Rectus sheath haematoma: it’s not just a cough

Abdominal pain
Differentiating rectus sheath haematoma from other causes of abdominal pain can be difficult and identifying risk factors can help.
Case scenario
As you are coming to the end of a long Friday evening shift, you see one final patient: an 88-year-old man presenting with left anterolateral rib pain that started the previous night after a coughing fit. He has had influenza-like symptoms for three days. However, when you see the patient, his symptoms have altered. He describes pain in the left lower quadrant of his abdomen that radiates up to his chest when he coughs.
The patient has had symptoms of an upper respiratory tract infection for two weeks, mainly a sore throat and nonproductive cough. Over the past week, he has been noticing an increasing dull aching pain in the left lower quadrant of his abdomen as he coughs. He became concerned today when the pain began radiating to the left upper quadrant of his abdomen, so he presented to hospital. The pain is worsened by movement, particularly when changing position from sitting, standing and lying down. The pain is relieved when he lies down or stands straight. He describes one episode of associated light-headedness, but no change to his bowel habits, no weight loss, nausea or vomiting, and his appetite has not altered. He has been feeling hot and cold occasionally (with no confirmed fevers) but assumed this was due to his upper respiratory tract infection. He has never had any abdominal surgery.
The patient has a history of hypertension, hypercholesterolaemia, prostate cancer, osteoarthritis and lumbar disc prolapse corrected by discectomy. His regular medications include paracetamol 1 g three times daily, simvastatin 20 mg at night, telmisartan 80 mg in the morning, spironolactone 12.5 mg in the morning and aspirin 100mg on alternate days. He has no known allergies. He lives alone in a single-level townhouse and is fully independent: he drives to the bowls club two to three times a week, but only plays now and again. Since his back operation he uses a stick when he mobilises for long periods of time.
Physical examination
On examination, the patient is afebrile and his vital signs are stable. He looks generally well. He is able to transfer from the chair to the examination table, but it clearly exacerbates his pain. He has a large abdominal girth that is longstanding and there is some minor bruising around his umbilicus.
There is a tender firm palpable mass, about 12 x 6 cm in size, in the left lower quadrant of the patient’s abdomen. Bowel sounds are present. There are no other peripheral stigmata of gastrointestinal disease. He has an erythematous throat and a postnasal drip, but there are no other abnormalities on respiratory or cardiovascular examination.
Provisional diagnosis and test results
You perform a venous blood gas analysis, which shows no abnormalities. The rest of his blood test results come back with the following abnormal results:
- creatinine level is elevated at 130 mcmol/L
- urea level is 9 mmol/L, so he is uraemic
- white cell count is 16 x 109/L and neutrophils are 11.4 x 109/L, showing neutrophilia
- C-reactive protein level is elevated at 19 mg/L
- haemoglobin level is 104 g/L, so he is anaemic.
He had routine blood tests at his GP three days ago and the results showed a white cell count of 11 x 109/L and a haemoglobin level of 11 g/L. His levels of lipase, calcium, magnesium, phosphate and other electrolytes as well as his liver function test results are within normal ranges. The results of a urinalysis are normal.
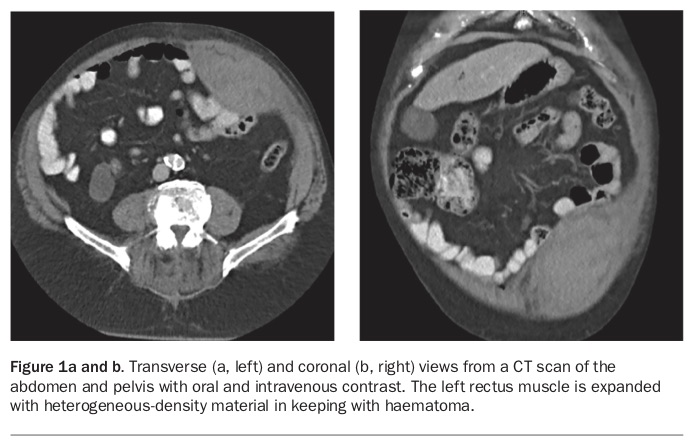
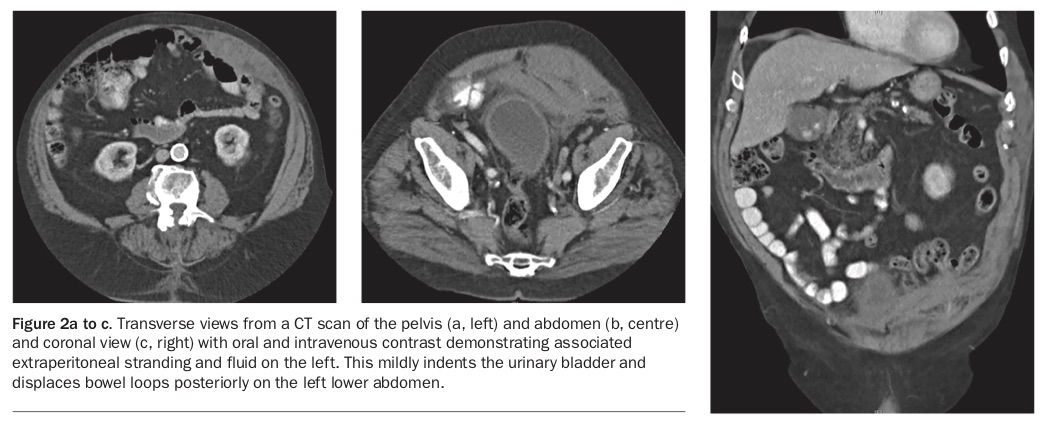
A chest x-ray shows no abnormalities. A CT of his abdomen was performed (Figure 1) and shows that his left rectus muscle is expanded with material of heterogeneous density, in keeping with a haematoma. There is associated extraperitoneal stranding and fluid on the left side of his abdomen, which mildly indents the urinary bladder and displaces bowel loops posteriorly in the left lower abdomen (Figure 2). He is diagnosed with a left rectus sheath haematoma.
{kind=link}
{kind=link}
Management
The patient is given analgesia and his aspirin is ceased. He is started on oral antibiotics and given a cough suppressant.
Given his history of abdominal pain and a palpable mass, he is initially reviewed by the surgical team. After the CT scan result is reviewed he is admitted to the care of the geriatricians. During his hospital admission his bruising is monitored and it spreads bilaterally towards his flanks over the next 72 hours. His haemoglobin level decreases to 78 g/L on day one of his admission, but on further monitoring it does not drop any further. He receives a transfusion of one unit of packed red blood cells.
The patient’s acute kidney injury is treated by withholding his nephrotoxic medications (i.e. telmisartan and spironolactone) and he is given careful intravenous hydration. His renal function improves to normal limits on the next day. He is encouraged to maintain oral hydration at all times.
He is discharged three days later and has no further complications.
Discussion
This is a relatively typical presentation of a very rare disease. Rectus sheath haematoma often mimics acute intra-abdominal disease and is difficult to differentiate from other intra-abdominal pathologies. It is therefore best diagnosed with a CT scan of the abdomen.
Although rare, there are several risk factors for rectus sheath haematoma (Box). These are mainly linked to a mechanism of injury (e.g. coughing, trauma) or exacerbation of presentation (e.g. anticoagulation, small rectus sheath muscle mass in women or elderly people leading to reduced ability to tamponade bleeding). Anticoagulation is one of the most common risk factors associated with the development of a spontaneous rectus sheath haematoma.1 Other comorbidities associated with rectus sheath haematoma are hypertension, atherosclerosis and abnormal clotting such as in cirrhosis and renal disease.
{kind=link}
Rectus sheath haematoma usually presents as a sudden onset of abdominal pain with a palpable mass.2 It is unusual in this case that the patient had not noticed the mass. If severe, a large rectus sheath haematoma can present with sudden onset of pain and either hypotension or a decrease in haemoglobin levels, which can be a further diagnostic challenge. This further enforces the need for a CT scan of the abdomen before a laparotomy if the condition is suspected on history and examination.
On examination, it can be difficult to differentiate rectus sheath haematoma from other causes of abdominal pain and masses. The mass is usually in the lower abdomen because the haematoma is caused by disruption of the inferior epigastric artery as it inserts into the rectus abdominis muscle at the arcuate line. At this point the inferior epigastric artery is relatively fixed within the muscle – making it the point for disruption.3 There is also limited ability to tamponade bleeding anatomically at this point.
There are two signs that are reported to be helpful in differentiating rectus sheath haematoma from other causes, but neither are sensitive or specific. These signs are Carnett’s sign and Fothergill’s sign. Carnett’s sign enables you to detect whether the pain is originating from the abdominal wall or the intra-abdominal organs. It has been shown to be 95% specific for an isolated abdominal wall process.4 To perform the test, the patient lies supine and the point of maximum tenderness is located on palpation of the abdomen. The patient is then asked to raise their head off the bed, and sit up as much as possible while the previously identified most tender point is palpated. If the tenderness is worse the test is said to be positive and the pain is likely to be originating in the abdominal wall. This manoeuvre is supposed to alleviate the pressure from the intra-abdominal viscera therefore alleviating the pain. Other causes of a positive Carnett’s sign include myositis, muscle strain and nerve entrapment.5 Fothergill’s sign is positive if the intra-abdominal mass does not cross the midline and does not change with leg movement.
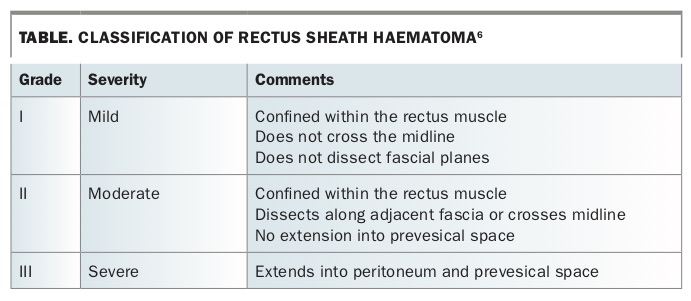
Treatment for rectus sheath haematoma is guided by grade of injury (grade I to III) and comorbidities.6 The CT scan of the abdomen is used to determine the grade of injury (Table) and if visualised then a CT angiography is performed to identify active bleeding. Most patients present with grade I rectus sheath haematomas and are managed conservatively. Conservative management includes analgesia, rest, ice treatment, reversal of anticoagulation if appropriate, and intravenous fluid resuscitation and blood transfusion if required.2 It is important to monitor haemoglobin levels with serial measurements.
{kind=link}
Management of grade II and III rectus sheath haematomas is further divided based on whether the patient is haemodynamically stable or unstable. If they are haemodynamically stable, treatment should be conservative but with increased monitoring and possibly follow-up CT angiography. If the patient is haemodynamically unstable, they should be resuscitated with early use of blood products and any anticoagulation should be reversed as per guidelines. A CT angiography (if not already performed) will identify the rectus sheath haematoma and help identify the site and severity of any active bleeding. If available, angiographic embolisation should be facilitated early.
Surgical intervention is only rarely required when the patient is unstable and embolisation has failed or in the presence of a significant abdominal compartment syndrome.7 Surgery may ligate the bleeding source, but will also cause the loss of tamponade to the haematoma and expose extensive sheared surfaces that may continue to bleed and ooze and require packing. This then precipitates a second operation to remove these packs when the patient’s clinical status has improved.
The most serious complications from rectus sheath haematoma are haemorrhagic shock and abdominal compartment syndrome. Mortality increases with anticoagulation from 4 to 25%. Mortality is also increased by two to three times in pregnant women.8
Conclusion
Rectus sheath haematoma, can be a mild or life-threatening disease. It is helpful to carefully consider the possibility of rectus sheath haematoma when an abdominal mass is found with risk factors in the patient’s history. MT