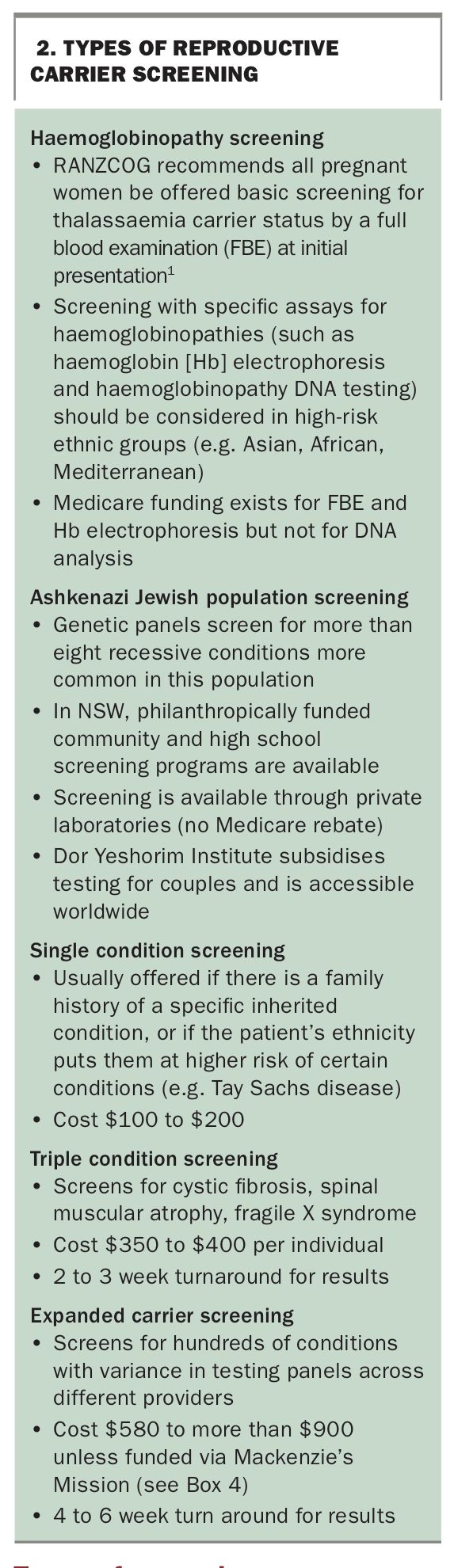
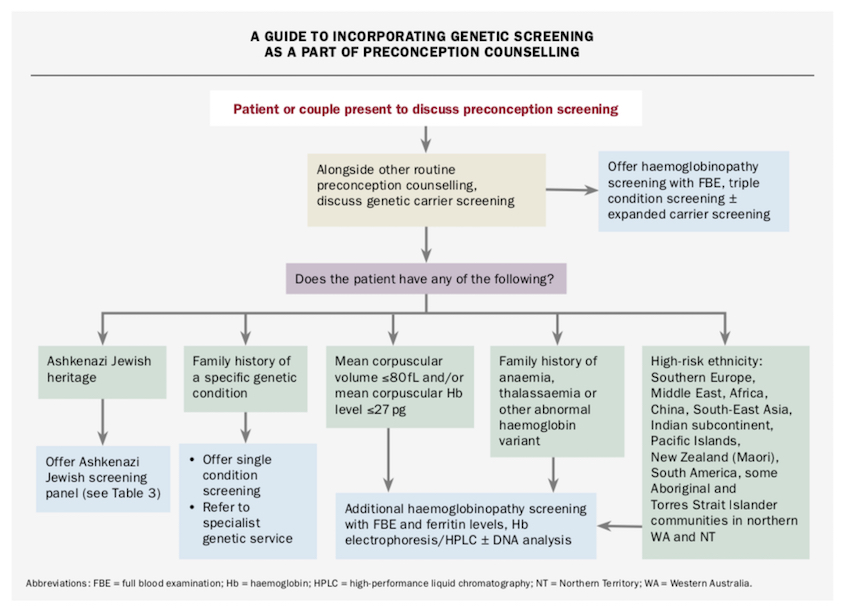
Carrier screening is offered in Australia by many private companies by a simple blood test or buccal swab. The cost can vary depending on provider and testing panels. There is no Medicare rebate for genetic carrier screening, although haemoglobinopathy screening may be partially funded by state and territory governments. Reproductive carrier screens that should be considered for couples planning, or in the early stages of pregnancy are summarised in Box 2. An algorithm for incorporating genetic screening during preconception counselling is presented in the Flowchart.
{kind=link}
{kind=link}
Haemoglobinopathy screening
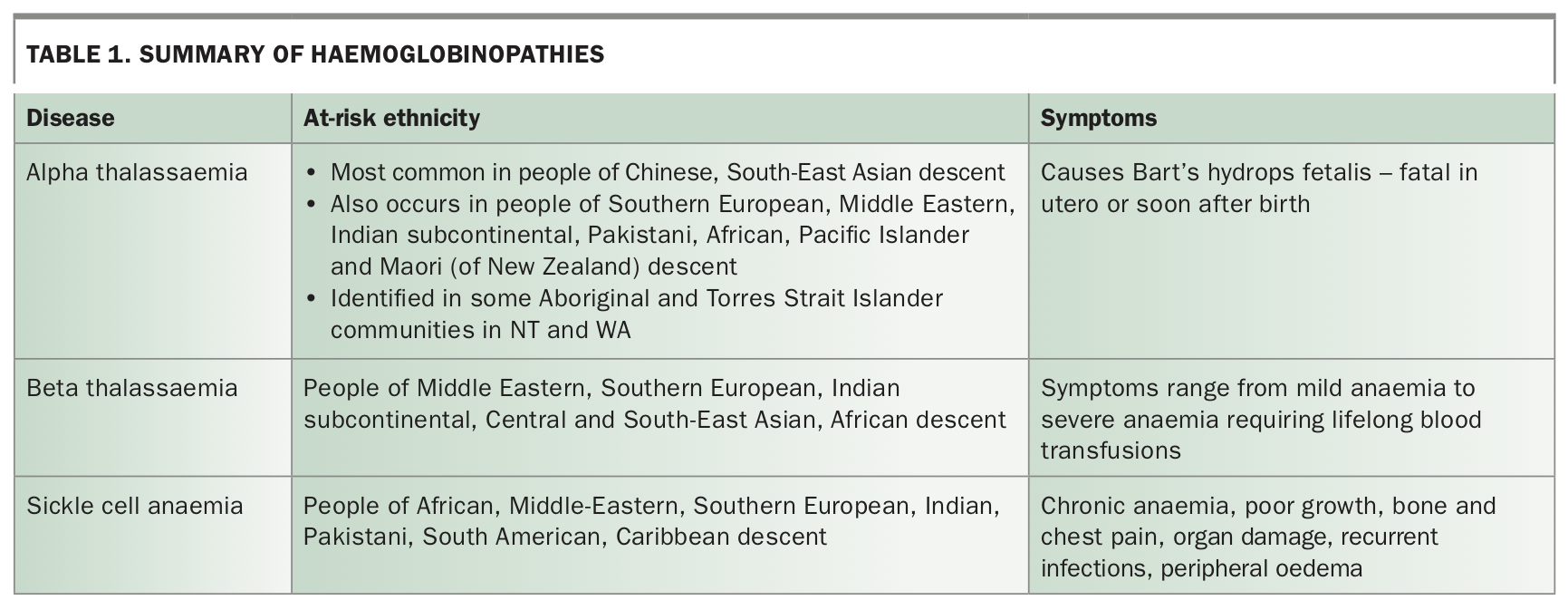
The RANZCOG recommends that all women should be offered basic haemoglobinopathy screening with full blood examination, with further testing for people of certain ethnicities (Table 1).2,9 Haemoglobinopathy screening is performed inconsistently across Australia because of differences in state and territory guidelines and funding. Australia has long been an ethnically diverse population with a significant number of carriers of beta thalassaemia mutations, particularly in individuals of Mediterranean, Middle Eastern and African backgrounds.7 Alpha thalassaemia mutations are common among people of South-East Asian descent. With increasing immigration from this region, testing for alpha thalassaemia should be considered as a part of standard thalassaemia testing.8
{kind=link}
Although Medicare funding for thalassaemia testing with haemoglobin electrophoresis and high-performance liquid chromatography has been available since 1998, specific alpha thalassaemia DNA testing is not currently covered.8 Funding for alpha thalassaemia screening varies across states and territories, with the Victorian government currently the only state to offer fully subsidised alpha thalassaemia testing.9
Triple condition screening and expanded carrier screening
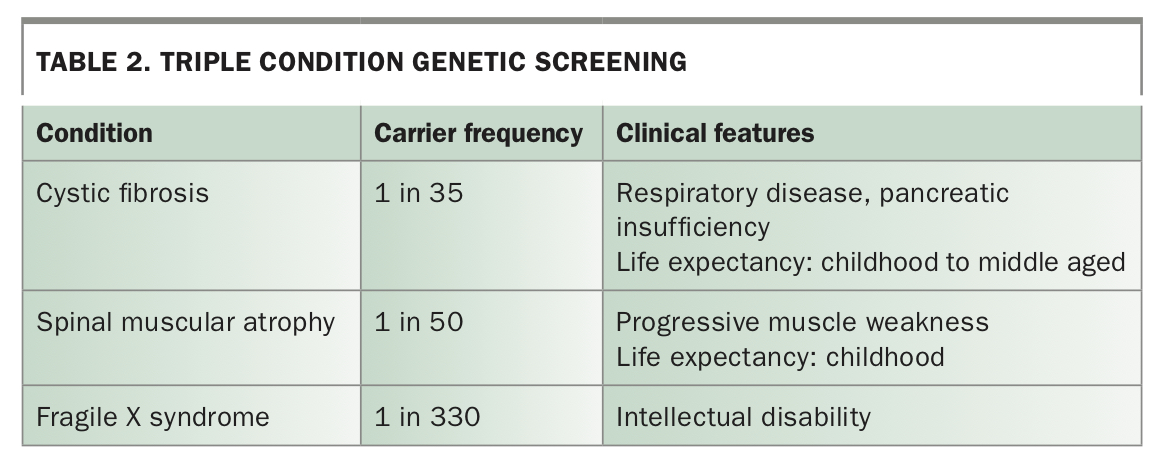
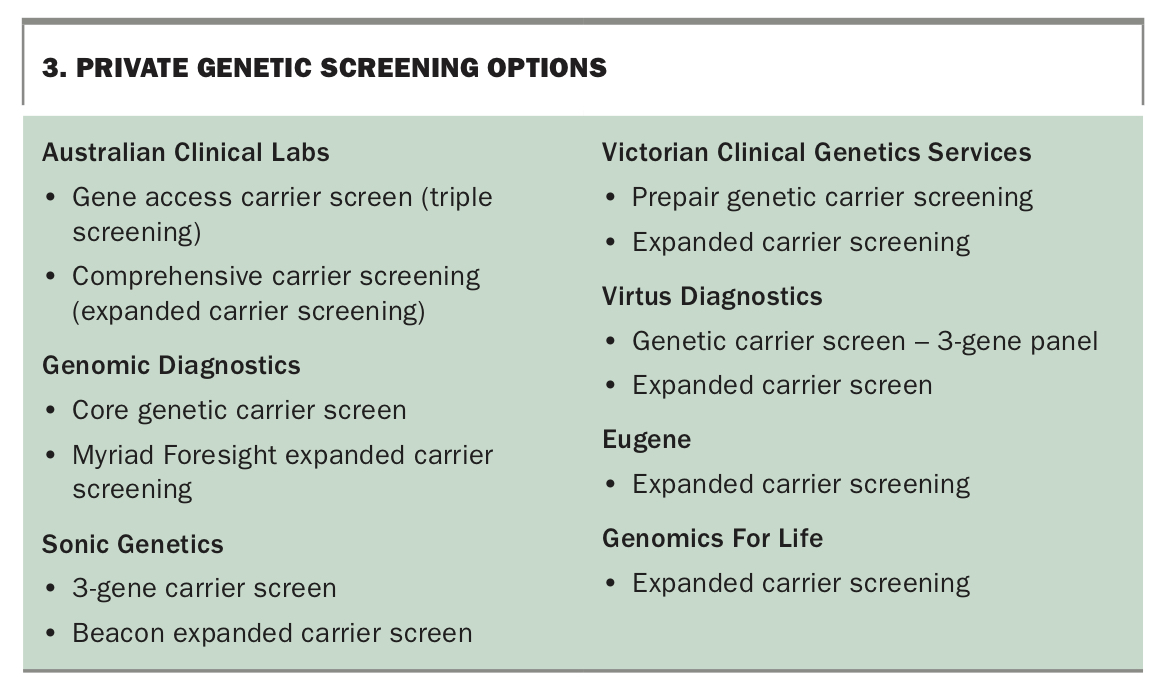
Triple condition screening is offered via many private companies for the three most common hereditary conditions – cystic fibrosis, spinal muscular atrophy and fragile X syndrome (Table 2). Additionally, expanded carrier testing is available through private laboratories, which allows testing for hundreds of genetic conditions (Box 3). Next generation sequencing is now widely available and can screen for a rapidly increasing number of conditions, at a fraction of its previous cost.2
{kind=link}
{kind=link}
Screening for ethnicity-specific conditions: monogenetic recessive conditions in the Ashkenazi Jewish community
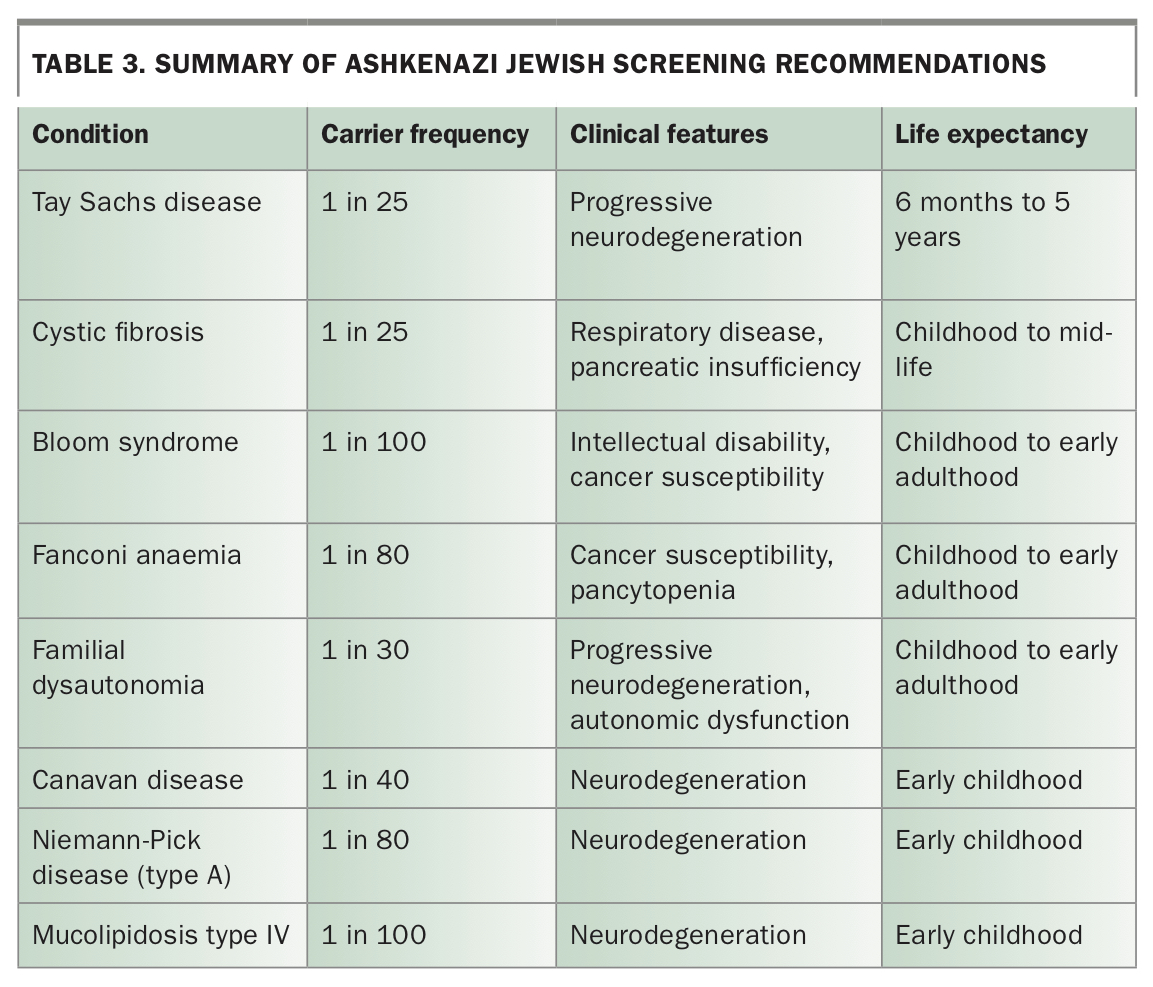
Further ethnicity-specific screening is suggested for certain at-risk groups. For instance, in Australia, Jewish people with Ashkenazi (Eastern European) ancestry have an increased incidence of severe monogenetic recessive conditions, including cystic fibrosis, Tay Sachs disease and Bloom syndrome, for which screening is recommended (Table 3). 2,10,11 Around one in five Ashkenazi Jewish individuals screened will be carriers for one or more of these conditions. With wide uptake of screening in Jewish communities, the prevalence of Tay Sachs disease has reduced by 90%.2,3,5
{kind=link}
If an Ashkenazi Jewish individual is diagnosed as a carrier for one or more conditions, their partner should be offered screening for the condition(s) in question, regardless of heritage. There is no Medicare rebate for Ashkenazi Jewish screening panels but some state genetic services may subsidise testing. In NSW, school screening is offered to Jewish students for free in select high schools, and community screening is available to Jewish adults who are planning pregnancy via the Community Genetics Program. Dor Yeshorim is an international Jewish genetic screening program that provides screening at reduced cost and is accessible to Ashkenazi Jewish couples worldwide.
Mackenzie’s Mission
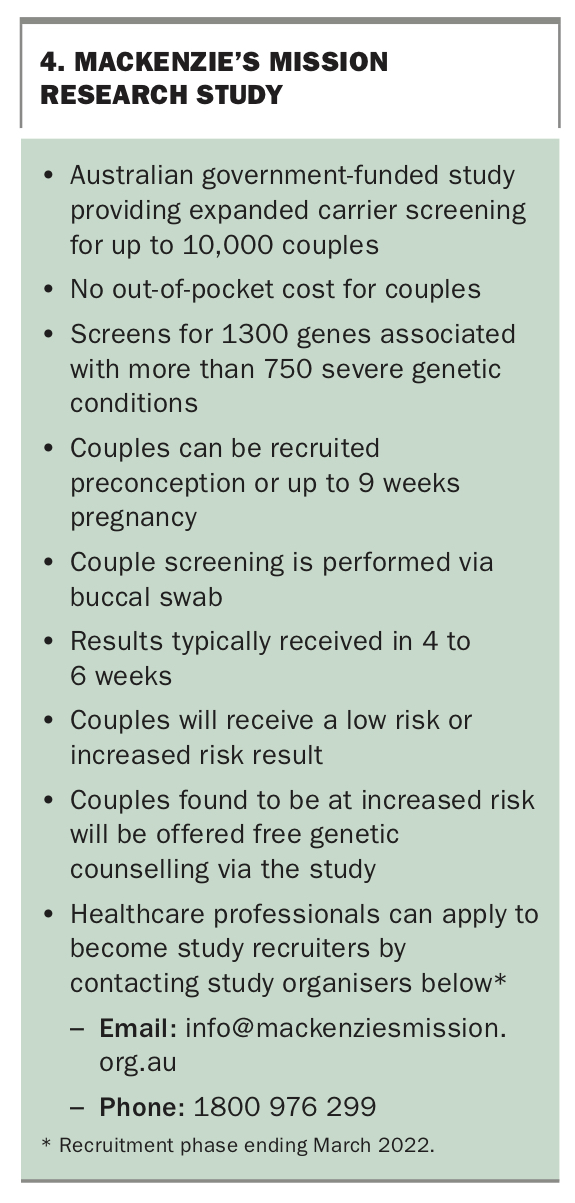
In 2018, the Australian government announced $20 billion in funding for reproductive genetic carrier screening via Mackenzie’s Mission, named after Mackenzie Casella, who passed away from spinal muscular atrophy at 7 months of age. Mackenzie’s mission is aiming to recruit 10,000 couples across Australia for expanded carrier screening, with the goal of making genetic carrier screening freely available and easily accessible to all couples (Box 4). Couples enrolled in Mackenzie’s Mission are offered expanded carrier screening with no out-of-pocket cost. If found to be at increased risk, couples will be offered free genetic counselling, as well as the option to access one funded cycle of IVF with preimplantation genetic testing.
{kind=link}
Sequential vs couple screening
Sequential testing involves testing one partner first, with subsequent screening of the other partner only if an autosomal recessive mutation is identified. The woman is usually screened first given the relevance of her carrier status for X-linked conditions.2 Sequential screening is the norm when testing for few conditions (e.g. triple condition screening) and when time is not a pressing factor (i.e. not late in first trimester of pregnancy).
Couple screening is more appropriate when many conditions are being screened for. Up to 75% of individuals will be a carrier for at least one of the many hundreds of conditions screened for in expanded carrier screening, so simultaneous screening of both partners is more efficient.12 A couple is given a low-risk result if found not to have the same autosomal recessive mutation and no X-linked mutation is identified.
Follow up
Couples found to be at increased risk should be referred for genetic counselling to a clinical geneticist or genetic counsellor to ensure they fully understand the implications of their result and to discuss reproductive options. State-funded genetic counselling is available through the public health system, and most private testing companies offer genetic counselling as part of their testing service.
Reproductive options include:2
- proceeding with a natural pregnancy and accepting the child may be affected
- undergoing further screening with noninvasive prenatal testing or early pregnancy testing via chorionic villus sampling or amniocentesis and considering termination of an affected pregnancy
- undergoing IVF with pre-implantation genetic testing
- undergoing IVF with donor eggs or sperm or embryos
- choosing to adopt
- choosing not to have children.
Conclusion
Genetic carrier screening should routinely be offered to all women and couples planning and in the early stages of pregnancy to assess the risk of carrying shared autosomal recessive or X-linked mutations. Haemoglobinopathy screening and triple condition screening for cystic fibrosis, spinal muscular atrophy and fragile X syndrome should be discussed with all couples before conception and in early pregnancy, as well as the option of expanded screening. Couples with a known family history or known carrier status should be offered referral for genetic counselling. Genetic carrier screening gives couples the chance to make informed decisions regarding their reproductive options. The Practice Points summarise the importance of preconception and early pregnancy genetic screening. MT
References
$File/1531%20Final%20PSD-Mar2019.pdf (accessed February 2022).