A sudden outbreak of facial papules and pustules

Test your diagnostic skills in our regular dermatology quiz. What is the cause of these painful lesions on a woman’s face?
Case presentation
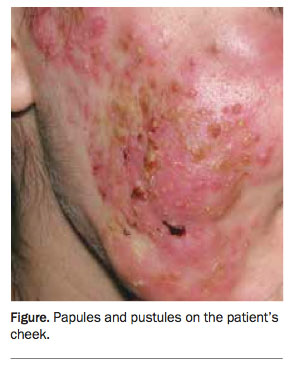
A 42-year-old woman presents with an eruption of papules and pustules on her chin and both cheeks (Figure). The lesions are painful and tender and associated with oedema and lymphadenopathy. The lesions appeared suddenly about three weeks ago. She is systemically well and afebrile.
{kind=link}
The patient has a history of minor acne as a teenager. She denies taking any medications.
Skin swabs and scrapings have been taken from the lesions and returned negative results for bacteria, herpes viruses and fungi. She has been treated with oral flucloxacillin, but the condition has not improved.
Differential diagnosis
Conditions to consider in the differential diagnosis include the following.
- Nodulocystic acne. This severe form of acne presents as pustules, cysts, papules and comedones and is usually seen in adolescents and young adults. There is a subtype (acne fulminans) associated with systemic upset. Severe nodulocystic acne would be very unlikely in a woman who is 42 years of age.
- Tinea faciei. Tinea infections are caused by dermatophyte fungi and have a classic appearance of a scaly patch with central clearing. However, tinea infections are occasionally acutely inflammatory and pustular, particularly when the pathogen is acquired from an animal. Even in the presence of dramatic inflammation, patients remain systemically well.
- Herpes infections. A primary attack of cutaneous herpes simplex infection may sometimes be severe. The lesions are typically small, closely grouped vesicles on an erythematous base and they may follow a linear (zosteriform) distribution. A severe herpes simplex infection is usually accompanied by lymphadenopathy, pain and fever. Herpes zoster may also present as an acute infection with vesicles that become pustular and erosive – the eruption is nearly always unilateral with a dermatomal distribution – and it is frequently severely painful.
- Impetigo. A staphylococcal infection should be considered in the differential diagnosis of any pustular eruption. However, it would be very unlikely to be as severely inflammatory as the skin eruption seen in the case patient presented here. Impetigo would be ruled out by negative bacteriology and a complete lack of response to treatment with flucloxacillin.
- Sweet’s syndrome. This uncommon inflammatory dermatosis often follows a streptococcal infection but may also be a sign of serious systemic disease. Patients present with acutely inflammatory plaques that may appear vesicular due to oedema. They are usually febrile and unwell, with a neutrophilia and elevated C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR).
- Rosacea fulminans (pyoderma faciale). This is the correct diagnosis. This uncommon and alarming eruption is generally seen in middle-aged women and is usually confined to the face. The onset is typically acute and, despite the highly inflammatory appearance of the skin eruption, the patient remains well. The pustular lesions and cystic swellings, which may be connected by sinuses, are itchy, tender and painful, and these occur on a background of erythema and oedema. Comedones are not part of the clinical picture and there is not always a history of typical rosacea. Rosacea fulminans may occur in pregnancy.1 There may be residual scarring after the eruption has cleared; this scarring is minimal and not proportionate to the severity of the lesions. Rosacea fulminans is often a clinical diagnosis and one of exclusion. For the case presented here, the skin eruption is consistent with the clinical features of rosacea fulminans; the patient is female and within the typical age range and infective causes have been ruled out.
Cause
It is not clear whether rosacea fulminans is a variant of rosacea or acne vulgaris or a separate entity.2 It has been suggested that hormones may play a role because rosacea fulminans is a condition that mainly affects females.1 There have been reported cases with associated inflammatory bowel disease, both Crohn’s disease3 and ulcerative colitis.4 Rosacea fulminans may be complicated by erythema nodosum.5
Diagnosis
Despite the severity of the skin inflammation in patients with rosacea fulminans, there are no systemic symptoms. Typically, no infective organisms are found in the bacterial and fungal cultures of the affected skin. Histopathological examination of skin lesions should be performed in patients for whom Sweet's syndrome is suspected. Biopsies of rosacea fulminans are not diagnostic in themselves, usually showing extensive lymphocytic infiltrate with perifollicular accentuation, mainly in the dermis and extending to the subcutis. Eosinophils, foreign body giant cells and granuloma formation, collagen necrosis and fibrosis have also been described.6 Patients are otherwise well and further blood tests or investigations are therefore not usually indicated.
Management
Patients with rosacea fulminans should be under the care of a dermatologist and early referral is advised. Treatment is initiated with oral prednisone (0.5 to 1.0 mg daily for one to two weeks) to settle the inflammation. Isotretinoin (0.2 to 0.5 mg/kg daily for three to four months) is then introduced while the prednisone is tapered. Recovery may take up to six months.7 MT
References
- Ferahbas A, Utas S, Mistik S, Uksal U, Peker D. Rosacea fulminans in pregnancy: case report and review of the literature. Am J Clin Dermatol 2006; 7: 141-144.
- Plewig G, Jansen T, Kligman AM. Pyoderma faciale: a review and report of 20 additional cases: is it rosacea? Arch Dermatol 1992; 128: 1611-1617.
- McHenry PM, Hudson M, Smart LM, Rennie JAN, Mowat NA, White MI. Pyoderma faciale in a patient with Crohn’s disease. Clin Exp Dermatol 1992; 17: 460-462.
- Dessoukey M, Omar MF, Dayem HA. Pyoderma faciale: manifestation of inflammatory bowel disease. Int J Dermatol 1996; 35: 724-726.
- Akhyani M, Daneshpazhooh M, Ghandi N. The association of pyoderma faciale and erythema nodosum. Clin Exp Dermatol 2007; 32: 275-277.
- Ormond P, Rogers S. Case 3. Pyoderma faciale (PF) (rosacea fulminans). Clin Exp Dermatology 2003; 28: 107-108.
- Firooz A, Firoozabadi MR, Dowlati Y. Rosacea fulminans (pyoderma faciale): successful treatment of a 3-year-old girl with oral isotretinoin. Int J Dermatol 2001; 40: 203-205.