Early arthritis: a guide to assessment
Arthritis
Joint disorders
In many cases of early arthritis, a specific diagnosis is not possible at presentation and the clinical picture emerges over time. Accurate history, examination and rational investigation are crucial in narrowing the broad list of differential diagnoses. For patients with confirmed rheumatoid arthritis, prompt initiation of therapy will lead to greatly improved outcomes.
- Accurate diagnosis in a patient presenting with joint pain is dependent on thorough history and examination, focusing on the cardinal features of possible causes.
- Early initiation of corticosteroids can be considered in some circumstances, but may obscure subsequent clinical assessment by a second practitioner.
- If symptoms persist, referral to a rheumatologist within six weeks (if seropositive), or up to 12 weeks (if seronegative), is imperative.
- Referral to an emergency department for urgent assessment of possible septic arthritis is appropriate, or if there are worrying abnormalities in the vital observations (e.g. tachycardia, fever, hypotension, hypoxia).
Early arthritis and recent-onset arthritis are synonymous terms that are indicative of an underlying inflammatory joint disease, the likely cause of which is yet to be defined. There are many causes of early arthritis. Pattern recognition through accurate history, examination and appropriately targeted investigation is the key to navigating this broad list of differential diagnoses. For most types of arthritis, the diagnosis is based on the clinical picture, which may evolve over time. Hence, accurate diagnosis in the early stages may not always be possible.
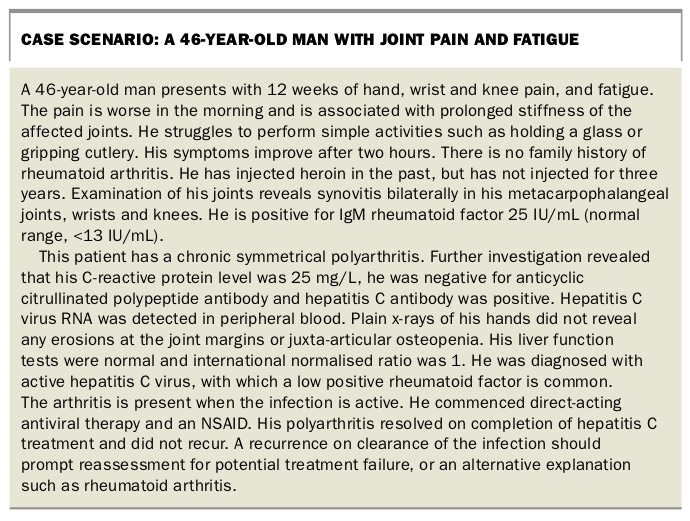
In many patients, early treatment with corticosteroids can obscure and delay the diagnosis. In the case of early rheumatoid arthritis (RA), treatment during the ‘window of opportunity’, meaning commencement of therapy as soon as the diagnosis has been made with certainty, leads to better outcomes for the patient.1 The purpose of this article is to provide a guide to the initial assessment of a patient presenting with joint pain. The clinical case study in the Box illustrates how the approach presented here can assist in making a diagnosis.
{kind=link}
Defining arthritis, arthralgia and periarticular pain
The terminology used is important in accurately communicating the synthesis of history and examination findings and will aid in narrowing the list of differential diagnoses. ‘Arthritis’, implying joint inflammation, is used when the classic features of inflammation are confirmed on history with the physical examination revealing both joint swelling and tenderness. The joint swelling is caused by synovitis and synovial effusion and typically has a ‘boggy’ feel on palpation. ‘Arthralgia’ is used when the history indicates joint pain but joint swelling is not seen on physical examination. In some patients, such as those with osteoarthritis, there may be mild inflammatory symptoms that are not prolonged (e.g. early morning stiffness lasting less than 30 minutes) and the joints display ‘bony’ swelling, or none at all, as well as tenderness, all still consistent with arthralgia. ‘Periarticular’ is used to describe pain arising from structures external to the joint capsule, but anatomically close to the joint. In most instances this is due to tendon-related pathology such as tendonitis or tenosynovitis.
Initial assessment
Time course
The time course of arthritis will alter the pretest probability of various conditions. An acute-onset arthritis (symptoms evolve in less than 48 hours) particularly with a monoarthritic presentation, can be caused by septic arthritis, crystal-associated arthritis (e.g. monosodium urate [MSU] crystal arthritis [gout], calcium pyrophosphate crystal arthritis [pseudogout]), haemarthrosis and occasionally other types of inflammatory arthritis that more typically present with polyarthritis over several weeks (e.g. RA, reactive arthritis or psoriatic arthritis). The most important of these is septic arthritis. Untreated septic arthritis can lead to rapid joint destruction or even death. A recurrent arthritis characterised by intervening periods of resolution is typical of MSU crystal arthritis. A chronic arthritis (lasting for more than six weeks) is more typical of untreated RA or psoriatic arthritis. In the case of chronic monoarthritis, chronic infection is more likely, particularly in an immunosuppressed patient. Synovial tissue biopsy and culture is the most important diagnostic procedure in such cases.
Type of joint pain
The cardinal symptoms of inflammatory joint pain are:
- worse after periods of inactivity
- (e.g. upon waking after sleeping all night)
- associated with prolonged (more than 30 minutes) stiffness of the affected joints
- improves with use of the joint
- improves with application of heat and NSAIDs
- may be associated with constitutional symptoms of inflammation such as weight loss and fatigue.
These symptoms may be accompanied by the cardinal physical findings of inflammation, such as erythema, warmth, tenderness on palpation and reduced range of motion.
In contrast, mechanical joint pain is characterised by pain that improves on resting, worsens with use (particularly weight bearing) and is associated with minimal or short-lived stiffness (less than 30 minutes and often less than 15 minutes). Mechanical joint pain is typical of osteoarthritis and periarticular pathology.
Distribution of the affected joints
Three categories define the number of joints affected:
- monoarticular (single joint)
- oligoarticular (two to four joints)
- polyarticular (five or more joints).
Typically, monoarthritis affects large joints (ankles, knees, hips, shoulders, wrists), as does oligoarthritis. Polyarthritis can involve both large and small joints. In the case of oligo- and polyarthritis, joints on both sides of the body may be affected. It is ‘symmetrical’ when joints in the same region are affected (e.g. metacarpophalangeal [MCP] joints two and three on the left hand and four and five on the right hand, not necessarily a mirror image of each other) and ‘asymmetrical’ when they are only affected on one side. Symmetrical arthritis is associated with RA, some presentations of psoriatic arthritis, crystal arthritis (when chronic) and connective tissue diseases (Figure). Asymmetrical arthritis is usually associated with spondyloarthritis and crystal arthritis.
{kind=link}
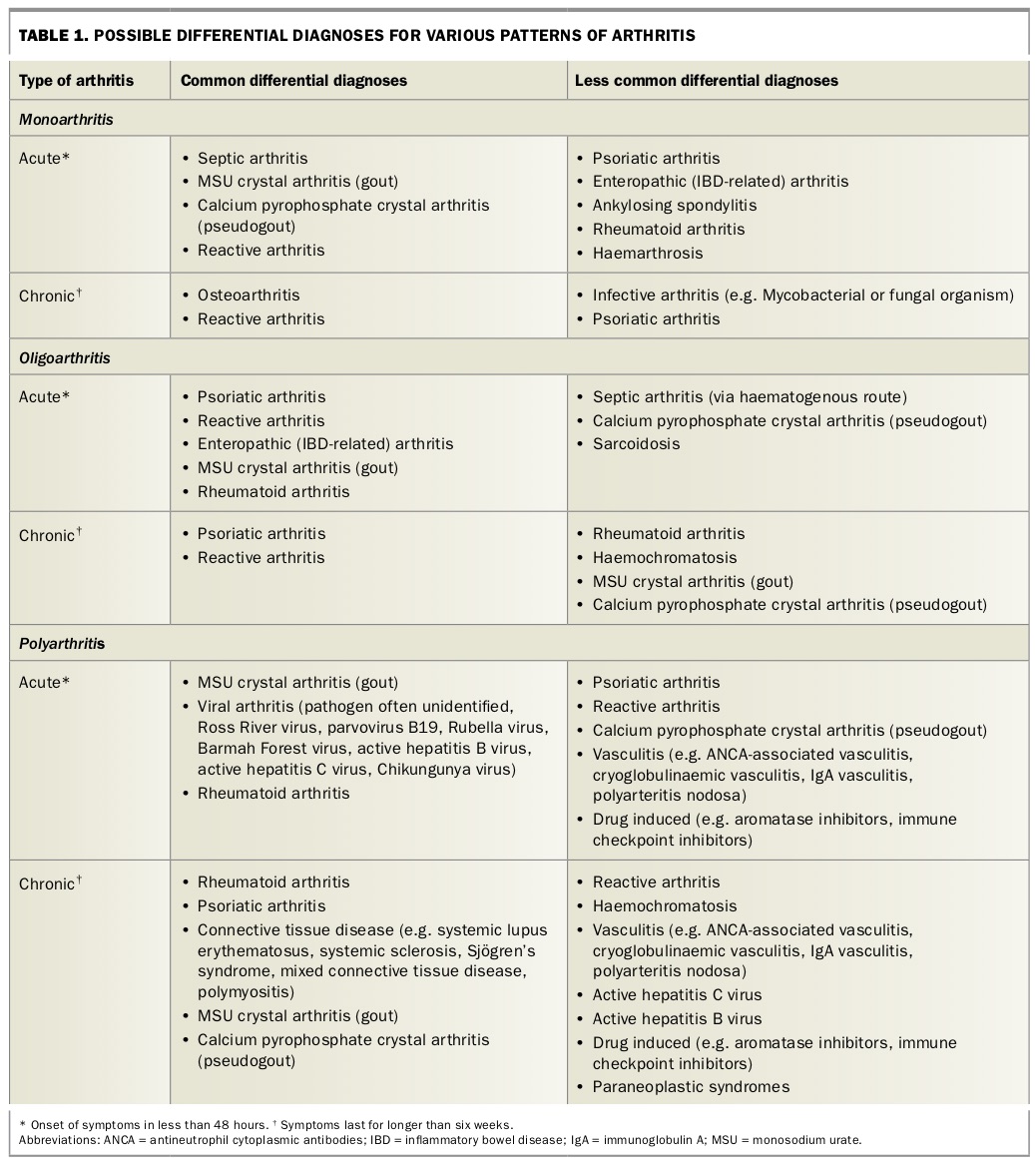
Using a combination of the joint distribution and time course, the differential diagnoses can be narrowed. Table 1 is not exhaustive, but provides an idea of the most likely differential diagnoses according to these parameters. Note the considerable overlap between the causes of mono-, oligo- and polyarthritis.
{kind=link}
Extra-articular clues
Identification of additional relevant symptoms and risk factors that occur with each of the various causes of arthritis in Table 1 will guide clinicians in prioritising their list of differential diagnoses and subsequent investigation. Patients with RA may have visible rheumatoid nodules, particularly near the elbows and on the hands. Women and smokers are more commonly affected and there is often a family history. Patients with gout might have tophi evident, and are typically (although not exclusively) older men.
Patients with spondyloarthritides will often have a history of acute anterior uveitis, inflammatory lower back pain, dactylitis (fusiform swelling of digits) and/or enthesitis. Each of the various spondyloarthritides have additional diagnostic features, such as the presence of chronic plaque psoriasis, nail psoriasis or a family history of psoriasis (for psoriatic arthritis), symptoms suggestive of inflammatory bowel disease (for enteropathic arthritis), or a recent history of acute gastrointestinal or genitourinary symptoms, or possibly a sexually transmitted infection (e.g. Chlamydia trachomatis) for reactive arthritis.
Patients with septic arthritis might present with features of sepsis, but in many cases there are no alterations in vital signs. This is particularly true in patients who are immunosuppressed. A high index of clinical suspicion is essential in any patient with an acute arthritis on such treatments. Some pathogens are known to cause a monoarthritis without any other features of sepsis, particularly Mycobacterium tuberculosis. It is not necessary for there to be concurrent pulmonary tuberculosis. When a chronic monoarthritis is present, infection must always be considered.
Connective tissue diseases (e.g. systemic lupus erythematosus, systemic sclerosis, Sjögren’s syndrome, mixed connective tissue disease, polymyositis) usually have additional features evident on history or examination, such as Raynaud’s phenomenon, photosensitivity, history of pericarditis or pleuritis, or muscle weakness.
Viral arthritis might result from active hepatitis B or C virus, or from other arthritogenic viruses (e.g. parvovirus B19, Barmah Forest virus, Ross River virus, Chikungunya virus). A history of possible exposure to hepatitis B or C virus (e.g. past intravenous drug use, recurrent blood transfusions before 1990) should prompt direct testing for confirmation of active infection.
Sarcoidosis can present with a classic triad of hilar lymphadenopathy, oligoarthritis of the ankles and erythema nodosum (so-called Lofgren syndrome). Vasculitis-associated arthritis will often have associated purpura, peripheral neuropathy and involve other vital organs (particularly the kidneys, lungs and eyes). Rarely, arthritis due to a paraneoplastic syndrome is identified by a comprehensive history and examination and targeted investigations.
Investigations guided by differential diagnoses
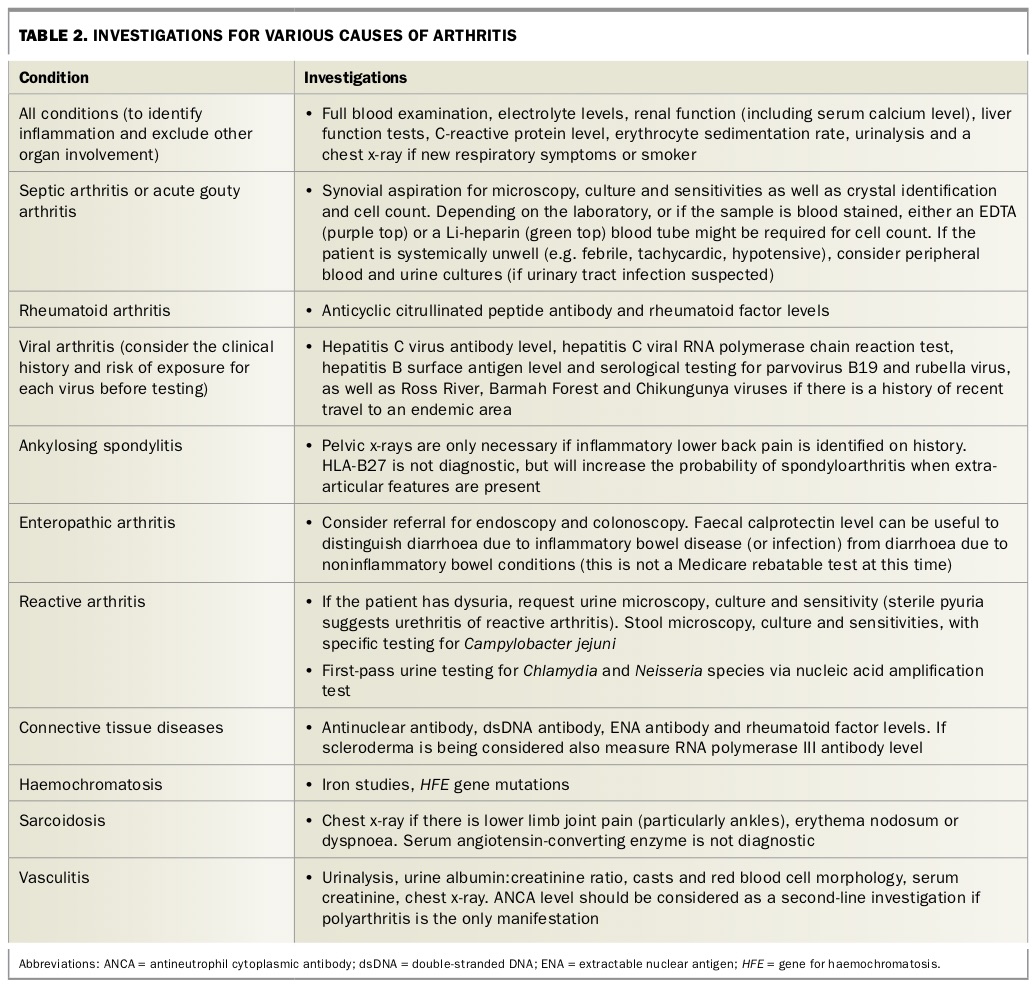
Additional testing is guided by the list of differential diagnoses (Table 2). Each set of investigations is a guide only and should only be done in the appropriate clinical context (i.e. they are not all required for every patient).
{kind=link}
A plain x-ray of the affected region is usually normal when the process is acute. In chronic arthritis, it may show evidence of erosive changes with or without bone remodelling. The distribution of erosive change can support a specific diagnosis (e.g. marginal erosions of the MCP joints on both hands suggests RA).
Referral
Is an emergency referral required?
Referral to an emergency department is required if a patient has deranged vital signs (e.g. tachycardia, fever, hypotension, hypoxia) or if septic arthritis is suspected. Recent-onset polyarthritis is an indication for referral for rapid review by a rheumatologist, although does not necessarily require assessment in an emergency department.
Referral to a rheumatologist
Referral to a rheumatologist should be made in the following circumstances:
- suspected RA, connective tissue disease, spondyloarthropathy, crystal arthritis, sarcoidosis or vasculitis
- diagnostic uncertainty despite investigation of persistent features of inflammatory disease.
RA with positive antibodies to cyclic citrullinated peptides and/or positive rheumatoid factor (so-called seropositive RA) is more likely to have an aggressive natural history with more erosions, deformity and disability compared with seronegative disease. When RA is strongly suspected, it is essential to refer patients early (within six weeks if persistent and seropositive or within 12 weeks if seronegative) to a rheumatologist, as early initiation of treatment can markedly improve outcomes. GPs should be alert to an insidious or stuttering onset, particularly of polyarthritis, as such patients often have a worse prognosis and specialist assessment is particularly valuable.
How to fast track early review
Where available, refer patients to the local network HealthPathways to determine the preferred means of fast-track referral to public hospital rheumatology clinics. Alternatively, contact the rheumatologist (public or private) directly by phone.
Symptom relief before specialist review
Advice on symptom relief before assessment can be obtained through phone contact with a rheumatologist, although in general the treatment choices should reflect the severity of the symptoms.
Paracetamol and judicious use of NSAIDs are useful first-line choices for early arthritis with mild-to-moderate symptoms. They do not alter the underlying pathology and should provide analgesia, although often incompletely. Long-term use should be avoided. The addition of fish oil (1 to 3 g three times daily) can be a useful anti-inflammatory adjunct in the longer term.
Corticosteroids usually improve arthritis of any severity, but should be reserved for severe symptoms with impairment in function. Corticosteroids will limit detailed physical assessment by a rheumatologist and subsequently may obscure the diagnosis. Use of corticosteroids is best considered once definitive evidence is obtained for a diagnosis, or after discussion with a rheumatologist if specialist assessment is required. Corticosteroids are usually then weaned once symptom control with disease-modifying antirheumatic drugs (DMARDs) is achieved. Occasionally, patients may continue to self-medicate with oral corticosteroids beyond the recommended dose and duration, potentially leading to adverse events. Parenteral formulations of corticosteroids are a reasonable alternative and can be administered intramuscularly or intravenously at an ambulatory care facility. Opiate analgesia is not recommended.
Conclusion
Early arthritis has a broad list of differential diagnoses. A thorough history, accurate examination and appropriately targeted investigations are the key to narrowing the list. Symptoms can be managed with simple analgesia in the first instance. Corticosteroids can obscure assessment by a second clinician. Identification and emergency referral of septic arthritis is essential, and early referral of patients with RA will lead to earlier therapy and better outcomes. MT