Iron deficiency – excluding serious causes

Iron deficiency is a common issue among patients presenting to general practice. Management requires oral or intravenous iron replacement coupled with clinical assessment and consideration of further investigations to exclude serious causes.
Iron deficiency anaemia is the most common nutritional deficiency worldwide. Although it can be diagnosed simply through blood tests, the aetiology is diverse, and management can be nuanced. The causes range from inadequate dietary intake through malabsorption to bleeding, ulceration and malignancy of the gastrointestinal or genitourinary tracts. Prompt recognition and investigation of iron deficiency, especially in men and postmenopausal women, can lead to improved outcomes.
Appropriate iron replacement therapy is important for optimal patient care. This article provides an overview of iron deficiency in adults, including the possible causes, management options and indications for further investigations.
Diagnosis and biochemical markers
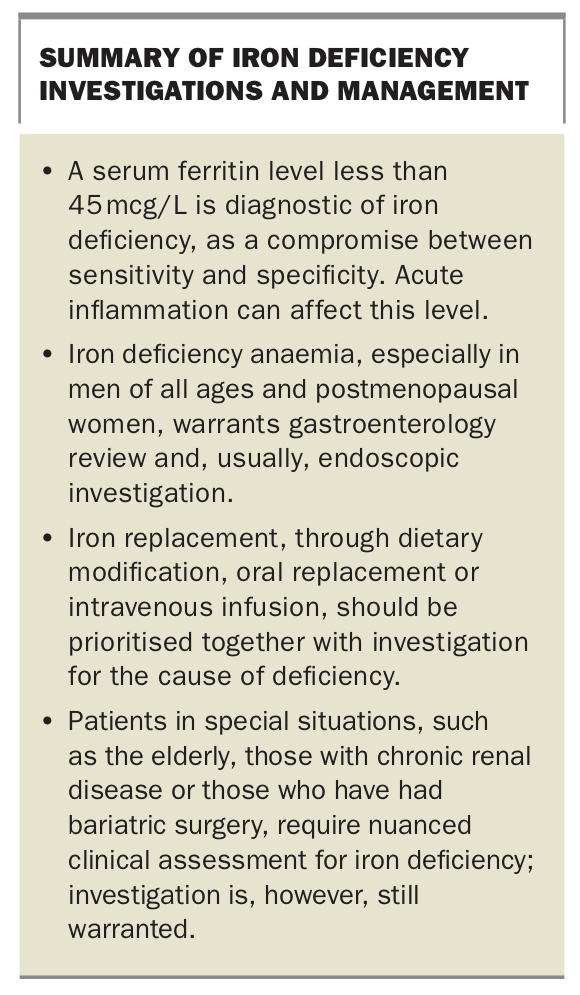
Serum ferritin is a measure of total iron stores and is the most useful marker of iron deficiency. A value less than 15 mcg/L is specific (99%) but not sensitive (59%) for absent iron stores, whereas a value less than 30 mcg/L is generally considered to be diagnostic of iron deficiency.1 A ferritin level greater than 100 mcg/L makes the diagnosis of iron deficiency unlikely.2 A recent practice guideline from the American Gastroenterological Association recommended the use of a threshold ferritin value of less than 45 mcg/L as a compromise between sensitivity (85%) and specificity (92%).2,3 This trade-off balances the benefits of fewer missed diagnoses against the harms of unnecessary diagnostic interventions.
As serum ferritin is an acute phase protein, acute or chronic inflammatory conditions can make biochemical assessment for iron deficiency difficult. In these situations, a decreased serum transferrin receptor saturation level and/or raised total iron binding capacity can be helpful indicators of iron deficiency. Serum iron levels are not helpful: they vary widely and are reduced in an acute phase response.
Iron deficiency anaemia is defined as low iron stores with reduced haemoglobin concentration and mean corpuscular volume (MCV). Anaemia is generally defined as a haemoglobin concentration less than 135 g/L in men and less than 115 g/L in women. Iron deficiency anaemia is microcytic (MCV less than 80 fL) and hypochromic (reduced mean cell haemoglobin [MCH]), although haemoglobinopathies such as thalassaemia can cause this pattern and should also be considered.
The MCV of an individual is generally constant over time. A falling MCV or mean corpuscular haemoglobin concentration (MCHC), even in the normal range, may indicate chronic blood loss and warrants further assessment.
Iron is absorbed primarily in the proximal small intestine (duodenum), and iron homeostasis is dependent on the ferroportin/hepcidin axis. In patients with chronic kidney disease and chronic inflammatory states, hepcidin production is increased, leading to decreased iron absorption.2 These conditions may be associated with iron deficiency but also make the biochemical assessment of true deficiency difficult. Hepcidin is also increased by an oral iron load, which may limit the absorption of oral iron therapy in the short term.
Clinical assessment of causes
Common causes
The most common causes of iron deficiency are:
- inadequate oral intake
- excessive loss through bleeding
- malabsorption.
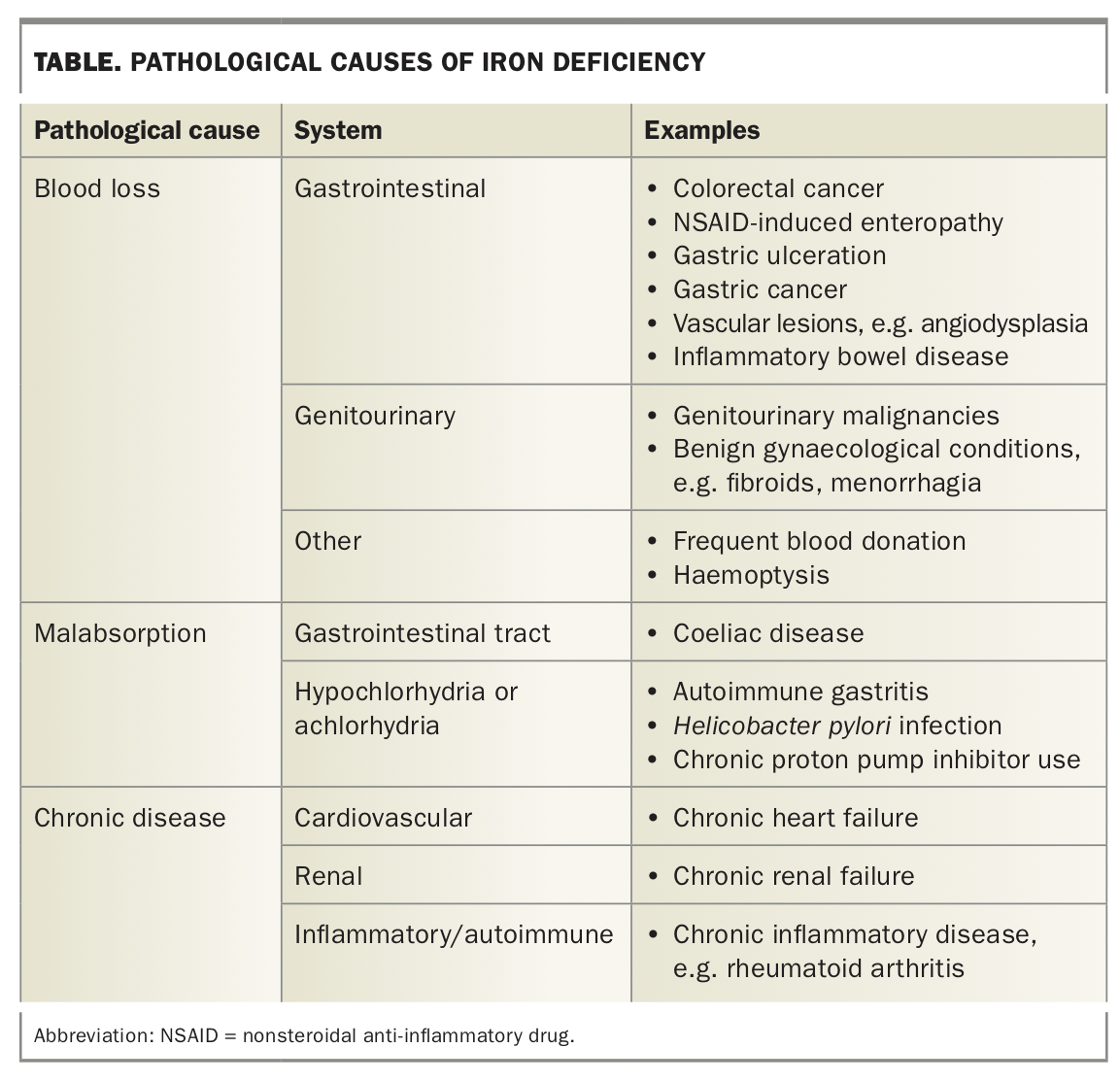
Examples of pathological causes of iron deficiency are listed in the Table.
{kind=link}
Differentiating between causes
Iron deficiency in men and postmenopausal women is commonly associated with chronic, and often occult, gastrointestinal bleeding. History and examination may identify likely causes but the absence of symptoms does not remove the need for complete assessment, particularly colonic causes, in appropriate patients.4
In addition to gastrointestinal bleeding, other causes of blood loss, such as heavy menstrual bleeding, other genitourinary bleeding or regular blood donation should be excluded.
The patient’s family history may reveal relevant conditions, such as colorectal cancer or coeliac disease. Other important factors include medication use (in particular NSAIDs, antiplatelet agents and anticoagulants) and any previous gastric surgery, including bariatric surgery.
The recommended daily intake of iron is 8 mg per day for adult men and postmenopausal women, and 18 mg or more per day for premenopausal women. Inadequate intake of iron can contribute to iron deficiency. Red meat is a rich source of dietary iron with beef containing 3.3 mg of iron per 100 g, compared with chicken thighs that contain only 0.9 mg per 100 g. Recommended iron-rich plant-based products include brown lentils (2.4 mg per 100 g) and kidney beans (1.2 mg per 100 g), but they contain non-haem iron, which is not as readily absorbed. Given differences in dietary knowledge and food preferences between patients, dietary assessment and education is an important aspect of management.
Coeliac disease accounts for 3 to 5% of the causes of iron deficiency anaemia and can present at any age. It is not always symptomatic. A dimorphic blood film (both large and small red cells) is sometimes seen if the patient is deficient in both folate and iron. Coeliac disease can be screened for with serology but should be confirmed by duodenal biopsy. Other malabsorptive causes include gastric surgery and, because of downregulation of iron absorption, Crohn’s disease and other chronic inflammatory states.5
Iron deficiency can be multifactorial, and this should especially be considered in elderly patients or patients with comorbidities. The identification of a likely cause should not preclude full investigation.4
Management
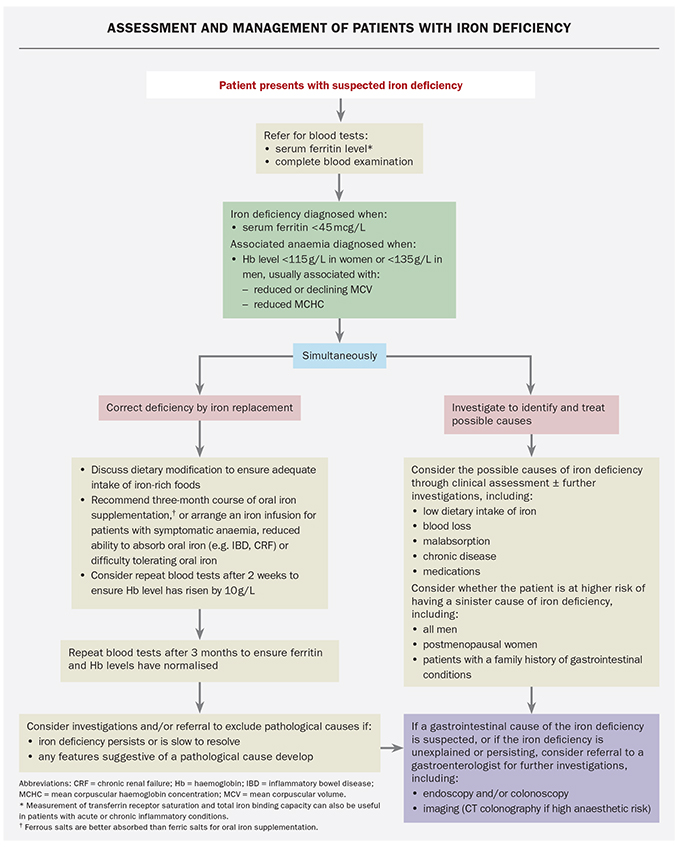
The approach to management involves correction of iron deficiency through dietary, oral or intravenous replacement, and the investigation and treatment of the underlying cause. A suggested approach to the management of patients with iron deficiency is outlined in the Flowchart.
{kind=link}
Iron replacement
The degree of deficiency and the presence of anaemia will dictate the urgency of iron replacement. Mild iron deficiency without anaemia can be corrected with dietary modification and oral supplementation, whereas a patient with an acute gastrointestinal bleed who is iron deficient would generally require an intravenous iron infusion or even a blood transfusion during their hospital stay.
Discussions to improve dietary intake of iron and advice from a dietitian are often beneficial.6
Oral iron supplementation for at least three months should be considered in patients with significant iron deficiency and/or anaemia. The British Society of Gastroenterology guidelines indicate that a good response is present if the patient's haemoglobin level rises by 10 g/L within two weeks of the initiation of replacement therapy in absolute iron deficiency.1 Ongoing iron supplementation is recommended for three months after normalisation of anaemia.
The choice of oral iron supplementation and its mode of administration are important. Ferrous salts are better absorbed than ferric salts. High doses of oral iron increase the hepcidin level, which blocks subsequent absorption. They are also associated with greater rates of adverse events, including constipation, nausea and diarrhoea. Absorption of oral iron appears to be most efficient using intermediate doses (around 60 to 100 mg) on alternate days.7 Slow-release formulations have not been shown to be effective in clinical trials.
If oral iron replacement and dietary modification are unsuccessful or poorly tolerated, intravenous iron replacement should be considered. Intravenous replacement could be considered earlier when more prompt replacement is appropriate, such as in patients with symptomatic anaemia, or in disorders in which there is impaired absorption of iron, such as inflammatory bowel disease or chronic renal disease. Although the initial forms of parenteral iron replacement (dextran-containing formulations) were associated with an increased risk of anaphylaxis, the currently available forms very rarely cause serious infusion reactions.
Further investigation to exclude serious causes
Referral of patients for further investigation of iron deficiency should be arranged if there is any concern about the possibility of a pathological cause from history and physical examination, as well as for asymptomatic men and postmenopausal women, and patients whose iron deficiency is persisting or inadequately responding to a course of iron replacement, as described in the Flowchart.
Gastroenterological investigations
Although faecal occult blood testing is the mainstay of colon cancer screening in the asymptomatic population, its use is not recommended in the assessment of patients with symptoms or any blood test abnormalities.
Investigation for iron deficiency, particularly through bidirectional endoscopy, should not be delayed while iron is being replaced, particularly in patients in whom gastrointestinal causes are more likely. These include men of all ages, postmenopausal women and any patient with upper or lower gastrointestinal symptoms or a family history of gastrointestinal disease.
Gastroscopy may demonstrate oesophageal or gastric cancer, peptic ulcer disease or ulcerative oesophagitis, and is also useful to obtain duodenal biopsies to exclude coeliac disease and other enteropathies such as NSAID-induced enteropathy or upper gut Crohn’s disease. Colonoscopy may find adenocarcinoma, large polyps, vascular malformations such as angiodysplasia, inflammatory bowel disease or uncommon infections like hookworm.
Gastroscopy is not always recommended in patients who have a high anaesthetic risk, given the lower prevalence of gastric and oesophageal cancer in Australian populations, particularly in those without upper gut symptoms.4
In cases of significant comorbidity and anaesthetic risk, CT colonography is an alternative to colonoscopy. CT colonography identifies lesions 6 mm or greater in size and may identify colorectal adenocarcinoma. The disadvantages are that histology cannot be obtained, lesions cannot be tattooed for laparoscopic resection and vascular causes will be missed. Under the Medicare Benefits Schedule, CT colonography is restricted to the investigation of a patient who has had an incomplete colonoscopy in the three months before the scan and/or has a high-grade colonic obstruction, and the service is requested by a specialist or consultant physician who performs colonoscopies in their regular practice.
In patients with negative results on bidirectional endoscopy, small bowel assessment, usually by video capsule endoscopy, can be performed in those with iron deficiency anaemia, but not routinely in those with iron deficiency without anaemia. If a bleeding point is found, most often subtle vascular or inflammatory lesions, the patient can be treated by therapeutic enteroscopy.
Special situations
Iron deficiency without anaemia
There are no clear guidelines regarding the management of iron deficiency without anaemia: each patient should be assessed individually. Broadly speaking, men with iron deficiency without an obvious cause should be referred for endoscopic assessment. Although nonanaemic iron deficiency is more prevalent in young women, in an asymptomatic patient with no relevant family history, endoscopic assessment may not be warranted as, in this situation the diagnostic yields are low. Such cases can be monitored in primary care, unless symptoms develop or iron deficiency persists or worsens despite appropriate replacement.
Post-surgery
Iron deficiency anaemia is common after bariatric (or any gastric) surgery, including both sleeve gastrectomy and bypass. It is postulated that this is secondary to decreased nutritional intake and decreased absorption. Other deficiencies, such as of vitamin B12, are also seen. Nevertheless, new presentations of iron deficiency anaemia in the context of gastric surgery should not preclude patients from endoscopic investigation, despite a lower yield of pathological findings.
Premenopausal women
The likelihood of a gastrointestinal malignancy or other pathology is low in asymptomatic premenopausal women. A trial of iron replacement in premenopausal women should be carried out before referral for bidirectional endoscopy, especially in the context of heavy menstrual bleeding. However, endoscopy is recommended if anaemia or gastrointestinal symptoms are present, menstrual bleeding is insignificant, coeliac disease is suspected or there is a family history of colorectal cancer.
Pregnancy
Anaemia is encountered in over 40% of pregnancies worldwide. Plasma volume increases throughout pregnancy, peaking in the third trimester, between 30 and 34 weeks. Red cell mass also increases, but to a lesser extent, resulting in a ‘physiological’ anaemia. Iron deficiency remains the most common cause of nonphysiological anaemia in pregnancy, because of the increased demand for iron.
In general, although oral iron replacement is encouraged in pregnant women with iron deficiency, endoscopic assessments are generally not recommended unless specific concerning features are present. Gastroscopy and magnetic resonance enterography are considered safer investigations in pregnancy, and there is insufficient data around the safety of colonoscopy.
If iron deficiency is significant, parenteral iron replacement is recommended over oral therapy, especially during the third trimester. As well as improving maternal health, iron supplementation has been shown to increase birthweight and reduce maternal transfusion requirements.7
Heart failure
Iron deficiency, with or without anaemia, is common in patients with heart failure because of the dysregulation of iron homeostasis caused by chronic inflammation. Multiple clinical trials have shown the detrimental impact of iron deficiency on functional capacity, quality of life and even hospital admissions. Iron repletion is advised for patients with ferritin levels less than 100 mcg/L or with levels between 100 and 300 mcg/L and a transferrin saturation less than 20%.8
Chronic renal failure
Iron deficiency in patients with chronic renal failure can be multifactorial. Factors include reduced absorption of iron, reduced intake of dietary iron, blood loss from regular dialysis and, possibly, gastrointestinal bleeding (e.g. angiodysplasia, ulceration or malignancy).
In chronic renal failure, hepcidin upregulation causes an inadequate supply of iron for erythropoiesis despite normal iron stores, resulting in a functional iron deficiency. Parenteral iron in combination with erythropoietin is often needed to correct anaemia.
Conclusion
Iron deficiency, the most common nutritional deficiency, is not a diagnosis in itself. Assessment and investigation in primary care and, when required, specialist services, is important to identify those with serious causes, especially in men of all ages and postmenopausal women. Iron replacement can be through dietary modification and oral intravenous supplementation, depending on patient preference and the severity of the iron deficiency. Summary points on iron deficiency are listed in the Box. MT
{kind=link}
COMPETING INTERESTS: None.