What’s new in menopausal hormone therapy: combination oestrogen–bazedoxifene

Menopause
Hormone replacement therapy
A product combining conjugated estrogens with the selective oestrogen receptor modulator, bazedoxifene, rather than a progestin is a recent new option for postmenopausal women with an intact uterus seeking relief from menopausal symptoms.
The publication of data from the combined hormone replacement therapy arm of the Women’s Health Initiative (WHI) in 2002 led to a stunning rejection of menopausal hormone therapy (MHT) for the treatment of symptoms of the menopause.1 Harms were said to be excessive and benefits few. Those early and dramatic claims of excessive harm broadcast by the WHI investigators have now been largely replaced by a much more considered position, which confidently states that when MHT is prescribed for healthy, recently postmenopausal women, its benefits far outweigh its risks. International guidelines and position statements all concur.2,3
The current position is based on much new research as well as a thorough reassessment of data from the WHI trials, taking into account the effects of patient age, years since the menopause, concurrent disease and, most significantly, the differences seen in outcomes for women using either the combined conjugated estrogens (CE) plus progestin regimen or the oestrogen-only regimen in the trials.4
Although the original interpretation of the WHI data has been rightly criticised, and the original findings in many cases overturned, these randomised trials remain a remarkable repository of data on the effects of MHT on postmenopausal women’s health. The data, stratified for age or years since the menopause, show minimal harm and maximum benefit for women starting MHT within 10 years of the menopause. Adverse effects increase with age, time since the last menstrual period and, strikingly, with regard to cardiovascular health and breast cancer risk, also in the combined MHT arm compared with the oestrogen-only arm. It is now clear that although the addition of a synthetic progestin (medroxyprogesterone acetate in the WHI) to CE protects the endometrium, it attenuates the cardiovascular benefits seen with CE alone. It also changes breast cancer risk, from a reduced risk for CE alone compared with placebo to a borderline increased risk for CE combined with medroxyprogesterone acetate.
Data from French observational studies and the UK General Practice Research Database support this proposition and also show that the use of micronised progesterone instead of a synthetic progestin provides a much better safety profile.5
Developing a tissue-selective oestrogen complex
The realisation that the addition of a progestogen to MHT potentially increases adverse events and attenuates oestrogen-related benefits has led researchers to look for other ways to protect the endometrium. An obvious choice is a selective oestrogen receptor modulator (SERM).6,7
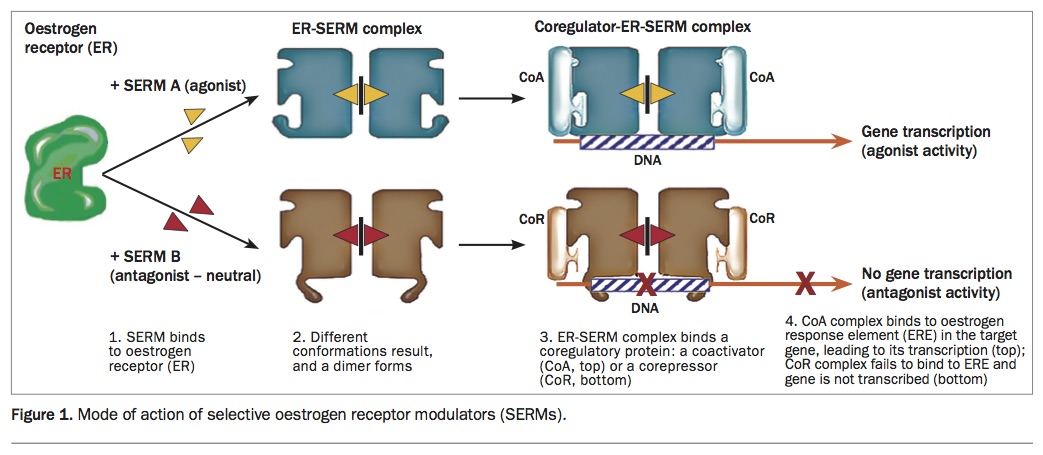
SERMs are a class of drugs that act only on oestrogen receptors. However, unlike pure oestrogen receptor agonists and antagonists, SERMs exert different effects in different tissues, allowing them to be agonists in some tissues and antagonists in others. First-generation SERMs such as clomifene and tamoxifen stimulate the endometrium, but newer SERMs such as raloxifene, lasofoxifene (not available in Australia) and bazedoxifene attenuate the proliferative effects of oestrogen on the endometrium (Figure).
{kind=link}
SERMs do not alleviate vasomotor symptoms (in fact, they may cause them); however, their selective mode of action allows some to have oestrogenic effects in some systems (e.g. bone) and antioestrogenic effects in the breast and endometrium. This is the case with bazedoxifene.
Combination CE-bazedoxifene
A new form of MHT has become available in Australia. Called a TSEC (tissue-selective oestrogen complex), it is an oral tablet that combines 0.45 mg of CE with 20 mg of a new SERM, bazedoxifene. A progestogen is not required as bazedoxifene adequately attenuates the proliferative effects of CE on the endometrium.
This TSEC combination was decided on after research trialling different doses of CE combined with different SERMs. The combination of CE 0.45 mg with bazedoxifene 20 mg was found to:
- effectively suppress the endometrium
- downregulate oestrogen receptors in the breast
- alleviate vasomotor symptoms
- improve quality of life
- reduce vulvovaginal atrophy
- improve bone mineral density at both the hip and lumbar spine (note that there are currently no data on fracture prevention).
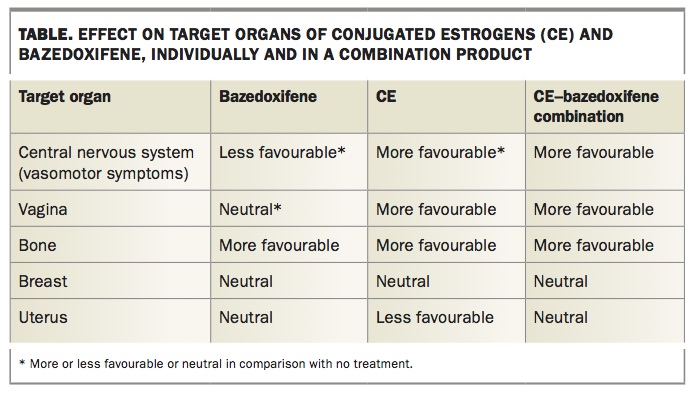
The effects of the components of CE–bazedoxifene and the combination product on target organs are shown in the Table. Combined CE–bazedoxifene, unlike its components, exerts favourable effects on the central nervous system (vasomotor symptoms), vagina and bone while maintaining neutral effects on breast and endometrium.
{kind=link}
Evidence on effectiveness
The CE–bazedoxifene combination, has been the subject of five randomised placebo-controlled trials (RCTs). These Selective Estrogens, Menopause, and Response to Therapy (SMART) trials lasted up to two years and involved over 7500 women.8-12
In the SMART-1 and 2 trials, CE–bazedoxifene significantly reduced the frequency and severity of hot flushes among generally healthy women with moderate to severe vasomotor symptoms at recruitment.8,9 At week 12, CE–bazedoxifene reduced the average daily number of moderate or severe hot flushes by 74% (from 10.3 at baseline to 2.8), compared with 51% for placebo (from 10.5 to 5.4).9
In the SMART-4 trial and a pooled analysis of the SMART-1 and 5 trials,
CE–bazedoxifene was shown to significantly improve bone density at both the lumbar spine and the femur and also to reduce markers of bone turnover.11,13
The SMART-3 trial examined the effect of CE–bazedoxifene on vulvovaginal atrophy.10 This showed the expected histological improvements in the vagina, namely an increase in superficial cells and a decrease in parabasal cells, together with reduced vaginal pain and discomfort plus improved vaginal lubrication and sexual function.
Evidence on safety
Endometrial safety
The key safety issue with a TSEC is endometrial safety. The SMART-1 and 4 trials were designed to monitor the endometrium over one to two years of treatment.
CE–bazedoxifene use was associated with less than a 1% incidence of endometrial hyperplasia, a result similar to placebo. This very low rate satisfies the strict demands of regulatory authorities in the USA, Europe and now Australia. Bazedoxifene prevents endometrial proliferation by blocking the oestrogen-mediated expression of proliferative genes while still maintaining expression of antiproliferative genes. This is different to the action of progestins, which block endometrial proliferation by inducing epithelial differentiation as well as downregulating oestrogen receptors.
In a pooled analysis of all trials, the risk of endometrial cancer for users of
CE–bazedoxifene was not significantly different to that in the placebo group (relative risk [RR] 0.9, 95% confidence interval 0.2 to 4.8).14
Breast cancer risk
The effects of any hormone therapy on breast cancer must be carefully evaluated. Both CE and bazedoxifene have shown good breast safety in clinical trials. In the WHI trials, the use of CE alone for up to 7.8 years was associated with a nonsignificant reduction in breast cancer risk compared with placebo. In a seven-year trial in women with osteoporosis, the use of bazedoxifene alone had a neutral effect on the breast.15
Preclinical studies in rodent models have shown that the addition of bazedoxifene to CE blocks the proliferative effects of oestrogen on terminal bud and lobular gland development.16 In substudies of the SMART-1 and 5 trials, CE–bazedoxifene did not increase breast density or breast pain compared with placebo.8,12 In a pooled analysis of the five SMART trials, the incidence of breast cancer was not significantly different to that in the placebo groups.14 However, these trials continued for only two years, and thus the long-term effect of CE–bazedoxifene on breast cancer risk remains unknown at this time.
Venous thromboembolism
An increased risk of venous thromboembolic events (VTEs) has been reported for both oral oestrogens and SERMs. In the WHI, CE 0.625 mg increased VTE risk (hazard ratio [HR] 1.48, 95% CI 1.06 to 2.07). In postmenopausal women with osteoporosis, bazedoxifene 20 mg for seven years was also associated with increased VTE risk (HR 1.62, 95% CI 0.08 to 3.3).15 In the SMART trials,
CE–bazedoxifene did not show an additive effect, and a pooled analysis of all five trials found no significant increase in VTE risk for CE–bazedoxifene compared with placebo. Given the small number of events and incomplete understanding of the mechanism of the effect, we must conclude that the true risk of VTE with
CE–bazedoxifene remains unknown.
CE–bazedoxifene is contraindicated in women with a history of VTE. Advice to women considered to be at increased risk of VTE (e.g. increasing age, obesity, smoking, prolonged immobilisation) is to use non-oral forms if MHT is required.
Other risks
Vaginal bleeding is a common complaint of women starting traditional MHT. WHI data showed MHT users to be four times more likely to experience vaginal bleeding than nonusers. In contrast, users of CE–bazedoxifene in the SMART trials reported an incidence of vaginal bleeding significantly lower than seen with standard MHT and similar to that in the placebo group.
Adverse mood changes have been reported in some trials of women using combined oestrogen and progestogen therapy. Results for the effects of
CE–bazedoxifene on mood have not been reported, although health-related quality of life scores and menopause-specific quality of life scores were improved compared with placebo in the SMART-2, 3 and 5 trials. Sleep quality and adequacy were also improved.17
Who should use CE-bazedoxifene?
CE–bazedoxifene is indicated for the relief of moderate to severe vasomotor symptoms associated with menopause in women with a uterus. It is an option for any postmenopausal woman with an intact uterus seeking relief from these symptoms at least 12 months after the last menstrual period. CE–bazedoxifene has been shown to significantly and persistently reduce both the frequency and severity of vasomotor symptoms, to improve sleep parameters and quality of life, to increase vaginal lubrication and to reduce vaginal discomfort and dyspareunia. There is also a significant improvement in bone density at both the hip and lumbar spine. Women who have used CE–bazedoxifene report high levels of satisfaction.18
CE–bazedoxifene is a low-dose MHT.Other low-dose MHT options include oral combination estradiol (1 mg) plus a progestogen, and tibolone.19 The key difference between CE–bazedoxifene and traditional MHT is the replacement of a progestogen with a SERM. MHT combinations containing oestrogen plus a synthetic progestin have been associated with an increased risk of breast cancer, increased breast density and pain, and increased vaginal bleeding. Progestin-containing MHT may also have adverse effects on mood. During two years of clinical trials, the incidence of these side effects among users of CE–bazedoxifene was less than that seen with progestin-containing MHT and similar to placebo. Hence, although CE–bazedoxifene is suitable for any postmenopausal woman with an intact uterus, this combination is especially attractive for those who have experienced mood changes, breast pain or tenderness, or vaginal bleeding (after underlying pathology is excluded) when using conventional combined MHT.20 There are no data directly comparing CE–bazedoxifene and tibolone.
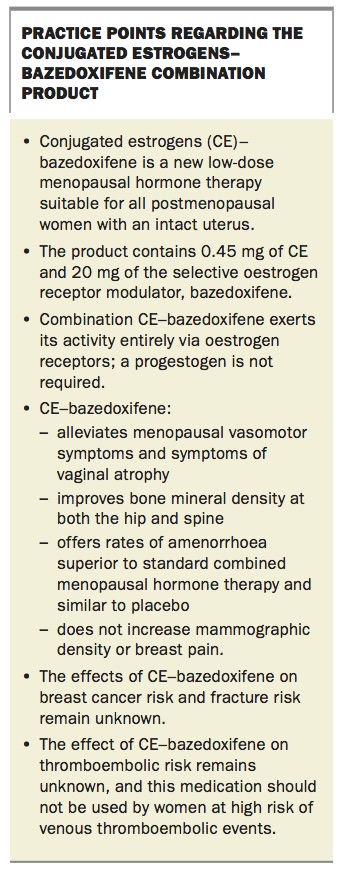
A suggested algorithm for selecting MHT for postmenopausal women in different circumstances is shown in the Flowchart. Practice points on CE–bazedoxifene are summarised in the Box.
{kind=link}
Women being prescribed CE–bazedoxifene, like all women receiving MHT, should have a full health check and risk assessment carried out before commencement; all appropriate screening tests should be performed and they should receive regular follow up at least annually.
Conclusion
CE–bazedoxifene is a new low-dose MHT that is suitable for use by postmenopausal women with an intact uterus. It exerts its activity entirely via oestrogen receptors; a progestogen is not required. It reduces vasomotor symptoms and symptoms of vaginal atrophy, improves bone mineral density at both the hip and spine and does not increase mammographic density or breast pain. Its effects on breast cancer risk, fracture risk and thromboembolic risk remain unknown, and it should not be used by women at high risk of VTE. MT