Premature ovarian insufficiency. Not ‘too young for menopause’

Dr Xu is a Diabetes and Reproductive Registrar in the Department of Endocrinology, Monash Health, Melbourne. Associate Professor Vincent is an Endocrinologist in the Department of Endocrinology, Monash Health, Melbourne; and Head, Early Menopause Studies, Monash Centre for Health Research and Implementation–MCHRI, School of Public Health and Preventive Medicine, Monash University, Melbourne, Vic.
Women's health
Premature ovarian insufficiency, which is defined as loss of ovarian activity before the age of 40 years, has negative health impacts. Prompt diagnosis, evaluation of cause and sequelae, psychological support and institution of hormone replacement therapy are essential components of management.
Premature ovarian insufficiency (POI), also known as premature menopause or premature ovarian failure, is defined as the loss of ovarian activity before the age of 40 years.1 It may occur spontaneously or secondary to medical treatments. Management should incorporate consideration of symptoms experienced, psychological health and desire for fertility, as well as the long-term sequelae related to bone and cardiovascular health. Hormone replacement therapy is recommended until the age of natural menopause.
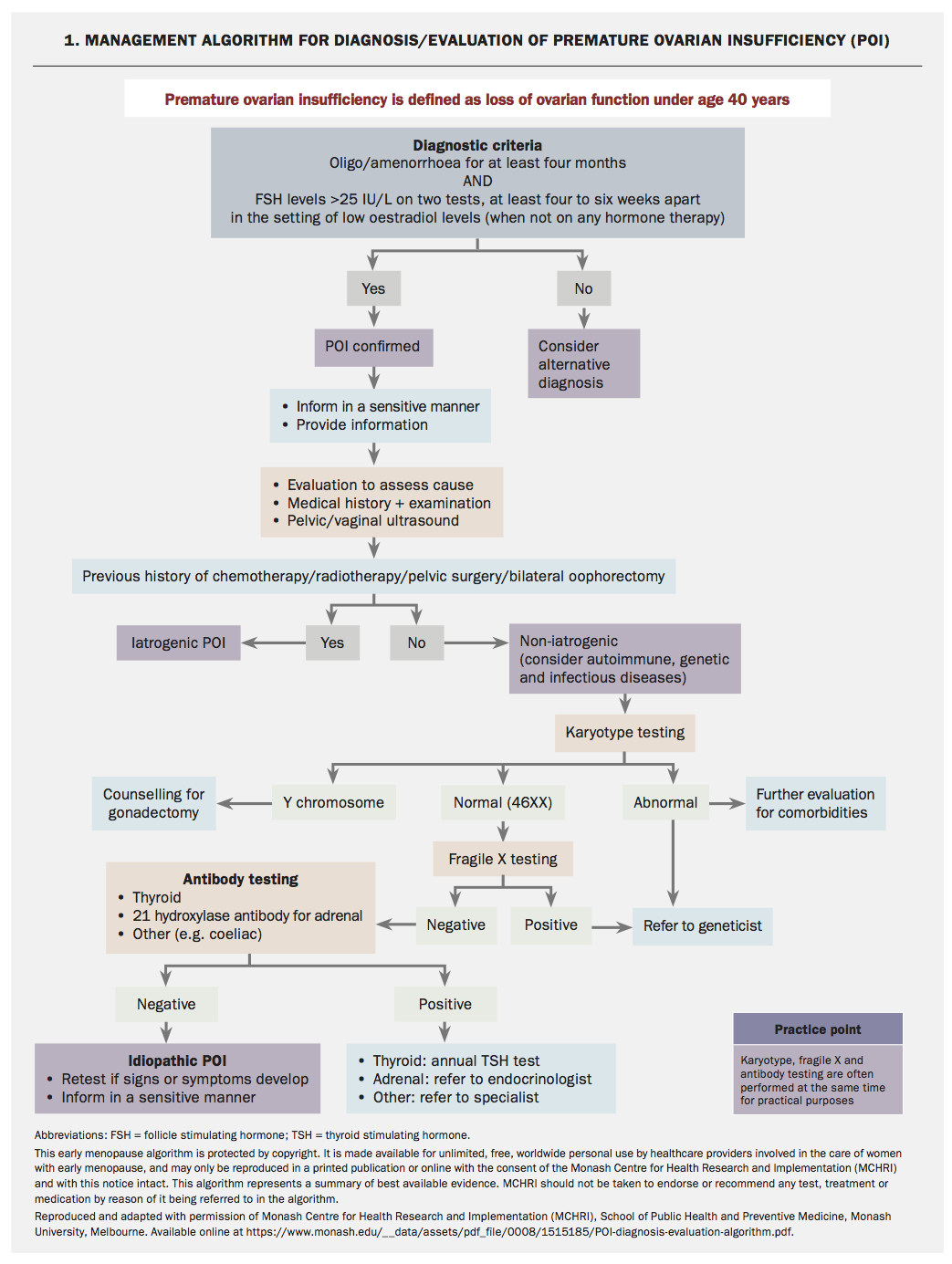
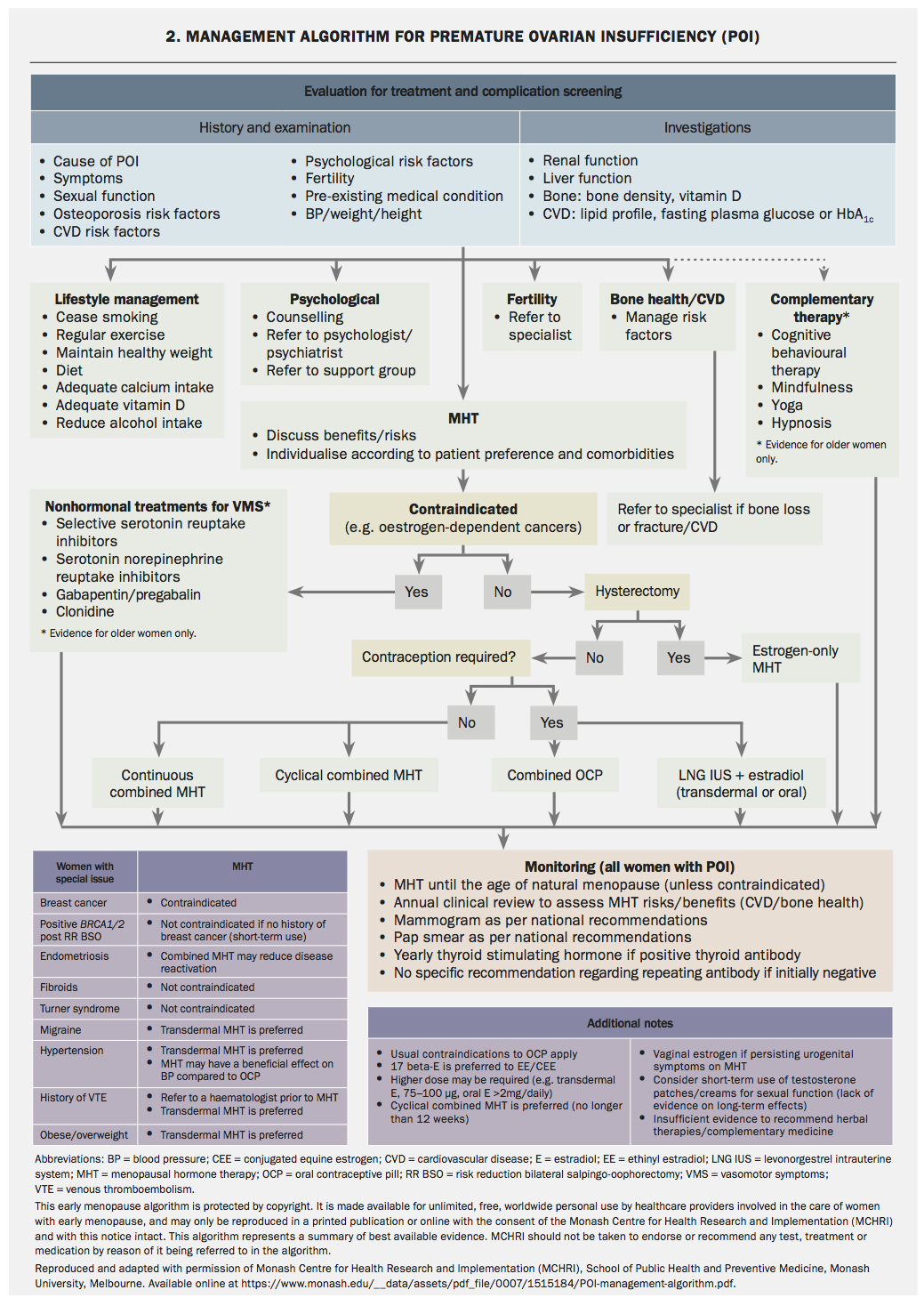
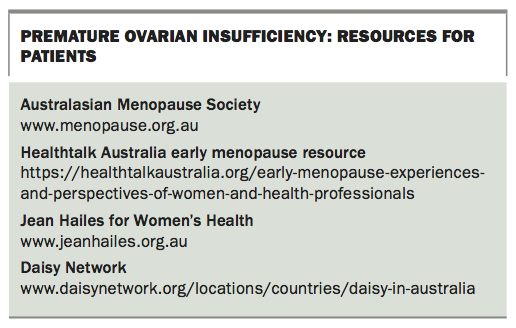
Resources are available to assist with the care of women affected by POI developed by Monash Centre for Health Research and Implementation, Melbourne (MCHRI), and available online (https://healthtalkaustralia.org/early-menopause-experiences-and-perspectives-of-women-and-health-professionals). These include algorithms for the diagnosis and evaluation and for the management of POI, which are based on a systematic search of menopause guidelines, AGREE (Appraisal of Guidelines for Research and Evaluation) evaluation and extraction of recommendations related to POI. The algorithms are shown on pages 57 and 58.
{kind=link}
{kind=link}
Terminology
The term ‘menopausal hormone therapy’ (MHT) is now preferred when referring to estrogen and progestin preparations for managing menopause. However, the term ‘hormone replacement therapy’ (HRT) is used in this article for women with premature ovarian insufficiency (and is also used in the European Society of Human Reproduction and Embryology [ESHRE] guideline),1 as this reflects the fact that in this setting women are using preparations to replace hormones that would normally be produced by the ovaries. In addition, some young women find the term MHT less appealing than HRT.
Case scenario
Karima is a 35-year-old woman who presents to her GP with an eight-month history of amenorrhoea, hot flushing, hair loss and loss of libido that is affecting her relationship with her husband. She and her husband have two daughters but have been hoping to have more children, particularly as in their culture a son is very much desired. Karima is a nonsmoker and does not drink alcohol. She does not take any medications and has no previous medical or surgical history.
What investigations should be performed to determine the cause of Karima’s secondary amenorrhoea?
Although the most common causes of secondary amenorrhoea are pregnancy, polycystic ovary syndrome and hypothalamic or pituitary disease, POI should also be considered in a young woman with oligo – or amenorrhoea. Spontaneous POI affects approximately 1% of women.
Diagnostic criteria for POI are oligo – or amenorrhoea for at least four months and FSH levels in the postmenopausal range (>25 IU/L) on two tests performed at least four to six weeks apart (Flowchart 1).1-3 Women should not be taking hormonal medication at the time of testing. Anti-Müllerian hormone (AMH) testing is not recommended for the diagnosis of POI, although it is used by specialists for fertility assessment.1,2
Karima’s initial investigations include a negative pregnancy test and show normal TSH and prolactin levels. Her FSH is elevated (68 IU/L and 101 IU/L) and her oestradiol low (86 pmol/L and 76 pmol/L) on two occasions, six weeks apart, confirming the diagnosis of spontaneous POI.
What could be the cause of Karima’s POI and what investigations should be performed?
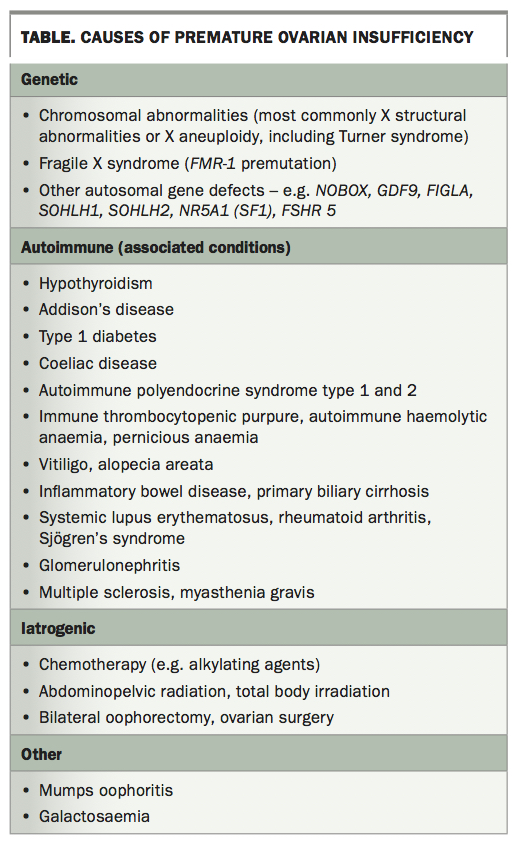
Known causes of POI include genetic, autoimmune and infectious diseases and iatrogenic factors (Table). Iatrogenic POI is becoming more common with advances in cancer treatment and risk-reducing bilateral oophorectomy. The risk of iatrogenic POI depends on a patient’s age, type and dose of chemotherapy, and dose and field of radiotherapy.4 Most cases of POI are unexplained or idiopathic and may reflect gene mutations that currently are not readily detected.5
{kind=link}
Chromosomal abnormalities are found in 10 to 12% of women with POI, and may cause primary or secondary amenorrhoea.6,7 If Y chromosomal material is detected then there is an elevated risk of gonadoblastoma, and gonadectomy is usually advised.8 Sporadic and familial fragile X (FMR-1) premutation has been reported in up to 7.5% and 13% of Caucasian women with POI, respectively, but it is less prevalent in Indian women and Chinese women with POI.1,9,10 The presence of this mutation has implications for a woman’s offspring and other family members. If any genetic abnormalities are detected then the woman should be referred to genetic services.
On exclusion of genetic causes, an autoimmune screen should be performed, including 21-hydroxylase antibody (21OH-Ab) or adrenocortical antibodies for adrenal autoimmunity and anti-thyroid peroxidase antibodies (TPO-Ab). If 21OH-Ab is positive, the woman should be referred to an endocrinologist for further assessment of adrenal function. If the woman is TPO-Ab positive, TSH should be measured yearly because of the increased risk of hypothyroidism secondary to Hashimoto thyroiditis.
In practice, karyotype, fragile X testing and autoantibody testing may be requested at the same time. Ovarian antibody testing is nonspecific and is not recommended. Testing for other autoimmune disorders may be indicated depending on initial history and examination.
What are the initial steps in the management of Karima’s symptoms and concerns?
POI can be a devastating diagnosis for many women, especially when it is unexpected and no underlying cause has been found. Early referral to psychology services and support groups (e.g. Daisy Network) may be beneficial (Flowchart 2). In addition, careful assessment for depression or anxiety is important. Lifestyle recommendations for women with POI are directed at menopausal symptom control, cardiovascular disease risk reduction and bone health. Women should be given appropriate information or referred to good quality resources – examples of useful websites are given in the Box.
{kind=link}
Baseline investigations are directed at determining choice of hormone replacement therapy, assessing fertility, and evaluating cardiovascular and osteoporosis risk. They include renal and liver function, pelvic ultrasound, AMH level, lipid profile, fasting plasma glucose, calcium, phosphate and vitamin D measurements and bone mineral density (BMD) scanning. Cervical screening should be up to date.
When and how should hormone replacement therapy be prescribed?
Recommendations for HRT in women with POI (Flowchart 2) are derived from observational studies and small clinical trials of women with POI due to Turner syndrome, bilateral oophorectomy or chemotherapy, or idiopathic in origin, and from evidence in women experiencing menopause at the usual age. As well as being the most effective treatment for vasomotor symptoms, HRT has been shown to improve genitourinary symptoms, sleep and emotional wellbeing. HRT is also important for long-term health by reducing the risk of cardiovascular disease, cognitive dysfunction and osteoporosis.11-13
HRT ameliorates the impact of POI on bone health, and has beneficial effects on cardiovascular and metabolic health, including lowering blood pressure and improving endothelial function and lipid profile.14-22 In women with Turner syndrome, HRT has been shown to improve liver function and increase lean body mass.20,23,24
HRT is recommended for women with POI until the average age of natural menopause (51 years); however, the optimal HRT preparation is unknown. Delay in initiation of HRT is associated with lower BMD, smaller uterine size and decreased quality of life. The choice of HRT depends on the cause of POI, need for pubertal induction, need for contraception, comorbidities and patient preference. Some women may prefer a regular withdrawal bleed and thus cyclical therapy (12 to 14 days of added progestogen per month) is appropriate, whereas others may prefer no withdrawal bleeds with a continuous progestogen regimen. A cyclical regimen stimulating active functioning of the endometrium with regular proliferation and withdrawal bleeding may be preferable in women aiming for pregnancy by oocyte donation, with amenorrhoea potentially indicating pregnancy.1
There is evidence that physiological oestradiol confers a greater benefit for BMD compared with ethinylestradiol or conjugated estrogens.15,18,19 Recommended doses for bone protection are at least 2 mg oral estradiol daily or 100 mcg transdermal estradiol weekly or twice weekly.24 Studies in postmenopausal women of typical age indicate that micronised progesterone has advantages in regard to breast cancer and venous thromboembolism risk compared to other progestogens.25,26 Transdermal estradiol with cyclical micronised progesterone most closely approximates ‘body-identical’ HRT. Tibolone and the oral combined preparation of bazedoxifene acetate and conjugated estrogens have not been studied in women with POI.
HRT is not contraceptive. Estradiol-containing combined oral contraceptives (COCs) have not been studied in POI, although may be considered in women desiring contraception for their potential benefit over ethinylestradiol for bone health. Continuous or long cycle use of COCs is preferred to avoid the non-estrogen inactive tablets. The levonorgestrel-releasing intrauterine system used in combination with transdermal estradiol is a good option for women requiring contraception.
Principles for HRT prescription for women affected by POI are similar to those for women experiencing menopause at the usual age. A list of HRT (MHT) preparations available in Australia can be found on the Australasian Menopause Society website (www.menopause.org.au/hp/information-sheets/426-ams-guide-to-equivalent-mht-hrt-doses). The usual contraindications apply, and include current or suspected oestrogen-dependent cancers and active liver, cardiovascular or venous thromboembolic disease. Although the evidence is limited, HRT does not appear to increase breast cancer risk in women with POI, and the risk appears to be less with estrogen alone than with combined estrogen and progestin in studies of postmenopausal women of typical age. BRCA gene mutation carriers can use short-term HRT following prophylactic bilateral salpingo-oophorectomy without an apparent increase in breast cancer risk.27 After the age of 51 years (average age of natural menopause), consideration of whether to use HRT/MHT is the same as for any postmenopausal woman.
There are limited data for the use of testosterone therapy in POI. One small trial in women with Turner syndrome showed that testosterone therapy improved lipid profile, BMD, body composition, cognitive function, quality of life and sexual desire.28 However, studies of women with normal karyotype idiopathic POI indicated that testosterone was no different to placebo for BMD or quality of life.16,29
Karima was advised to use HRT rather than the COC for management of her POI due to her desire for fertility. A cyclical HRT regimen was chosen because the development of amenorrhoea may indicate pregnancy.
What other options can be offered if Karima prefers not to have HRT?
HRT is the best treatment in POI and should be strongly recommended unless there are contraindications. If HRT is contraindicated, nonhormonal options may be considered for vasomotor symptoms. Serotonin noradrenaline reuptake inhibitors, selective serotonin reuptake inhibitors, clonidine, and gabapentin have all been shown to reduce vasomotor symptoms in women with a history of breast cancer (off-label use except for clonidine).30 Cognitive behavioural therapy has been shown to reduce vasomotor symptoms and improve mood, sleep, sexual function and quality of life. Nonhormonal vaginal moisturisers or lubricants can be used for urogenital symptoms.1 Cardiovascular health should be monitored carefully, and referral to an endocrinologist for management of bone health should be considered.
What fertility advice should be given to Karima?
Spontaneous resumption of ovarian activity has been reported in 25% of women with idiopathic POI,31 usually within the first year after diagnosis, with a spontaneous pregnancy rate of 5%.32 Therefore, contraception needs to be considered in the choice of HRT if a woman does not want to become pregnant. However, in the case of desired fertility, women with POI should be referred to a fertility specialist for assessment. Currently, oocyte donation is the best method to achieve a pregnancy.
Karima and her husband were referred to a fertility specialist.
Conclusion
POI can have profound effects on a woman’s physical and psychosocial wellbeing that require multimodal assessment and management. Prompt diagnosis, institution of individualised HRT, psychological support, provision of information and monitoring for long-term sequelae are essential components of management. Referral to psychological, genetic, endocrinology and fertility services may also be required.
References
J Clin Endocrinol Metab 2009; 94: 4820-4827.