‘headspace’ and GPs – working together to improve young people’s lives

Child mental health
Adolescent mental health
Most mental disorders start in adolescence or early adult life. Early detection and holistic treatment are crucial. GPs, working in partnership with specialist youth mental health services such as headspace, have an important role to play in supporting young people experiencing a mental health condition.
- Mental health conditions typically start in adolescence or early adult life. Left untreated these conditions can have serious personal and social impacts.
- Early detection and holistic treatment reduce the likelihood of adverse outcomes and promote recovery.
- GPs working in partnership with specialist mental health services have a major role to play in supporting young people experiencing a mental health condition.
- GPs are able to refer young people to headspace for assessment and management of common mental health conditions such as depression and anxiety.
- GPs play a crucial role in the headspace model. They are a key source of referral to headspace centres and also a key workforce within centres.
Mental health conditions are a major public health issue. These conditions typically start early in life: 50% of lifetime disorders emerge by 14 years of age and 75% by 24 years of age.1 In Australia, the recent Young Minds Matter survey found that one in seven children and adolescents between 4 and 17 years of age had experienced a clinically significant mental health condition in the 12 months before the survey; and the 2007 National Survey of Mental Health and Wellbeing found that 26% of young people between 16 and 24 years of age had experienced a mental disorder in the 12 months before interview.2,3 The personal, social and economic impacts of these conditions are significant. Mental health conditions are distressing, potentially disabling and associated with premature death from suicide and chronic disease. Together with substance use disorders, they account for 12% of the burden of disease in Australia, third after cancers and cardiovascular disease.4
About headspace
In recognition of the impact of mental health conditions on young people’s lives, the Australian government launched headspace, the National Youth Mental Health Foundation, in 2006. Its mandate was to raise awareness about youth mental health conditions; promote help-seeking and early detection; provide youth-friendly, comprehensive and integrated services to young people between 12 and 25 years of age; and build the capacity of those working with young people through workforce development and support for evidence-based practice.5 Its focus is on early intervention to reduce or prevent the negative impacts that mental health conditions have on young people’s lives now and in the future.
The headspace centres are the cornerstone of this initiative. There are currently more than 100 headspace centres located in metropolitan, regional and rural locations across Australia. Each headspace centre is expected to provide four core activity streams: mental health, alcohol and other drug, physical health and vocational assistance.6 Funding is provided by the Australian Government to Primary Health Networks, which are responsible for commissioning lead agencies to provide headspace centre services. Centres are operated by lead agencies in collaboration with a local consortium of youth-focused services. Oversight is provided by headspace National. Each centre is expected to adhere to the core components of the headspace model under a licencing deed and credentialing system managed by headspace National.7 These core elements include 10 service components (youth participation, family and friends’ participation, community awareness, enhanced access, early intervention, appropriate care, evidence informed practice, four core streams, service integration, supported transitions) and six enabling components (national network, lead agency governance, consortia, multidisciplinary workforce, blended funding, monitoring and evaluation).6
Services offered at headspace
The staffing profile at headspace varies from centre to centre but broadly speaking, staff disciplines include psychology, social work, youth work, general practice, nursing and psychiatry. In line with the blended funding model, some headspace staff are employed on a salaried basis through the Primary Health Networks grant to the lead agency. Others are engaged as private practitioners who co-locate within the headspace centre and work within the parameters of the headspace model. Most of these private practitioners bulk bill the young person using a relevant Medical Benefits Schedule item. In many instances, nongovernment and state and territory-funded youth-focused services, such as drug and alcohol or specialist mental health services, also co-locate staff at the headspace centre to create a ‘one-stop shop’ model.8
Young people access headspace centres in a range of ways including self-referral, referral by family and friends, and referral from GPs, school-based staff or staff in local youth services. Young people who access a headspace centre undergo a comprehensive assessment, which is based on the HEADSS assessment tool (Box 1).9 At every occasion of service, young people complete questions from the headspace minimum dataset that includes questions relating to the young person’s pathway to care, presenting issues and clinical and functional status (e.g. Kessler Psychological Distress Scale [K10], MyLifeTracker). Service providers complete information on clinical and functional status (e.g. Social and Occupational Functioning Assessment Scale [SOFAS]).10 This information is used to develop a management plan and to monitor the young person’s outcomes during their contact with the centre.
{kind=link}
Who accesses headspace services?
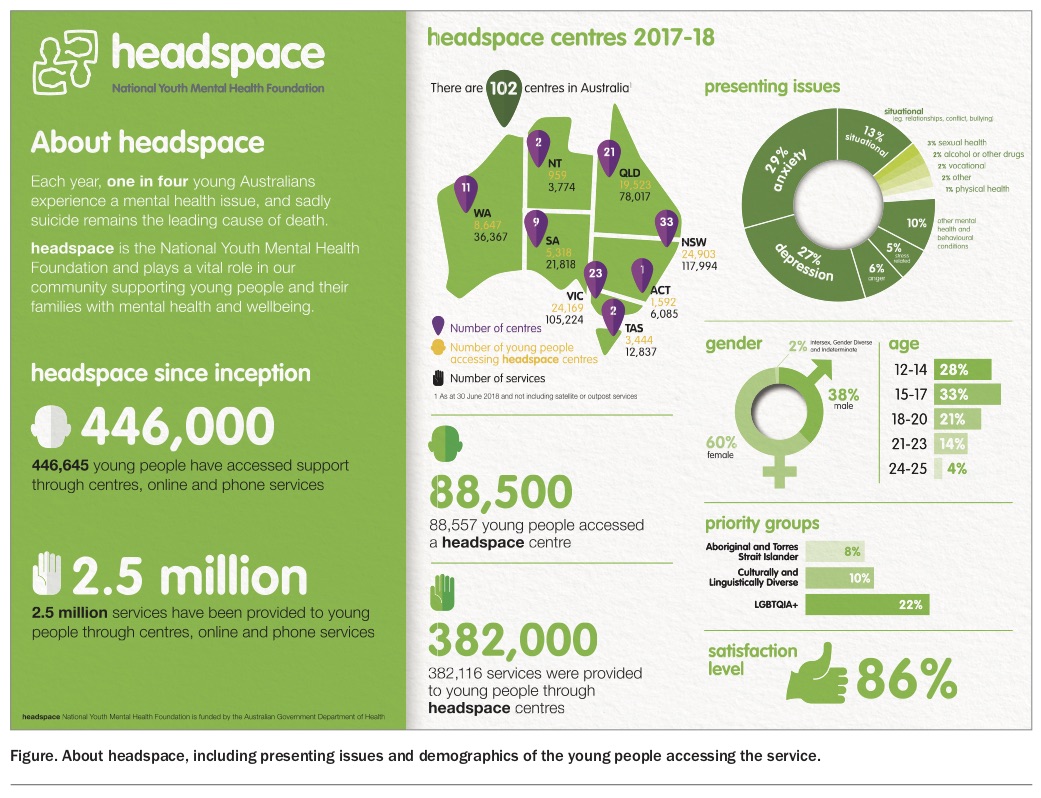
By mid-2018, more than 450,000 young people had accessed headspace services (Figure). About 88,500 young people visited a headspace centre during the 12-month period from July 2017 to June 2018. In that period, 38% of service users were male, 60% were female and 2% were gender diverse. The mean age of service users was 16.9 years. Centres are well utilised by vulnerable groups. Although the proportion of Aboriginal and Torres Strait Islander young people utilising headspace services varies between centres, overall about 8% of young people accessing headspace services identify as Aboriginal and/or Torres Strait Islander, well above the proportion of Aboriginal and Torres Strait Islander people in this age bracket. About 10% of young people accessing services are from a culturally and linguistic diverse background and 22% identify as LGBTQIA+. Young people living in nonmetropolitan centres are also well represented among those accessing services.10
{kind=link}
Presenting issues and treatments offered
Most young people who present to a headspace centre are experiencing a mental health condition or behavioural issues, rather than a physical health, alcohol or other drug or vocational issue.11 The two most common conditions are anxiety (29%) and depression (27%).11 Other presenting problems include situational issues (relationships, bullying and conflicts), anger issues, stress, sexual health, alcohol and other drug problems, and suicide-related behaviour (Figure).
Most young people who access headspace centres receive a mental health service, generally in the form of psychological therapy provided by psychologists or other allied mental health workers. The predominant form of therapy is cognitive behaviour therapy.12 Other modalities include general and supportive counselling, psychoeducation (including skills training and relaxation strategies), interpersonal therapy, acceptance and commitment therapy, mindfulness-based therapies, motivational interviewing and problem solving therapy.12 Many centres provide services for family members and friends of the young person, including Single Session Family Consultation. Other services include alcohol and other drug services, physical and sexual health services, and vocational support. Telepsychiatry services are also available and enable staff in some rural and remote locations who do not have a psychiatrist on site to access this support via a secure videoconferencing platform.
Client outcomes
Young people’s outcomes are generally favourable. A review of routine data collected on headspace clients between 1 April 2013 and 31 March 2014 found that among young people for whom there was relevant data, self-reported psychological distress (measured through pre-post K10 scores) was significantly reduced in 36% of young people and reliably improved in 26%.12 Similar patterns were seen on the pre-post clinician-rated SOFAS scores where 31% of clients showed reliable improvement and 37% showed a significant improvement.12 Overall, outcomes on the K10 or SOFAS improved for about 60% of young people, particularly for those who engaged well with the service and had multiple sessions. Nevertheless, as occurs in all mental health services, a subgroup showed no improvement and some young people showed signs of deterioration.7,13
The role of the GP in making referrals
Young people are not always confident or comfortable in accessing assistance from mental health services. Several barriers to help-seeking have been identified in the research literature. These include low levels of emotional or mental health literacy, preference for self-reliance, lack of trust, concerns about privacy and confidentiality, stigma that generates embarrassment or shame, lack of confidence in health or mental health professionals, the efficacy of mental health treatments, low levels of knowledge of available services, cost and transport barriers, and lack of access to available services.8,14
Although many young people in distress turn first to their friends and family, GPs are also a major port-of-call and therefore have a crucial role in recognising and supporting young people with a mental health condition. Providing a youth-friendly environment, seeing a young person on their own or with a trusted friend or family member, reassuring the young person about privacy and confidentiality while explaining its limits, being genuine and empathic as well as unhurried and nonjudgemental all help to build rapport and therapeutic engagement.15,16
Having a structure for the consultation is also important and the HEADSS assessment framework provides a useful way of exploring a young person’s psychosocial concerns as well as risk and protective factors in their home, school, work and social environments.9 A risk assessment is essential. Although it is not always easy to gauge the level of suicidality, it is crucial to ask whether a young person is experiencing suicidal thoughts, whether they have a plan and whether they have access to means, as this will influence the management plan and the urgency of any potential referral.17
Who can be referred?
Given headspace’s focus on early intervention, GPs are encouraged to refer all young people between 12 and 25 years of age who are at risk of or who have an emerging or newly diagnosed mental health condition, particularly those with depression and anxiety conditions. Although young people with an established high-prevalence mental health condition or those with more complex conditions such as eating disorders, personality disorders or psychoses are eligible to access headspace centres, a referral to a state or territory-funded specialist mental health service may be more appropriate. Since 2015, a limited number of headspace centres across Australia have established a Youth Early Psychosis Program that offers services for young people with a first-episode psychosis or at very high risk of developing psychosis; there are currently 14 such sites (Box 2). Young people who are at high or imminent risk of suicide should be referred to emergency services, hospital emergency departments or a state or territory-funded specialist child and adolescent, youth or adult mental health service, depending on their age.
{kind=link}
In addition to their primary focus on mental health conditions, headspace centres also provide general health services, in particular sexual health (subject to availability of a GP or sexual health nurse) as well as services and supports for young people with substance use issues and/or study and work issues. The headspace initiative is supported by two major online services: eheadspace (a telephone, text and online chat-based service staffed by mental health clinicians) and the Digital Work and Study Service, which provides online vocational support for young people with mental health issues.
Making a referral
GPs play a crucial role in the headspace model. They are one of the key sources of referral to headspace centres (and one of the key workforces within centres). GPs may refer young people in a range of ways. Ideally, the GP should contact the headspace centre by telephone and speak to the intake worker to provide details about the young person and their presenting issues, giving clear reasons for the referral (e.g. diagnostic assessment, psychological treatment). In addition, GPs should provide a written referral to the centre (some centres have referral templates available on their websites). The referral may be provided to the young person with the contact details of the local headspace centre with advice to them, or their supporters, to contact the centre for an appointment. Although some centres accept fax referrals, this is not the ideal mechanism. Most headspace centres do not have encrypted online or email referral systems.
When making a referral and where indicated, GPs are encouraged to provide the young person with a Mental Health Treatment Plan as this will enable them to access headspace services using Medical Benefits Schedule rebates. Once a referral is received and assessment is completed, best practice is for the headspace centre staff to keep the referring GP informed and involved in the young person’s treatment.
Confidentiality issues
Most young people who attend a headspace centre are willing for their parents or caregivers to be involved in their treatment, as long as their own views and independence are respected. In some cases, however, a young person may not want their family informed or involved in their care. Although legislation varies between Australian jurisdictions, young people 16 years of age and older are generally able to give informed consent for medical treatment without parental consent (and legally able to do so from 18 years of age). Young people less than 16 years of age may, in some circumstances, be able to consent to treatment without parental consent if they are assessed as being sufficiently mature and competent to do so (mature minor).18
Clinicians at headspace centres routinely try to involve a young person’s family and friends in their care and attempt to work through any concerns that a young person may have with respect to confidentiality or family conflicts. However, if the young person refuses and is old enough or mature enough to make this decision, the clinicians are required to respect their decision.
GPs working at headspace
GPs are an important part of the headspace workforce. About 75% of centres have GPs working on site, typically on a part-time basis. Other headspace centres have forged close working relationships with GPs working in the local area. Young people greatly value having GPs involved in their care at headspace.13 GPs bring a holistic management approach across mental, physical and sexual health as well as managing alcohol and other drug issues. They provide essential medical services, and can be a less-stigmatised ‘soft-entry’ point to mental health care. GPs working at headspace are ideally well integrated into the multidisciplinary team, including access to team meetings and supervision. Any GP interested in working in a headspace centre or in close collaboration with a headspace centre should contact their local centre (https:// headspace.org.au/headspace-centres).
Resources for GPs
In recognition of the important role played by GPs and other health professionals, headspace National has developed education and training programs and evidence-based resources to equip frontline workers to better engage, assess and assist young people with a mental health condition. These include free, accredited online training modules and clinical resources (Box 2).
Conclusion
It has been said that there can be no health without mental health. Mental health care is an integral part of health care and all health professionals have a role to play. Given the significant interconnections between physical health and mental health, it is important that people have access to holistic services that take an integrated approach to service provision. headspace centres are a one-stop shop for young people between 12 and 25 years of age where they can have their health and psychosocial needs addressed together through a multi-disciplinary team-based approach. GPs are a crucial part of the headspace model and young people value being able to access their services. By working within a headspace centre or having a close working relationship with a centre, GPs can make a significant contribution to improving young people’s lives. MT