Regaining trust: managing inadvertent vaccination errors

Medicolegal medicine
Immunisation
This series highlights common medicolegal issues in general practice. Written by a team from medical defence organisation Avant, it is based on actual cases with details changed for privacy and some issues summarised for discussion. This scenario of 20-month-old twins given the wrong vaccine shows the importance of protocols to prevent error and of effective disclosure after an error to restore trust.
Inadvertent errors in the administration of vaccines are consistently among the reasons that GPs contact their medical defence organisations (MDOs) for advice. Vaccination errors that commonly come to our attention include administering the incorrect vaccine, administering an adult dose to a child, administering an out-of-date formulation or using an incorrect technique (e.g. an intramuscular rather than subcutaneous route). As vaccination errors often involve infants, the emotional stakes are high. For GP registrars, this may be the first time they conduct open disclosure with a patient.
In our experience, although patients rarely bring claims for compensation as a result of vaccination errors, they may make a complaint to a complaints body. Receiving a formal complaint can be stressful and confronting for clinicians. A patient’s decision to lodge a formal complaint is often influenced not just by the error but by how the doctor communicates the error and responds to the patient’s concerns. Having a strategy in place for openly and honestly communicating an error is part of good clinical practice and reduces the risk of complaints escalating.
The following case scenario derives from a number of similar claims and calls for medicolegal advice about vaccine administration errors.
Clinical scenario
At midday on Friday, Mrs Black attended a medical centre with her 20-month-old twins, Mary and Jane, for their 18-month immunisations. The family was seen by Dr Smith. Mrs Black explained they had recently moved to the area, and she had been unable to find the twins’ ‘blue books’. Dr Smith examined the twins and checked their vaccination histories through the immunisation register. As the twins were clinically well, he referred them to Registered Nurse Jones for administration of measles, mumps, rubella and varicella (MMRV) live vaccine and diphtheria-tetanus-acellular pertussis (DTPa) vaccine.
In accordance with the vaccination protocol, RN Jones checked the patients’ names and ages and the vaccines’ expiry date before administering the vaccines.
When she was writing up the vaccines, RN Jones realised that rather than DTPa, she had inadvertently administered combined DTPa, hepatitis B, poliovirus and Haemophilus influenzae type B vaccine to both Mary and Jane. As it had been a very busy day, the usual two-person check of the correct vaccine and dosage had not occurred.
RN Jones immediately advised Dr Smith, who contacted the local public health unit (PHU). The PHU advised that no adverse effects were expected.
Mrs Black had already left the practice. RN Jones attempted to contact her but was unable to get through. She left a message on Mrs Black’s mobile phone, asking her to contact the practice.
Mrs Black called the practice at 5:50 pm, 10 minutes before it was due to close. As Dr Smith and RN Jones were both attending to other patients, the practice manager spoke to Mrs Black. She acknowledged the error and apologised for the mistake. She told Mrs Black that Dr Smith had contacted the PHU and there should be no adverse effect to Mary and Jane. Dr Smith had also advised that no further action was required, as the combined DTPa, hepatitis B, poliovirus and H. influenzae type B vaccine contained additional vaccines and would not affect the twins’ future vaccination schedule.
Mrs Black stated that both Mary and Jane were well. She had a number of questions regarding the effect of the additional vaccines. The practice manager reassured Mrs Black that there was no urgency, and that Dr Smith would contact her on Monday to provide the requested information.
At 8:00 am on Monday, Mrs Black phoned the surgery. She was concerned that Mary had developed a mild temperature over the weekend and asked to speak to Dr Smith. The practice manager advised that Dr Smith was due to arrive at 10:00 am, and offered to put her through to another doctor. Mrs Black hung up the phone.
Later that week, Dr Smith received a written complaint from Mrs Black. She said his consultation with her had been rushed and there had been a delay in disclosing the error. She stated he had failed to respond to her concerns and lacked interest in the welfare of her daughters. Mrs Black said she had been very stressed over the weekend and missed work on Monday after her daughter became unwell. She wanted a written apology and changes made to the practice protocols. Mrs Black stated that if she did not receive a satisfactory response she would lodge a formal complaint.
Discussion
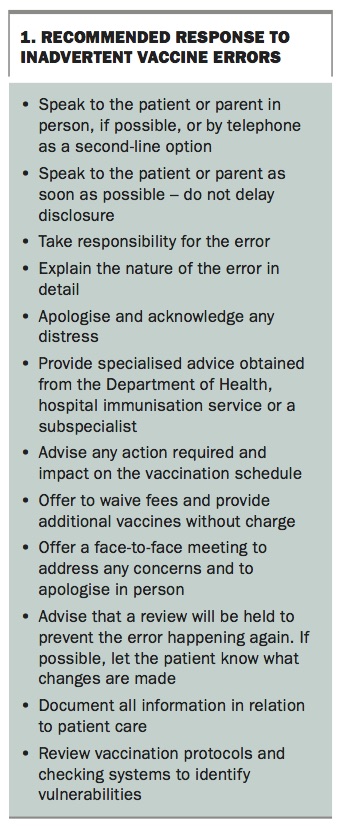
Disclosure of a medical error is a process, not a formula. Successful communication involves openly and honestly acknowledging the error, seeking to understand the patient’s concerns and approaching the incident as an opportunity to refine clinical systems. Recommendations on responding to inadvertent errors are summarised in Box 1.
{kind=link}
Seek advice and information
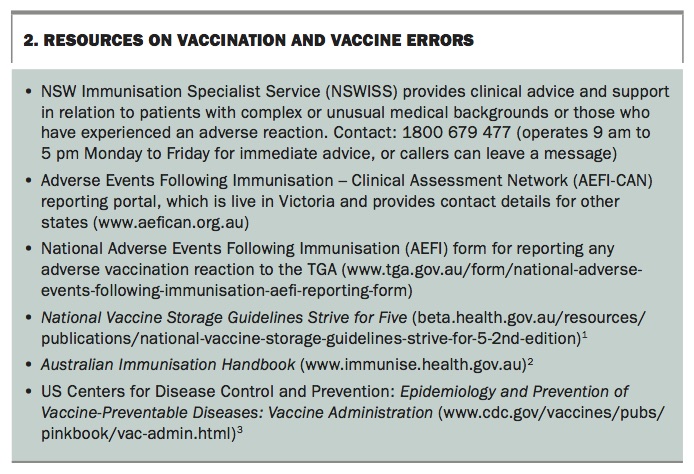
Before contacting the patient, obtain advice on the clinical implications of the error; for a vaccine error this could be obtained from the local PHU or hospital infectious diseases unit. Other useful contacts and resources on vaccination and vaccine errors are listed in Box 2.1-3
{kind=link}
Acknowledge the error
In accordance with the Good Medical Practice: a Code of Conduct for Doctors in Australia, contact the patient promptly and advise that an error has occurred.4 Preferably do this in person rather than over the telephone. Explain the nature of the error, as well as the known facts about how it occurred.
Provide an apology
A key element of accepting responsibility for the error is apologising to the patient. Ideally, all healthcare providers involved in the error should apologise. An apology should include words such as ‘I am sorry this has happened’. An apology should not be seen as an admission of liability, and all Australian jurisdictions have statutory provisions that protect an apology being used in legal contexts.
If you are upset about the outcome, it is appropriate to state this, using words such as ‘this is not the outcome either of us wanted’. However, the patient’s experience and concerns should remain the focus of the discussion.
Discuss potential consequences
Following a vaccination error, patients are usually concerned they are not fully covered or will suffer an adverse reaction from an excess dose, from receiving an additional vaccine or from incorrect administration.
Fortunately, most vaccination errors do not result in an adverse outcome. Fully inform the patient of the specialist immunisation or infectious diseases advice, including any action required and any impact on the vaccination schedule. This is also an opportunity to clarify any misunderstandings the patient may have.
Also provide advice on monitoring adverse outcomes and when to escalate care, particularly if the error occurs before a weekend. If the patient is present, provide a printout of the side effects of the vaccines as a helpful reference. Offer to discuss their concerns again if needed, either in person or by telephone.
Understand the patient’s perspective
Patients may express a range of concerns in addition to the clinical consequences. It is important to listen to the patient to understand what they are really upset about, how this can be addressed and what level of reassurance is required. A defensive response is more likely to result in the matter escalating.
Parents of infants who have been incorrectly vaccinated often express significant anger or distress at the thought that their otherwise well child may have been harmed. They may also be responding to seeing their child suffer. It is important to acknowledge this, even if you consider the level of distress to be disproportionate. Advice on what they can safely do to manage their child’s pain may also help.
A patient who requires re-vaccination may be upset or angry at the inconvenience or cost involved. As a gesture of goodwill, consider offering to waive any fees and to provide additional vaccines without charge.
Advising the patient that a review will be held to improve safety measures demonstrates you are taking the complaint seriously, and that their complaint will make a difference.
When there is significant anger or distress, offer to hold a face-to-face meeting to address any concerns and to apologise in person. It may be appropriate for the practice manager to also attend to discuss any practice or administrative issues. The practice should ensure that patients have access to information about making a complaint.
Maintain clinical records
Ensure you document all information in relation to patient care. If you contact your MDO for advice, record this separately, as it does not form part of the clinical record.
Review systems and protocols
Take steps to address the issue. Review your vaccination protocols and checking systems to identify contributing factors. Refer to the National Vaccine Storage Guidelines – Strive for Five and the Australian Immunisation Handbook.2,3 If possible, let the patient know what changes have been made after the review.
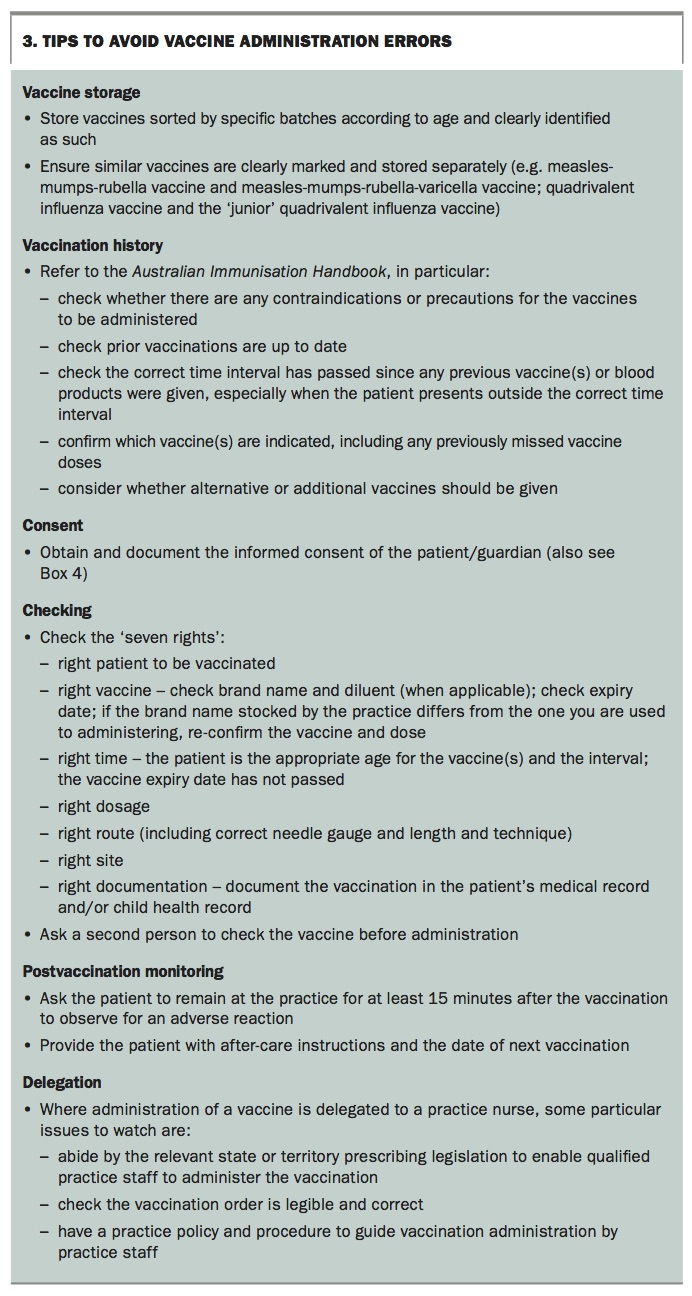
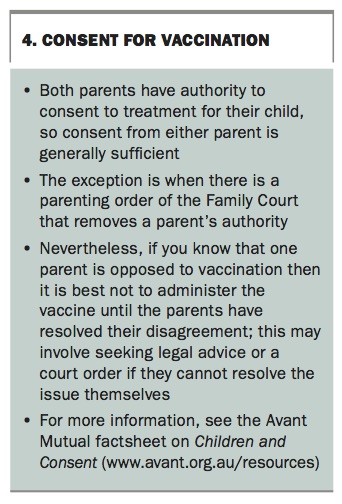
Some tips to avoid common risks are outlined in Box 3 and Box 4, and resources to help manage adverse events and consent in Box 5.
{kind=link}
{kind=link}
{kind=link}
Outcome
Dr Smith drafted a response to Mrs Black. However, he found it difficult to maintain objectivity as he felt Mrs Black was over-reacting. Dr Smith contacted his MDO and requested feedback on the suitability of his response. After discussion with his MDO, Dr Smith wrote to Mrs Black apologising for the error and acknowledging her distress. He acknowledged that being new to the area would have added to her stress. Dr Smith reassured Mrs Black that the twins should experience no adverse effects. He accepted he should have apologised personally to Mrs Black and contacted her the same day to discuss her concerns. Dr Smith confirmed that following a team meeting, changes had been implemented to reduce the risk of the error being repeated.
Mrs Black accepted the apology and did not lodge a formal complaint. Although she declined to see Dr Smith again, she continued to attend the practice for the twins’ medical needs.
Conclusion
Only a small proportion of patients who experience a vaccination error make a formal complaint. A strategy of openly and honestly communicating the error as soon as possible, and attempting to understand the patient’s expectations can positively influence the patient’s decision to make a formal complaint, and minimise the impact of the complaint on you and your staff. Follow up by telephone after the event provides further reassurance and demonstrates care and concern for the child and parent. MT