Gout – can we prevent ongoing attacks?

Gout
Arthritis
Gout is a common form of inflammatory arthritis, seen more often in men and increasing in prevalence with age. The diagnosis can be made on a typical history of recurrent episodes or crystal identification using polarised microscopy.
Case scenario
Mr Liew is a 50-year-old Chinese man who presents to the medical centre for the third time in two years. A diagnosis of gout in his right first metatarsophalangeal (MTP) joint was made at each previous presentation. He requests colchicine at this visit (as he was prescribed this previously). Mr Liew’s uric acid level (initially measured two years ago) was raised at 0.46 mmol/L (reference range, 0.20 to 0.42 mmol/L) and his kidney function was normal. Mr Liew drinks 20 g of alcohol (red wine) daily and up to 60 g daily on weekends. He works as a stockbroker and has a stressful job; he does not always stop to eat and drink when at work. There is no family history of gout.
Mr Liew wants to know if there is any way to prevent his recurrent gout. He also wants to know why he has it and why it has started at this stage in his life. What is the likelihood of his children getting gout? How important is diet in the prevention of gout? How relevant is his alcohol intake in the development of his gout?
Commentary
Gout is the most frequent inflammatory arthritis seen in men (recent Australian prevalence estimates between 2.67% and 11% of men and between 0.53% and 2.4% of women 25 years of age and older).1,2 It increases in prevalence with age in both men and women, and initially presents in the first MTP joint in 50% of cases. Psoriatic arthritis, osteoarthritis, acute calcium pyrophosphate arthritis and calcific (hydroxyapatite) peri-arthritis can also cause recurrent pain and swelling in the first MTP joint.
Diagnosis
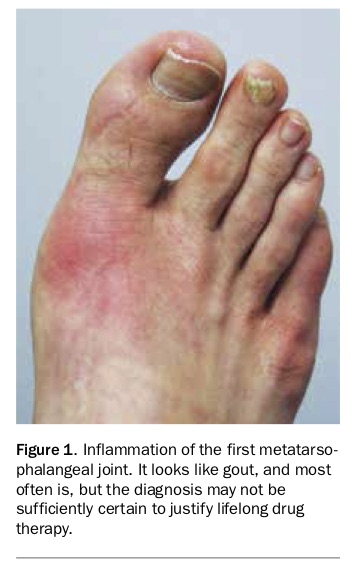
Aspiration of the swollen joint followed by immediate examination of the synovial fluid using polarised light microscopy is the gold standard for confirmation of the diagnosis. As the tiny amount of fluid obtained from an MTP joint dries rapidly, the time between aspiration and examination should be less than 30 minutes. Typical clinical features in combination allow a high level of diagnostic certainty, but in less typical cases it is often appropriate to defer a decision regarding lifelong, urate-lowering therapy until the diagnosis is confirmed (Figure 1).3 Typical features include:
{kind=link}
- first MTP joint, ankle or midfoot involvement
- erythema, marked tenderness, great difficulty walking
- time to maximal pain less than 24 hours, resolution in less than 14 days
- complete resolution between episodes
- tophus (Figure 2)
- elevated serum urate.
{kind=link}
Dual-energy CT scans can detect urate deposits in soft tissues and joints and has good (not perfect) specificity but lacks sensitivity for a patient with a history of only three episodes. Urate crystal deposition can be identified on ultrasound by hyperechoic irregular enhancement of the articular surface of the hyaline cartilage (double contour sign), hyperechoic aggregates suggestive of tophi within the joint or along tendons, and floating hyperechoic foci within the joint space (which have the appearance of a snowstorm). The technique requires an experienced observer and is not (yet) a reliable tool in practice in Australia.
To check diagnostic/classification confidence, visit http://goutclassificationcalculator.auckland.ac.nz.
Treatment of the acute episode
NSAIDs, corticosteroids (oral, parenteral or intra-articular) or colchicine are the readily available options, and all are effective. Comparative studies are few and small but prednisone 30 mg daily for five days was found to be of equal efficacy to indomethacin 50 mg three times daily for two days then 25 mg three times daily for three days.4 The best option depends on the patient’s comorbidities, especially hypertension, renal disease (avoid NSAIDs) and diabetes (avoid corticosteroids). If colchicine is used, a low-dose regimen consisting of 1 mg initially, 0.5 mg one hour later (presuming normal renal function) and no more for 24 hours, was as effective and less toxic than the previous higher-dose regimen.5 It is reasonable to then continue 0.5 mg twice daily. Mr Liew requests colchicine at this visit (and he has normal renal function) and thus presumably he found it effective and tolerable previously; there is no reason to change his approach to the acute episode.
Why did Mr Liew develop gout?
Although most people with serum urate concentrations above saturation (about 0.41 mmol/L) do not have gout, a persistently elevated serum urate level is required for urate crystal formation and is the driving force behind the disease. Monosodium urate monohydrate (urate) crystal formation is a slow process (months to years) and does not directly cause symptoms. Interaction between the inflammatory system and the crystals is responsible for the clinical manifestations, including the acute episode.
Mr Liew suffered gout primarily because he had persistent hyperuricaemia over many years, which allowed urate crystal growth. Impaired renal clearance, mainly determined by genetically influenced function of anion transporters in the proximal renal tubule, is the primary mechanism in more than 90% of hyperuricaemic patients (with or without gout). The onset in middle age is common, reflecting the gradual increase in serum urate levels with age and the slow growth of urate crystals that precedes the first attack.
Will dietary change help?
Obesity, excess alcohol intake and dietary factors (high intake of fructose, meat, seafood, Western dietary pattern) are associated with hyperuricaemia and gout. Improving these factors in the community (and in his sons, who have about twice the background risk of developing gout6) should reduce the future prevalence of gout. A recent review of weight loss for control of gout in overweight and obese individuals concluded that the current evidence consists of few studies of low methodological quality.7 In a prospective, randomised, cross-over feeding trial the DASH diet (based on a high intake of fruits, vegetables, nuts, legumes, low-fat dairy products and whole grains, and low intake of sweetened beverages and red and processed meats) reduced serum urate levels by an average of 7% (0.02 mmol/L); insufficient to achieve target levels.8 Alcohol reduction and, if Mr Liew is overweight, weight reduction would be reasonable recommendations, but we do not have evidence that focussing on diet will be of practical use for control of his gout.
Effective management
As is often encountered in clinical practice, Mr Liew and his GP are interested in the role of diet, alcohol and hereditary factors. Prevention of ongoing attacks and joint damage will be determined by whether Mr Liew can maintain his serum urate levels below saturation in the long term. His target serum urate levels is less than 0.36 mmol/L; if he had tophi it would be less than 0.30 mmol/L. The only way this is likely to be achieved is through the use of urate-lowering therapy, which will be needed life-long. Allopurinol is the best first option for most people, but in Han Chinese people, if HLA-B58:01 is present the risk of allergy would make febuxostat a good choice. For the first six months of urate-lowering therapy prophylaxis against flares is required (e.g. colchicine 0.5 mg twice daily). If colchicine is not tolerated, a low-dose NSAID should be considered. Urate-lowering therapy (regardless of specific drug) should be commenced at a low dose and titrated up (monthly intervals is reasonable) until serum urate levels are persistently below target. If allopurinol 600 mg daily or 900 mg daily fails to achieve target, a uricosuric agent should be added (probenecid, losartan or fenofibrate, depending on the patient’s comorbidities). Rarely, the combination of a xanthine oxidase inhibitor (allopurinol or febuxostat) and benzbromarone (the most potent uricosuric agent currently available and requires TGA Special Access Scheme approval) is required to achieve target levels. Benzbromarone should only be used by clinicians with experience in the drug.
Conclusion
The key messages for Mr Liew are that: ‘cure’ of his gout is possible; maintaining his serum urate levels persistently below target levels (less than 0.36 mmol/L) is required; drug therapy is the reliable way to achieve target levels; and if target levels are difficult to achieve, referral to a rheumatologist is indicated as almost all patients can achieve target levels with appropriate escalation of therapy. MT